The Hib vaccine, designed to protect against Haemophilus influenzae type b (Hib), a bacterium causing severe infections like meningitis and pneumonia, was first introduced in the United States in 1985. This marked a significant milestone in public health, as Hib was a leading cause of childhood illness and death before the vaccine's availability. The initial Hib vaccine, known as PRP-D, was followed by more advanced conjugate vaccines in the late 1980s and early 1990s, which offered better protection and were suitable for infants. By the mid-1990s, widespread vaccination led to a dramatic decline in Hib-related diseases, reducing cases by over 99% in the U.S. and transforming the landscape of pediatric health.
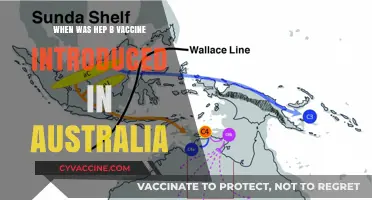
| Characteristics | Values |
|---|---|
| Year Introduced | 1985 (first Hib vaccine approved in the U.S.) |
| Initial Vaccine Type | PRP-D (polyribosylribitol phosphate conjugated to diphtheria toxoid) |
| Manufacturer of First Vaccine | Merck & Co. (marketed as ActHIB) |
| Target Population | Infants and young children (high-risk groups initially) |
| Routine Immunization Recommendation | 1987 (for infants starting at 2 months of age) |
| Impact on Disease | Reduced Hib cases by >99% in the U.S. by the early 1990s |
| Current Vaccine Types | Multiple conjugated Hib vaccines (e.g., ActHIB, PedvaxHIB, Hiberix) |
| Schedule (U.S.) | 2 or 3 doses in infancy, depending on the vaccine brand |
| Booster Dose | Not routinely recommended for healthy children |
| Global Impact | Hib vaccination included in routine immunization programs worldwide |
| Disease Burden Before Vaccine | ~20,000 cases of invasive Hib disease annually in U.S. children |
| Current Disease Incidence | Rare (<1 case per 100,000 children) |
Explore related products






What You'll Learn
- Initial Development: Hib vaccine research began in the 1970s, leading to early formulations
- First Approval: The initial Hib vaccine was licensed in the U.S. in 1985
- Widespread Adoption: Routine childhood immunization with Hib vaccine started in 1987
- Improved Versions: Conjugate Hib vaccines, more effective, were introduced in the late 1980s
- Impact on Disease: Hib cases in the U.S. dropped by 99% post-vaccine introduction
![]()
Initial Development: Hib vaccine research began in the 1970s, leading to early formulations
The 1970s marked a pivotal era in medical research, as scientists turned their attention to Haemophilus influenzae type b (Hib), a bacterium responsible for severe infections in young children. This decade saw the inception of Hib vaccine research, driven by the urgent need to combat diseases like meningitis, pneumonia, and epiglottitis, which disproportionately affected infants and toddlers. Early efforts focused on understanding the bacterium’s polysaccharide capsule, a key component that allowed it to evade the immune system. Researchers hypothesized that a vaccine targeting this capsule could provide effective protection, laying the groundwork for the first Hib vaccine formulations.
One of the critical challenges in early Hib vaccine development was ensuring the vaccine’s immunogenicity in young children. Infants under two years old, who were most vulnerable to Hib diseases, had immature immune systems that often failed to respond adequately to polysaccharide-based vaccines. To address this, scientists pioneered the use of conjugate vaccines, which linked the Hib polysaccharide to a protein carrier. This innovation enhanced the immune response, making the vaccine effective even in very young children. By the late 1970s, initial clinical trials were underway, testing the safety and efficacy of these early formulations.
The first Hib conjugate vaccines were administered in doses tailored to the age of the recipient, typically starting at two months old with additional doses at four and six months, followed by a booster at 12–15 months. These early vaccines demonstrated promising results, significantly reducing Hib-related diseases in trial populations. However, they were not without limitations. Some formulations required larger doses or additional boosters to maintain immunity, and manufacturing complexities posed challenges for widespread distribution. Despite these hurdles, the success of these early vaccines underscored the potential of conjugate technology, setting the stage for further refinements.
A comparative analysis of these initial formulations reveals both their achievements and areas for improvement. For instance, the PRP-D (polysaccharide-diptheria toxoid conjugate) vaccine, one of the earliest to market, effectively reduced Hib meningitis cases by over 90% in vaccinated populations. However, its efficacy waned over time, necessitating booster doses. In contrast, later formulations like PRP-T (polysaccharide-tetanus toxoid conjugate) offered longer-lasting immunity with fewer doses, highlighting the iterative nature of vaccine development. These early successes not only saved countless lives but also established a blueprint for future conjugate vaccines, including those for pneumococcal and meningococcal diseases.
Practical tips for healthcare providers administering early Hib vaccines included careful adherence to dosing schedules and monitoring for rare adverse reactions, such as localized swelling or fever. Parents were advised to keep vaccination records and stay informed about booster requirements. While these early formulations were not perfect, they represented a monumental step forward in pediatric infectious disease prevention. Their development not only addressed a pressing public health crisis but also demonstrated the power of scientific innovation in transforming medical care. By the time the Hib vaccine was formally introduced in the U.S. in the mid-1980s, the groundwork laid in the 1970s had already paved the way for its success.
Skipping Vaccines: The Hidden Risks to Long-Term Health and Wellness
You may want to see also
Explore related products






![]()
First Approval: The initial Hib vaccine was licensed in the U.S. in 1985
The Haemophilus influenzae type b (Hib) vaccine's journey in the United States began with a significant milestone in 1985. This year marked the first approval of a Hib vaccine by the U.S. Food and Drug Administration (FDA), a pivotal moment in the fight against a bacterium that was a leading cause of meningitis and other invasive diseases in young children. The initial vaccine, known as the PRP-D (polyribosylribitol phosphate conjugated to diphtheria toxoid) vaccine, was a breakthrough in pediatric healthcare, offering a new layer of protection for infants and toddlers.
A Game-Changer for Pediatric Health
Before 1985, Hib infections were a formidable threat, particularly for children under five. Meningitis, pneumonia, and epiglottitis were common and often severe outcomes of Hib disease, leading to hospitalizations, long-term disabilities, or even death. The introduction of the Hib vaccine in 1985 was a turning point. It was initially recommended for children aged 18–24 months, with a dosage of 0.5 mL administered intramuscularly. This first-generation vaccine laid the groundwork for future advancements, demonstrating the potential of immunization to drastically reduce the burden of Hib-related illnesses.
Challenges and Improvements
While the 1985 vaccine was a significant step forward, it had limitations. Its effectiveness was lower in infants under 18 months, the age group most vulnerable to Hib disease. This prompted researchers to develop improved versions. By the late 1980s and early 1990s, conjugate Hib vaccines, such as PRP-T (conjugated to tetanus toxoid) and PRP-OMP (conjugated to meningococcal outer membrane protein), were introduced. These vaccines offered better immune responses in younger infants, leading to updated recommendations for a three-dose series starting at 2 months of age, with doses spaced 4–8 weeks apart.
Practical Implementation and Impact
The rollout of the Hib vaccine in 1985 required careful planning and education. Healthcare providers had to ensure parents understood the importance of vaccinating their children, even though Hib disease was less widely recognized than other childhood illnesses. The vaccine’s success was evident within a few years: by the early 1990s, Hib cases in the U.S. had plummeted by over 90%. This dramatic reduction highlighted the vaccine’s effectiveness and set a precedent for the control of other vaccine-preventable diseases.
A Legacy of Prevention
The 1985 approval of the Hib vaccine was more than just a regulatory milestone; it was the beginning of a public health success story. It demonstrated the power of scientific innovation and immunization programs in saving lives. Today, the Hib vaccine is a routine part of childhood vaccination schedules, typically administered in combination with other vaccines to streamline immunization efforts. Its introduction in 1985 remains a testament to the impact of targeted interventions in combating infectious diseases.
Vaccination Rates Among Seniors: How Many Over 80 Are Protected?
You may want to see also
Explore related products






![]()
Widespread Adoption: Routine childhood immunization with Hib vaccine started in 1987
The Hib vaccine's journey to widespread adoption in the United States began in the mid-1980s, but it wasn't until 1987 that routine childhood immunization truly took off. This pivotal year marked a turning point in public health, as the vaccine became a standard part of the childhood immunization schedule. Prior to this, Hib (Haemophilus influenzae type b) was a leading cause of bacterial meningitis and other severe infections in children under 5, claiming thousands of lives annually. The introduction of the Hib vaccine in 1985 was a breakthrough, but its integration into routine care required time, education, and infrastructure adjustments. By 1987, these pieces fell into place, and the vaccine became a cornerstone of pediatric care.
Analyzing the rollout, the success of the Hib vaccine’s widespread adoption in 1987 can be attributed to several factors. First, the vaccine’s efficacy was undeniable: clinical trials demonstrated a 95-100% reduction in invasive Hib disease among vaccinated children. Second, public health campaigns emphasized the vaccine’s safety and the devastating consequences of Hib infections, which included meningitis, pneumonia, and epiglottitis. Pediatricians played a critical role, advocating for the vaccine during well-child visits and ensuring parents understood its importance. The vaccine was administered in a series of doses, typically starting at 2 months of age, with boosters at 4 and 6 months, followed by a final dose between 12 and 15 months. This schedule maximized immunity during the period when children were most vulnerable.
From a practical standpoint, parents and caregivers in 1987 needed clear guidance on what to expect. The Hib vaccine was often combined with other routine immunizations, such as DTaP (diphtheria, tetanus, and pertussis), to minimize clinic visits. Side effects were generally mild, including redness or swelling at the injection site and low-grade fever, but these were far outweighed by the vaccine’s benefits. It’s important to note that the Hib vaccine was not a one-time shot; completing the full series was essential for long-term protection. For families with limited access to healthcare, public health clinics and school-based programs helped bridge the gap, ensuring that socioeconomic barriers did not prevent children from receiving the vaccine.
Comparing the pre- and post-1987 eras highlights the vaccine’s impact. Before widespread adoption, Hib disease affected approximately 20,000 children annually in the U.S., leading to 600 deaths and thousands of cases of permanent disabilities like deafness or developmental delays. By the early 1990s, just a few years after routine immunization began, Hib cases had plummeted by over 99%. This dramatic decline is a testament to the power of vaccination and the importance of timely adoption. The Hib vaccine’s success also paved the way for the introduction of other conjugate vaccines, such as those for pneumococcal disease and meningococcal infections, further reducing childhood mortality and morbidity.
In conclusion, the widespread adoption of the Hib vaccine in 1987 was a landmark achievement in U.S. public health. It transformed the childhood immunization landscape, saving countless lives and preventing severe illnesses. For parents today, the Hib vaccine remains a critical component of the childhood vaccine schedule, a reminder of how far we’ve come in protecting children from once-common, life-threatening diseases. Its story underscores the importance of continued investment in vaccine development, education, and accessibility to safeguard future generations.
Understanding the Administration Code for Pneumococcal Vaccine: A Guide
You may want to see also
Explore related products






![]()
Improved Versions: Conjugate Hib vaccines, more effective, were introduced in the late 1980s
The introduction of the Hib vaccine in the United States marked a significant milestone in the fight against Haemophilus influenzae type b (Hib), a bacterium responsible for severe infections like meningitis and pneumonia. However, the initial polysaccharide-based Hib vaccines, introduced in the early 1980s, had limitations, particularly in young children under two years old, who were most vulnerable to Hib diseases. This age group often failed to mount a robust immune response to these vaccines, leaving them susceptible to infection.
The arrival of conjugate Hib vaccines in the late 1980s revolutionized Hib prevention.
Conjugate vaccines represent a breakthrough in vaccine technology. Unlike their predecessors, which used only the Hib capsule's polysaccharide coating, conjugate vaccines chemically link this polysaccharide to a protein carrier. This ingenious modification allows the immature immune systems of infants to recognize and respond effectively to the Hib antigen. The protein carrier acts as a flag, signaling the immune system to take notice and generate protective antibodies.
This innovation led to a dramatic decline in Hib cases.
The impact of conjugate Hib vaccines was swift and profound. Following their introduction, Hib incidence plummeted by over 90% in the United States. Meningitis cases, once a leading cause of childhood death and disability, became rare. This success story highlights the power of scientific advancement in combating infectious diseases.
Today, conjugate Hib vaccines are a cornerstone of childhood immunization schedules. They are typically administered in a series of doses, starting at two months of age, with boosters given at 12-15 months. This regimen ensures robust immunity during the period of highest vulnerability. The vaccines are safe and well-tolerated, with mild side effects like soreness at the injection site being the most common.
The development and widespread use of conjugate Hib vaccines stand as a testament to the ongoing efforts to protect children from preventable diseases.
Understanding the Duration of Anti-Rabies Vaccine Protection
You may want to see also
Explore related products

![]()
Impact on Disease: Hib cases in the U.S. dropped by 99% post-vaccine introduction
The introduction of the Hib vaccine in the United States in 1985 marked a turning point in the battle against Haemophilus influenzae type b (Hib), a bacterium that once posed a significant threat to young children. Prior to the vaccine, Hib was a leading cause of bacterial meningitis, pneumonia, and epiglottitis, particularly in children under 5 years old. The disease was not only devastating but also highly contagious, spreading through respiratory droplets and causing severe complications that often led to long-term disabilities or death. The Hib vaccine’s arrival was a medical breakthrough, but its true impact became evident in the years that followed.
Analyzing the data reveals a dramatic shift in disease prevalence. Before 1985, the U.S. reported approximately 20,000 cases of invasive Hib disease annually, with a fatality rate of 5%. By the early 1990s, just a few years after the vaccine’s introduction, Hib cases had plummeted by 99%. This reduction was not gradual but swift, demonstrating the vaccine’s efficacy and the success of widespread immunization campaigns. The Centers for Disease Control and Prevention (CDC) recommends the Hib vaccine as part of the routine childhood immunization schedule, with doses administered at 2, 4, and 6 months of age, followed by a booster at 12–15 months. This regimen ensures robust immunity during the period when children are most vulnerable.
The near-eradication of Hib disease in the U.S. underscores the power of vaccination as a public health tool. It also highlights the importance of herd immunity, as high vaccination rates not only protect individuals but also reduce the bacterium’s circulation in the population. However, this success story is not without cautionary notes. In regions with lower vaccination coverage, Hib remains a threat, and sporadic cases still occur in the U.S., often in unvaccinated or undervaccinated children. This serves as a reminder that maintaining high immunization rates is critical to sustaining the gains made against Hib.
From a practical standpoint, parents and caregivers play a vital role in ensuring children receive the Hib vaccine on schedule. Keeping track of immunization records and adhering to the CDC’s recommended timeline are essential steps. Additionally, staying informed about vaccine safety and efficacy can help dispel misinformation and build confidence in the immunization process. For healthcare providers, continued vigilance in monitoring Hib cases and promoting vaccine uptake remains crucial. The story of Hib vaccination is a testament to what can be achieved when science, policy, and community efforts align—a 99% reduction in cases is not just a statistic but a life-saving achievement.
Andrew Cuomo's Vaccine Remarks: Key Statements and Implications
You may want to see also
Frequently asked questions
The Hib vaccine was first licensed and introduced in the United States in 1985.
The Hib vaccine was introduced to prevent Haemophilus influenzae type b (Hib) infections, which were a leading cause of bacterial meningitis, pneumonia, and other severe illnesses in young children.
The initial Hib vaccine introduced in 1985 was highly effective, reducing Hib disease cases by over 90% in vaccinated populations within a few years.
Yes, the Hib vaccine has undergone improvements since 1985. Newer conjugate vaccines, introduced in the late 1980s and early 1990s, provided longer-lasting immunity and were more effective in infants.