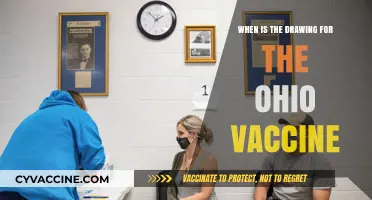
The development of a coronavirus vaccine has been a global priority since the outbreak of COVID-19, with scientists and researchers working tirelessly to create a safe and effective solution. While the typical timeline for vaccine development spans several years, the urgency of the pandemic has accelerated this process, with unprecedented collaboration and funding. Early estimates suggested that a vaccine could be available as early as 12 to 18 months after the virus was first identified, and indeed, by late 2020, several vaccine candidates had entered Phase 3 clinical trials. The earliest approvals and distributions began in December 2020, with vaccines like Pfizer-BioNTech and Moderna leading the way, marking a significant milestone in the fight against the virus. However, the timeline for widespread availability and global distribution continues to evolve, influenced by factors such as manufacturing capacity, regulatory approvals, and equitable access.
| Characteristics | Values |
|---|---|
| Earliest Possible Availability | Late 2024 (for updated vaccines targeting new variants) |
| Current Vaccine Status | Multiple vaccines (e.g., Pfizer, Moderna, AstraZeneca) already approved and widely distributed globally since late 2020/early 2021. |
| Updated Vaccines | Annual or variant-specific updates are being developed and may be available by late 2024 or early 2025. |
| Development Timeline | Typically 10+ years, but expedited to ~1 year for COVID-19 due to global collaboration and funding. |
| Regulatory Approval Process | Emergency Use Authorization (EUA) or full approval by agencies like FDA, EMA, or WHO. |
| Global Distribution Challenges | Uneven distribution, with high-income countries having better access than low-income regions. |
| Variant-Specific Vaccines | Ongoing research to adapt vaccines for new variants (e.g., Omicron subvariants). |
| Booster Recommendations | Periodic boosters recommended to maintain immunity, especially for vulnerable populations. |
| Technologies Used | mRNA (Pfizer, Moderna), viral vector (AstraZeneca, J&J), protein subunit (Novavax), inactivated virus (Sinovac, Sinopharm). |
| Efficacy Against Variants | Varies by variant; updated vaccines aim to improve efficacy against dominant strains. |
| Long-Term Immunity | Studies ongoing; boosters likely needed to sustain protection. |
| Global Vaccination Rates | As of 2023, over 13 billion doses administered globally, but coverage remains uneven. |
Explore related products



$9.99 $9.99

$126.09 $166.95


What You'll Learn
- Preclinical Testing Timeline: Animal trials and safety checks before human trials begin
- Phase 1-3 Trials Duration: Stages of human testing for safety, dosage, and efficacy
- Regulatory Approval Process: Fast-tracked reviews by health agencies for emergency use
- Manufacturing Scale-Up: Mass production challenges and distribution readiness
- Global Collaboration Efforts: International partnerships to accelerate vaccine development
![]()
Preclinical Testing Timeline: Animal trials and safety checks before human trials begin
Before a coronavirus vaccine can even be considered for human trials, it must undergo rigorous preclinical testing to ensure safety and efficacy. This phase is critical, as it lays the groundwork for understanding how the vaccine behaves in living organisms and identifies potential risks before human exposure. Animal trials are the cornerstone of this stage, providing essential data on dosage, immune response, and adverse effects. Typically, small animals like mice or rats are used initially to assess basic safety and immunogenicity, followed by larger animals such as monkeys to evaluate the vaccine’s effectiveness against the virus in a more human-like biological system. These trials are meticulously designed to mimic human exposure as closely as possible, with dosages adjusted for species differences in body weight and metabolism.
One of the key safety checks during preclinical testing is the evaluation of toxicity. Researchers administer the vaccine at various doses to animals, observing for any signs of harm, such as organ damage or systemic reactions. For instance, a vaccine candidate might be tested at doses 10 to 100 times higher than the intended human dose to establish a safety margin. This step is crucial because it helps determine the maximum safe dosage and identifies any long-term effects that might not be immediately apparent. Regulatory agencies like the FDA require comprehensive toxicity data before approving a vaccine for human trials, ensuring that only the safest candidates move forward.
Another critical aspect of preclinical testing is the assessment of immunogenicity—how effectively the vaccine triggers an immune response. In animal trials, researchers measure the production of antibodies and the activation of immune cells after vaccination. For example, a successful vaccine candidate might induce neutralizing antibodies in 80-90% of the test animals, indicating a robust immune response. However, this phase also highlights potential challenges, such as inadequate immunity or the production of non-neutralizing antibodies, which could lead to vaccine failure or even harm in humans. These findings often prompt adjustments to the vaccine’s formulation or delivery method before proceeding.
Despite its importance, preclinical testing is not without limitations. Animal models, while useful, do not perfectly replicate human biology, and results can sometimes be misleading. For instance, a vaccine that works in monkeys might not translate to humans due to differences in immune system responses. Additionally, this phase can be time-consuming, typically lasting 6 to 12 months, depending on the complexity of the vaccine and the number of species tested. Accelerating this timeline without compromising safety is a delicate balance, often achieved through overlapping studies or using advanced technologies like computer modeling to predict outcomes.
In conclusion, preclinical testing is a non-negotiable step in vaccine development, serving as the first line of defense against unsafe or ineffective candidates. By carefully designing animal trials and conducting thorough safety checks, researchers can identify promising vaccines while weeding out those with potential risks. While this phase is lengthy and challenging, it is essential for building public trust and ensuring that only the most viable candidates advance to human trials. Without it, the earliest possible availability of a coronavirus vaccine would be built on shaky ground, risking both health and credibility.
Understanding Your Vaccine Group: A Simple Guide to Find Out
You may want to see also
Explore related products






![]()
Phase 1-3 Trials Duration: Stages of human testing for safety, dosage, and efficacy
The journey from a potential coronavirus vaccine to its widespread availability is a complex process, meticulously designed to ensure safety and efficacy. At the heart of this process are Phase 1-3 clinical trials, each phase serving a distinct purpose and contributing to the overall timeline. Understanding these stages is crucial for anyone eager to know when a vaccine might become available.
Phase 1: Safety First (Typically 2-6 months)
In this initial stage, the vaccine is administered to a small group of healthy volunteers, often 20-100 individuals, to assess its safety profile. Researchers monitor for adverse reactions, such as allergic responses or systemic issues, while also evaluating how the immune system responds. Dosage levels are carefully calibrated, starting with low doses (e.g., 10 micrograms) and escalating gradually to determine the optimal amount that balances safety and immune activation. For example, Moderna’s mRNA-1273 vaccine began Phase 1 with doses of 25, 100, and 250 micrograms, with 250 micrograms later deemed too reactive. This phase is critical for identifying red flags early, ensuring that only safe candidates proceed to larger trials.
Phase 2: Dosage and Immunogenicity (Typically 2-6 months)
With safety established, Phase 2 expands to include several hundred participants, often stratified by age groups (e.g., 18-55 years and 55+ years) to assess variability in response. The focus shifts to refining dosage and confirming immunogenicity—the vaccine’s ability to provoke an immune response. Placebo groups are introduced to compare outcomes, and specific biomarkers, such as neutralizing antibody levels, are measured. For instance, the Oxford-AstraZeneca vaccine’s Phase 2 trial tested doses of 5x10^10 viral particles, ultimately selecting this as the standard dose. This phase also explores whether the vaccine’s effects differ across demographics, a critical factor for global deployment.
Phase 3: Efficacy in Real-World Conditions (Typically 6-12 months)
The largest and most definitive phase, Phase 3, involves thousands to tens of thousands of participants and is designed to prove the vaccine’s efficacy in preventing disease. Participants are randomly assigned to vaccine or placebo groups and monitored over time, often in high-transmission areas to accelerate data collection. For example, Pfizer’s Phase 3 trial enrolled 43,000 volunteers and demonstrated 95% efficacy after two doses (30 micrograms each, administered 21 days apart). This phase also continues to monitor safety, capturing rare side effects that might not appear in smaller trials. The duration can vary depending on infection rates in the study population; faster spread shortens the timeline, while low transmission prolongs it.
Practical Takeaways and Accelerated Timelines
While traditional vaccine development can take 10-15 years, the urgency of the COVID-19 pandemic has compressed Phase 1-3 trials into as little as 12-18 months through unprecedented global collaboration and funding. Overlapping trial phases, such as initiating manufacturing during trials, has further expedited the process. However, shortcuts in testing are not an option—each phase must meet rigorous standards to ensure public trust and safety. For those tracking vaccine progress, understanding these stages provides clarity on why timelines are both ambitious and necessary.
CBC's Vaccine and Booster Recommendations: What You Need to Know
You may want to see also
Explore related products






![]()
Regulatory Approval Process: Fast-tracked reviews by health agencies for emergency use
The race to develop a coronavirus vaccine has been unprecedented, with global efforts accelerating timelines that typically span years. Amid this urgency, regulatory approval processes have adapted to meet the crisis without compromising safety. Health agencies worldwide, including the FDA, EMA, and WHO, have implemented fast-tracked reviews for emergency use authorization (EUA), a mechanism that allows vaccines to reach the public sooner than traditional pathways. This approach balances speed with rigorous evaluation, ensuring that only effective and safe vaccines are approved.
Fast-tracked reviews prioritize vaccines that demonstrate strong efficacy and safety data from clinical trials. For instance, Pfizer-BioNTech and Moderna’s mRNA vaccines were granted EUA in late 2020 after Phase 3 trials involving tens of thousands of participants showed efficacy rates above 90%. These trials included diverse age groups, with specific dosages—typically 30 µg for Pfizer and 100 µg for Moderna—administered in two shots, spaced 3–4 weeks apart. Health agencies scrutinized trial data for adverse effects, ensuring risks were minimal compared to the benefits of protection against severe COVID-19.
One critical aspect of fast-tracked approvals is the reliance on interim data and rolling submissions. Instead of waiting for trials to conclude, manufacturers submit data in real-time as it becomes available. This allows regulators to begin their review process earlier, shaving months off approval timelines. However, this approach requires robust monitoring post-authorization to detect rare side effects that may not appear in initial trials. For example, the rare incidence of myocarditis in young males after mRNA vaccination was identified through post-authorization surveillance, leading to updated guidelines for at-risk populations.
Practical tips for understanding fast-tracked approvals include staying informed through official health agency websites, which often publish detailed summaries of their reviews. For individuals, knowing the specific dosage and administration schedule for each vaccine is crucial, as these can vary. For instance, the AstraZeneca vaccine, approved in many countries, requires a 4–12 week interval between doses, while Johnson & Johnson’s single-dose vaccine offers a simpler regimen. Additionally, being aware of age restrictions—such as Pfizer’s initial approval for ages 16 and up, later expanded to 12 and up—helps in making informed decisions.
In conclusion, fast-tracked reviews by health agencies have been instrumental in expediting coronavirus vaccine availability while maintaining safety standards. By leveraging interim data, rolling submissions, and post-authorization monitoring, regulators have achieved a delicate balance between speed and scrutiny. For the public, understanding the specifics of these approvals—from dosages to age categories—empowers informed decision-making in the fight against the pandemic. This adaptive regulatory framework sets a precedent for future public health crises, demonstrating that urgency and safety can coexist.
Hep A Vaccine: Lifetime Protection or Booster Needed?
You may want to see also
Explore related products






![]()
Manufacturing Scale-Up: Mass production challenges and distribution readiness
The race to produce a coronavirus vaccine has been unprecedented, but developing a safe and effective formula is only half the battle. The real test lies in manufacturing and distributing billions of doses globally, a feat never attempted at this scale or speed. While scientific advancements have accelerated vaccine development, scaling up production and ensuring equitable distribution present unique challenges that could delay widespread immunization.
Consider the logistical nightmare of producing a vaccine requiring ultra-cold storage, like Pfizer’s mRNA vaccine, which must be kept at -70°C. This demands specialized equipment and infrastructure, particularly in low-resource settings. For instance, a single vaccination site might need multiple ultra-low temperature freezers, each costing upwards of $10,000, not to mention the trained personnel to handle such delicate logistics. Contrast this with vaccines like Oxford-AstraZeneca’s, which can be stored at standard refrigerator temperatures (2-8°C), making it far more accessible for mass distribution. The choice of vaccine technology, therefore, directly impacts the feasibility of scale-up and distribution, highlighting the need for a diversified portfolio of vaccine candidates.
Scaling up manufacturing also requires addressing raw material shortages and supply chain bottlenecks. For example, lipid nanoparticles, a critical component of mRNA vaccines, are in limited supply globally. A single dose of an mRNA vaccine requires approximately 30 micrograms of these nanoparticles, and producing billions of doses would strain existing suppliers. Governments and manufacturers must collaborate to secure these materials, potentially through incentives or partnerships, to avoid delays. Additionally, the global nature of vaccine production means that geopolitical tensions or trade restrictions could disrupt supply chains, underscoring the need for regional manufacturing hubs to ensure resilience.
Distribution readiness is equally critical, particularly in reaching vulnerable populations. Vaccines often require multiple doses, such as the two-dose regimen for Pfizer and Moderna vaccines, spaced 3-4 weeks apart. This necessitates robust tracking systems to ensure individuals receive the correct dosage at the right time. In regions with limited healthcare infrastructure, mobile clinics and community health workers could play a pivotal role. For instance, in rural areas, drones have been piloted to deliver medical supplies, a strategy that could be adapted for vaccine distribution. However, such innovations require significant investment and coordination, emphasizing the need for global solidarity in funding and implementing these solutions.
Finally, public trust and acceptance are indispensable for successful distribution. Misinformation about vaccine safety or efficacy can derail even the most meticulously planned rollout. Transparent communication, tailored to local cultures and languages, is essential. For example, in communities with high vaccine hesitancy, engaging trusted figures like religious leaders or healthcare workers can help dispel myths. Practical tips, such as providing clear instructions on side effects and what to expect post-vaccination, can also alleviate concerns. Without addressing these social and behavioral aspects, even the most advanced manufacturing efforts will fall short of their goal.
In summary, while scientific breakthroughs have brought us closer to a coronavirus vaccine, manufacturing scale-up and distribution readiness are the linchpins of global immunization. By addressing logistical, supply chain, and social challenges head-on, we can ensure that vaccines reach those who need them most, marking the beginning of the end of this pandemic.
Pre-Vaccine America: Unveiling the Devastating Health Crises That Shaped the Nation
You may want to see also
Explore related products






![]()
Global Collaboration Efforts: International partnerships to accelerate vaccine development
The race to develop a coronavirus vaccine has highlighted the critical role of global collaboration. International partnerships have emerged as a cornerstone in accelerating vaccine development, leveraging shared resources, expertise, and infrastructure to overcome logistical and scientific hurdles. For instance, the Coalition for Epidemic Preparedness Innovations (CEPI) has coordinated funding and research across multiple countries, enabling parallel clinical trials and manufacturing scale-up. Without such alliances, the timeline for vaccine availability would have stretched far beyond the unprecedented 11-month mark achieved by the Pfizer-BioNTech and Moderna vaccines.
Consider the practical mechanics of these partnerships. Collaborative efforts often involve technology transfer agreements, where vaccine formulations developed in one country are licensed and produced in another. For example, the Oxford-AstraZeneca vaccine, developed in the UK, was manufactured in India by the Serum Institute, the world’s largest vaccine producer. This not only increased global supply but also reduced costs, making doses more accessible to low-income nations. Such partnerships require clear legal frameworks and mutual trust, but the payoff is immense: a single vaccine candidate can reach billions more people, faster.
However, global collaboration is not without challenges. Intellectual property disputes, geopolitical tensions, and unequal distribution of resources can stall progress. Wealthier nations often prioritize their populations, leading to "vaccine nationalism," where doses are hoarded rather than shared. Initiatives like COVAX, a global vaccine-sharing program, aim to address this by pooling funds to procure vaccines for poorer countries. Yet, as of mid-2021, COVAX had delivered only a fraction of its target doses, underscoring the need for stronger political commitment and transparency in these partnerships.
To maximize the impact of international collaborations, stakeholders must adopt a multi-pronged strategy. First, standardize regulatory processes across countries to expedite approvals without compromising safety. Second, invest in local manufacturing capabilities in developing nations to reduce reliance on imports. Third, establish data-sharing platforms to aggregate trial results and identify effective vaccine candidates more swiftly. For instance, the World Health Organization’s Solidarity Trials network has streamlined clinical research by harmonizing protocols across participating countries. These steps, while complex, are essential to ensure that future vaccines are developed and distributed equitably.
Ultimately, the success of global collaboration in vaccine development hinges on a shared sense of urgency and responsibility. The COVID-19 pandemic has demonstrated that no nation can defeat a global health crisis alone. By fostering partnerships that transcend borders, we not only accelerate vaccine timelines but also build a resilient framework for tackling future pandemics. The earliest we could have a vaccine depends not just on scientific innovation, but on our collective willingness to work together.
Crafting a Religious Exemption Vaccination Letter: Essential Elements to Include
You may want to see also
Frequently asked questions
The earliest a coronavirus vaccine could be available for emergency use or limited distribution was projected to be by late 2020 or early 2021, as seen with the Pfizer-BioNTech and Moderna vaccines, which received emergency use authorization in December 2020.
Traditionally, vaccine development takes 10–15 years, but the COVID-19 pandemic accelerated this process through global collaboration, funding, and regulatory fast-tracking, reducing the timeline to under a year for emergency use.
The rapid development was due to unprecedented global cooperation, prior research on related coronaviruses, significant funding, and streamlined regulatory processes, without compromising safety or efficacy standards.
No, the speed did not compromise safety. Clinical trials followed rigorous protocols, and regulatory agencies like the FDA and EMA conducted thorough reviews to ensure the vaccines met safety and efficacy standards before approval.






![Pandemic [DVD]](https://m.media-amazon.com/images/I/91ynbSGeZVS._AC_UL320_.jpg)