The availability of vaccines in the United States has been a pivotal moment in public health history, particularly highlighted during the COVID-19 pandemic. The first COVID-19 vaccines were authorized for emergency use in the U.S. in December 2020, with the Pfizer-BioNTech vaccine receiving approval on December 11, followed by Moderna’s vaccine on December 18. These vaccines marked a significant turning point in the fight against the virus, offering hope and protection to millions. The rollout began with high-risk groups, including healthcare workers and the elderly, and gradually expanded to the general public in early 2021. This rapid development and distribution of vaccines showcased the power of scientific collaboration and innovation in addressing global health crises.
| Characteristics | Values |
|---|---|
| First COVID-19 Vaccine Authorized | December 11, 2020 (Pfizer-BioNTech) |
| Second COVID-19 Vaccine Authorized | December 18, 2020 (Moderna) |
| Third COVID-19 Vaccine Authorized | February 27, 2021 (Johnson & Johnson/Janssen) |
| First Doses Administered | December 14, 2020 |
| Full Approval (Pfizer-BioNTech) | August 23, 2021 |
| Full Approval (Moderna) | January 31, 2022 |
| Pediatric Vaccinations (5-11 years) | November 2, 2021 (Pfizer-BioNTech) |
| Pediatric Vaccinations (6 months-5 years) | June 18, 2022 (Pfizer-BioNTech and Moderna) |
| Booster Shots Authorized | September 22, 2021 (Pfizer-BioNTech for certain groups) |
| Updated (Bivalent) Boosters | August 31, 2022 (Pfizer-BioNTech and Moderna) |
| Vaccines Currently Authorized | Pfizer-BioNTech, Moderna, Novavax (as of October 2023) |
| Total Doses Administered (as of Oct 2023) | Over 670 million doses |
Explore related products






What You'll Learn
![]()
First COVID-19 Vaccine Approval
The first COVID-19 vaccine approval in the United States marked a pivotal moment in the global fight against the pandemic. On December 11, 2020, the U.S. Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) for the Pfizer-BioNTech COVID-19 vaccine, making it the first vaccine available to the American public. This approval came after rigorous clinical trials involving over 43,000 participants, which demonstrated the vaccine’s 95% efficacy in preventing symptomatic COVID-19 infection. The authorization was a testament to the unprecedented speed and collaboration of scientists, regulators, and manufacturers, all working under the umbrella of Operation Warp Speed.
From a practical standpoint, the Pfizer-BioNTech vaccine required a two-dose regimen, administered 21 days apart, with each dose containing 30 micrograms of the mRNA vaccine. Initially, the vaccine was approved for individuals aged 16 and older, though this age range would later expand. Healthcare workers and long-term care facility residents were among the first to receive the vaccine, as they were identified as high-priority groups due to their increased risk of exposure and severe illness. The rollout was a complex logistical challenge, involving ultra-cold storage requirements for the vaccine, which necessitated specialized freezers capable of maintaining temperatures between -80°C and -60°C.
Comparatively, the Pfizer-BioNTech vaccine’s approval set the stage for subsequent authorizations, including Moderna’s mRNA vaccine just one week later. While both vaccines utilized mRNA technology, Pfizer’s earlier approval gave it a head start in distribution. However, Moderna’s vaccine offered slightly more flexibility in storage, requiring temperatures of -20°C, which eased some logistical burdens. The rapid succession of these approvals underscored the urgency of the pandemic and the need for multiple vaccine options to meet global demand.
Persuasively, the first COVID-19 vaccine approval was not just a scientific achievement but a beacon of hope for a weary public. It signaled that the tide could turn against a virus that had upended lives, economies, and societies. Yet, the approval also highlighted the importance of public trust and education. Misinformation and vaccine hesitancy posed significant challenges, necessitating clear communication about the vaccine’s safety, efficacy, and side effects, which were generally mild and short-lived, such as soreness at the injection site, fatigue, or fever.
In conclusion, the first COVID-19 vaccine approval in the United States was a landmark event that combined scientific innovation, regulatory diligence, and logistical coordination. It provided a critical tool in the battle against the pandemic, offering protection to millions and paving the way for a return to normalcy. For individuals, understanding the vaccine’s specifics—from dosage and scheduling to storage and side effects—was essential for informed decision-making. This approval was not just the end of one chapter but the beginning of a new phase in the global response to COVID-19.
Child Allergic to Tdap Vaccine? Understanding Risks and Alternatives
You may want to see also
Explore related products






![]()
Vaccine Distribution Timeline
The first COVID-19 vaccines became available in the United States in December 2020, marking a pivotal moment in the fight against the pandemic. The initial rollout prioritized high-risk groups, including healthcare workers and long-term care facility residents, due to limited supply and the urgent need to protect those most vulnerable to severe illness. This phased approach was guided by recommendations from the Centers for Disease Control and Prevention (CDC) and the Advisory Committee on Immunization Practices (ACIP), ensuring equitable distribution based on risk factors.
By early 2021, eligibility expanded to include older adults, essential workers, and individuals with underlying health conditions. States began opening mass vaccination sites, pharmacies, and community clinics to increase access. The Pfizer-BioNTech vaccine, authorized for individuals aged 16 and older, required two doses administered 21 days apart, while Moderna’s vaccine, for those 18 and older, followed a 28-day interval. Johnson & Johnson’s single-dose vaccine, approved in late February, offered a simpler option, particularly for hard-to-reach populations.
As supply increased, eligibility broadened further in spring 2021, with all adults aged 16 and older becoming eligible by mid-April. Efforts shifted to addressing hesitancy and reaching underserved communities through mobile clinics, partnerships with local organizations, and multilingual outreach. By May, the Pfizer vaccine was authorized for adolescents aged 12–15, followed by approval for children aged 5–11 in late 2021, significantly expanding protection to younger age groups.
Booster shots were introduced in fall 2021 to combat waning immunity and emerging variants. Initially recommended for older adults and immunocompromised individuals, boosters became available to all adults within months. The CDC advised waiting 6 months after the second Pfizer or Moderna dose, or 2 months after the Johnson & Johnson shot. Updated bivalent boosters, targeting both the original virus and Omicron variants, were rolled out in fall 2022, offering enhanced protection against circulating strains.
Practical tips for navigating vaccine distribution included checking state and local health department websites for eligibility and appointment availability, utilizing pharmacy apps for scheduling, and keeping vaccination cards or digital records handy for future doses. Employers and schools often provided on-site clinics, streamlining access for specific populations. Understanding the evolving timeline and guidelines ensured individuals could make informed decisions and contribute to collective immunity.
Israel's Vaccination Rules: Travel Requirements and Restrictions
You may want to see also
Explore related products






![]()
Priority Groups for Vaccination
The COVID-19 vaccine rollout in the United States began in December 2020, with healthcare workers and long-term care facility residents receiving the first doses. As supply increased, the focus shifted to prioritizing groups at higher risk of severe illness or death. This phased approach aimed to maximize the vaccine’s impact while addressing limited initial availability. Understanding these priority groups is crucial for appreciating the strategy behind the rollout and its evolution over time.
Analyzing the Initial Phases: Who Got Vaccinated First?
The Centers for Disease Control and Prevention (CDC) and the Advisory Committee on Immunization Practices (ACIP) identified priority groups based on risk factors. Phase 1a included healthcare personnel (approximately 21 million people) and long-term care facility residents (about 3 million), as they faced the highest exposure and vulnerability. Phase 1b expanded to frontline essential workers (e.g., teachers, grocery store employees) and adults aged 75 and older, totaling roughly 49 million individuals. Phase 1c added adults aged 65–74, those with underlying conditions (e.g., diabetes, heart disease), and other essential workers, covering another 57 million people. This tiered system ensured those most at risk received protection first, reducing hospitalizations and deaths.
Practical Tips for Priority Group Members
If you fell into a priority group, early action was key. Pre-registration through state health department websites or local pharmacies was often required. For example, seniors aged 65+ were advised to use senior-specific vaccination hours or mobile clinics for easier access. Individuals with underlying conditions needed documentation from healthcare providers to verify eligibility in some states. Dosage schedules were critical: Pfizer and Moderna vaccines required two doses, 21 and 28 days apart, respectively, while Johnson & Johnson’s single-dose option offered flexibility for harder-to-reach populations.
Comparing Priority Strategies: Equity vs. Efficiency
The U.S. approach prioritized high-risk groups, but it faced criticism for not explicitly addressing racial disparities early on. For instance, essential workers, who were disproportionately people of color, were not vaccinated until Phase 1b or 1c. In contrast, countries like Israel prioritized age-based rollouts, achieving rapid coverage among older adults. The U.S. eventually shifted to broader eligibility in April 2021, opening vaccines to all adults aged 16+. This shift balanced equity concerns with the practical need to distribute doses quickly as supply increased.
The Takeaway: Lessons from Priority Group Vaccination
The phased rollout demonstrated the importance of data-driven decision-making in public health crises. By targeting high-risk groups first, the U.S. reduced COVID-19 deaths by an estimated 140,000 in the first five months of vaccination. However, the process highlighted challenges in equitable access and communication. Moving forward, vaccine distribution strategies must better integrate social determinants of health to ensure no group is left behind. For individuals, understanding priority criteria and staying informed about eligibility changes remains essential for navigating future health emergencies.
Identifying Vaccination Status in Deceased Individuals: A Comprehensive Guide
You may want to see also
![]()
Vaccine Manufacturers and Types
The COVID-19 pandemic spurred an unprecedented global effort to develop and distribute vaccines, with the United States playing a pivotal role in both manufacturing and deployment. By December 2020, the Pfizer-BioNTech vaccine received emergency use authorization (EUA) from the FDA, marking the first COVID-19 vaccine available in the U.S. This mRNA vaccine, administered in two doses 21 days apart, demonstrated 95% efficacy in clinical trials and was initially prioritized for healthcare workers and high-risk populations. Moderna’s mRNA vaccine followed shortly after, authorized later in December 2020, with a similar two-dose regimen but a longer interval of 28 days. Both vaccines required ultra-cold storage, presenting logistical challenges for distribution.
In contrast to the mRNA vaccines, Johnson & Johnson’s Janssen vaccine, authorized in February 2021, offered a single-dose option, making it a practical choice for hard-to-reach populations. This adenovirus vector-based vaccine had a lower efficacy rate (around 66-72%) compared to its mRNA counterparts but provided strong protection against severe illness and hospitalization. Its ease of storage, requiring only standard refrigeration, further simplified its distribution. These three vaccines formed the backbone of the U.S. vaccination campaign, each addressing different needs and preferences.
Beyond COVID-19, the U.S. has a long history of vaccine manufacturing for diseases like influenza, measles, and polio. Companies like Pfizer, Moderna, and Johnson & Johnson have expanded their expertise to include cutting-edge technologies, such as mRNA platforms, which have revolutionized vaccine development. For instance, the annual flu vaccine, produced by manufacturers like Sanofi Pasteur and GlaxoSmithKline, is updated each year based on global virus surveillance, highlighting the adaptability of vaccine production. Pediatric vaccines, such as those for measles, mumps, and rubella (MMR), are typically administered in two doses, starting at 12-15 months and again between 4-6 years, ensuring lifelong immunity for most recipients.
When selecting a vaccine, factors like age, health status, and vaccine availability play critical roles. For example, the Pfizer-BioNTech COVID-19 vaccine is authorized for individuals aged 6 months and older, while Moderna’s is approved for those 6 months and older but with adjusted dosages for younger age groups. Pregnant individuals are often advised to receive mRNA vaccines due to their safety profile, while those with severe allergies to vaccine components may require alternative options. Practical tips include scheduling appointments during off-peak hours to avoid long waits and keeping a vaccination card handy for future doses or travel requirements.
The diversity of vaccine manufacturers and types underscores the importance of tailored public health strategies. While mRNA vaccines have dominated the COVID-19 response, traditional platforms like adenovirus vectors and protein-based vaccines continue to play vital roles in global health. Understanding these differences empowers individuals to make informed decisions, ensuring broader protection against preventable diseases. As vaccine technology evolves, collaboration between manufacturers, regulators, and healthcare providers will remain essential to meet emerging challenges.
Met Gala and Vaccination: Was It a Must?
You may want to see also
![]()
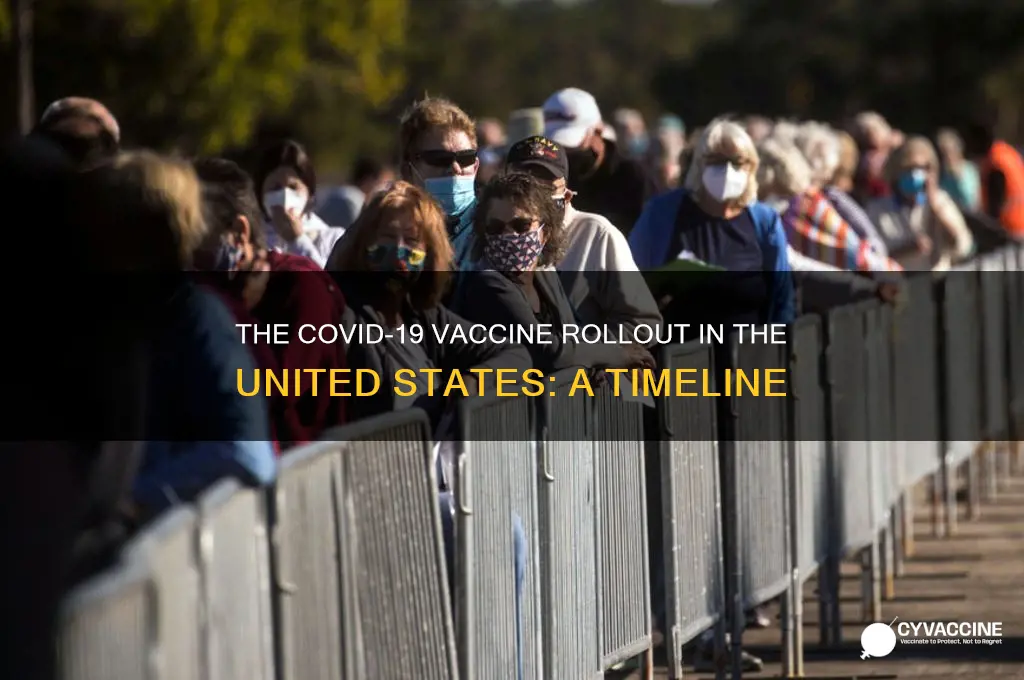
Public Availability and Rollout
The first COVID-19 vaccines became available to the public in the United States in December 2020, marking a pivotal moment in the fight against the pandemic. Initially, distribution was limited to high-risk groups, including healthcare workers and long-term care facility residents, due to constrained supply. This phased approach prioritized those most vulnerable to severe illness and death, ensuring maximum impact with limited doses. The Pfizer-BioNTech vaccine, authorized for individuals aged 16 and older, required two doses administered 21 days apart, while Moderna’s vaccine, approved for those 18 and older, followed a 28-day interval. These early stages laid the groundwork for a broader rollout, balancing urgency with logistical precision.
As production ramped up, eligibility expanded rapidly. By spring 2021, all adults in the U.S. were eligible to receive a vaccine, with states and local jurisdictions managing distribution through pharmacies, hospitals, and mass vaccination sites. The Johnson & Johnson vaccine, authorized in late February, offered a single-dose option, simplifying the process for some populations. However, rollout challenges persisted, including vaccine hesitancy, inequitable access in underserved communities, and logistical hurdles in rural areas. Public health campaigns emphasized the safety and efficacy of the vaccines, addressing misinformation and encouraging uptake across diverse demographics.
The rollout also adapted to emerging data and evolving guidelines. In May 2021, the Pfizer vaccine was authorized for adolescents aged 12 to 15, followed by approval for children aged 5 to 11 in October. Booster shots were introduced later in the year to enhance immunity, particularly for older adults and immunocompromised individuals. These adjustments underscored the dynamic nature of the vaccination effort, responding to new variants and scientific insights. Practical tips for the public included scheduling appointments early, monitoring for side effects (e.g., fatigue, fever), and staying informed about local distribution channels.
Comparatively, the U.S. rollout outpaced many countries, thanks to early investments in vaccine development and a robust distribution infrastructure. However, disparities in access highlighted systemic inequalities, prompting targeted initiatives to reach marginalized communities. Mobile clinics, community partnerships, and multilingual outreach efforts became critical tools in bridging these gaps. The public availability of vaccines not only saved lives but also paved the way for a gradual return to normalcy, demonstrating the power of coordinated public health action.
In retrospect, the rollout of COVID-19 vaccines in the U.S. was a testament to scientific innovation and logistical resilience. From the first doses administered to healthcare workers to the widespread availability for all age groups, the process was marked by adaptability and determination. While challenges remain, the rapid expansion of public access to vaccines stands as a landmark achievement, offering lessons for future public health crises. Practical takeaways include the importance of clear communication, equitable distribution strategies, and flexibility in response to evolving circumstances.
Texas Motor Speedway Vaccine Drive: Which COVID-19 Shot is Being Administered?
You may want to see also
Frequently asked questions
The first COVID-19 vaccine, developed by Pfizer-BioNTech, became available in the United States on December 14, 2020, following emergency use authorization (EUA) by the FDA.
The Moderna COVID-19 vaccine received emergency use authorization (EUA) from the FDA on December 18, 2020, and became available shortly after.
The Johnson & Johnson (Janssen) single-dose COVID-19 vaccine was authorized for emergency use by the FDA on February 27, 2021, and became available soon after.