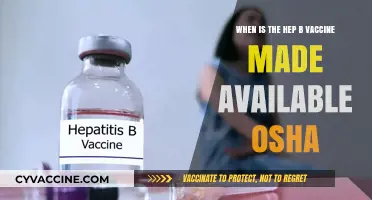
The rollout of the coronavirus vaccine in the United States has been a highly anticipated and closely monitored process, with many Americans eagerly awaiting their turn to receive the shot. As of late 2020, several vaccine candidates had shown promising results in clinical trials, leading to emergency use authorization by the FDA for the Pfizer-BioNTech and Moderna vaccines. The initial distribution began in December 2020, prioritizing healthcare workers and vulnerable populations, with a phased approach to ensure equitable access. The timeline for widespread availability has been influenced by factors such as production capacity, distribution logistics, and public acceptance. While the exact date for when the majority of the population can expect to receive the vaccine has been subject to change, health officials have projected that by mid-2021, a significant portion of Americans could be vaccinated, marking a crucial step toward controlling the pandemic.
| Characteristics | Values |
|---|---|
| Expected Timeline (General) | Late 2020 to early 2021 (initial rollout began in December 2020) |
| First Vaccines Authorized | Pfizer-BioNTech (December 11, 2020) and Moderna (December 18, 2020) |
| Priority Groups for Initial Rollout | Healthcare workers, long-term care facility residents, and elderly adults |
| General Public Availability | Spring 2021 (accelerated by increased production and distribution) |
| Vaccine Types | mRNA vaccines (Pfizer, Moderna), viral vector (Johnson & Johnson) |
| Efficacy Rates | Pfizer: 95%, Moderna: 94.1%, Johnson & Johnson: 66-72% |
| Dosing Requirements | Pfizer: 2 doses (21 days apart), Moderna: 2 doses (28 days apart), J&J: 1 dose |
| Storage Requirements | Pfizer: Ultra-cold (-70°C), Moderna: Standard freezer (-20°C), J&J: Refrigerated (2-8°C) |
| Emergency Use Authorization (EUA) | Granted by FDA for rapid deployment during the pandemic |
| Current Status (as of 2023) | Widely available, including booster shots for variants |
| Manufacturers | Pfizer, Moderna, Johnson & Johnson, Novavax (authorized later) |
| Government Involvement | Operation Warp Speed (U.S. government initiative to accelerate development) |
| Global Distribution | COVAX initiative for equitable distribution worldwide |
Explore related products



$9.99 $9.99



What You'll Learn
- Vaccine Development Timeline: Key milestones in creating and testing COVID-19 vaccines for U.S. distribution
- Emergency Use Authorization: FDA’s role in approving vaccines for rapid public availability
- Distribution Phases: Prioritization of high-risk groups and general population rollout plans
- Manufacturing Capacity: Scaling production to meet U.S. demand and global supply chains
- Public Acceptance: Strategies to address vaccine hesitancy and ensure widespread adoption
![]()
Vaccine Development Timeline: Key milestones in creating and testing COVID-19 vaccines for U.S. distribution
The race to develop a COVID-19 vaccine has been unprecedented, with scientists and regulators working at warp speed to deliver a safe and effective solution. Understanding the key milestones in this process is crucial for grasping the timeline and the rigor involved in bringing a vaccine to the U.S. public. From initial research to emergency use authorization, each phase has been meticulously designed to balance urgency with safety.
Preclinical and Phase 1 Trials (January–June 2020):
Within weeks of the SARS-CoV-2 genome being sequenced in January 2020, researchers began developing vaccine candidates. Preclinical trials in animals tested safety and immune response, while Phase 1 trials in humans focused on dosage and side effects. For example, Moderna’s mRNA-1273 vaccine started Phase 1 trials in March with 45 participants, testing doses of 25, 100, and 250 micrograms. These early trials laid the groundwork for larger studies, demonstrating the vaccine’s potential without compromising safety.
Phase 2 and 3 Trials (July–November 2020):
Phase 2 expanded testing to hundreds of participants to assess efficacy and refine dosage. Pfizer and BioNTech’s BNT162b2 vaccine, for instance, selected a 30-microgram dose after Phase 2. Phase 3 trials involved tens of thousands of volunteers to confirm efficacy and monitor rare side effects. By November 2020, Pfizer reported 95% efficacy in its 43,000-participant trial, while Moderna’s trial of 30,000 participants showed 94.1% efficacy. These results were pivotal in seeking emergency use authorization (EUA) from the FDA.
Emergency Use Authorization (December 2020):
The FDA granted EUA to Pfizer’s vaccine on December 11, 2020, and to Moderna’s on December 18, 2020. This allowed distribution to high-risk groups, such as healthcare workers and the elderly, under strict guidelines. For example, Pfizer’s vaccine required a two-dose regimen, 21 days apart, while Moderna’s doses were administered 28 days apart. This phase highlighted the importance of logistical planning, including ultra-cold storage for Pfizer’s vaccine.
Ongoing Monitoring and Variants (2021–Present):
Post-authorization, the CDC and FDA implemented systems like VAERS (Vaccine Adverse Event Reporting System) and V-safe to monitor side effects. As variants emerged, vaccine manufacturers adapted. Pfizer and Moderna developed booster shots targeting Omicron variants, with the FDA authorizing updated formulations in fall 2022. These efforts underscore the dynamic nature of vaccine development in response to evolving viral threats.
Practical Tips for the Public:
Stay informed about booster recommendations, especially if you’re over 65 or immunocompromised. Schedule vaccinations through local pharmacies or health departments, and keep track of your vaccine card or digital records. For parents, note that Pfizer’s vaccine is approved for children as young as 6 months, with dosages adjusted by age group. Always consult healthcare providers for personalized advice.
This timeline illustrates the remarkable collaboration between scientists, regulators, and manufacturers, ensuring that COVID-19 vaccines met safety standards while addressing a global crisis.
Safe Toddler Detox: Supporting Vaccine Recovery Naturally and Gently
You may want to see also
Explore related products






![]()
Emergency Use Authorization: FDA’s role in approving vaccines for rapid public availability
The FDA's Emergency Use Authorization (EUA) process is a critical mechanism for accelerating the availability of medical products, including vaccines, during public health emergencies. Unlike traditional approval pathways, which can take years, the EUA allows for rapid deployment of potentially life-saving treatments when the benefits outweigh the risks. For the coronavirus vaccine, this process has been pivotal in shortening the timeline from development to distribution, addressing the urgent need to curb the pandemic’s spread. However, the EUA is not a shortcut in safety; it requires manufacturers to submit data from clinical trials demonstrating efficacy and safety, albeit with a focus on expedited review.
To understand the FDA’s role, consider the steps involved in granting an EUA. First, the Secretary of the Department of Health and Human Services (HHS) must declare a public health emergency, which was done for COVID-19 in early 2020. Next, the FDA evaluates the available data, including results from Phase 3 clinical trials, which typically involve tens of thousands of participants. For example, the Pfizer-BioNTech and Moderna vaccines submitted data showing around 95% efficacy in preventing symptomatic COVID-19 in adults. The FDA also assesses manufacturing quality and safety profiles, ensuring that the vaccine meets specific criteria for emergency use. This process, while faster than full approval, still maintains rigorous standards to protect public health.
One key distinction of the EUA is its temporary nature. It remains in effect only as long as the emergency declaration is in place and can be revoked if the vaccine’s risks outweigh its benefits. For instance, the FDA may require additional monitoring, such as tracking adverse events through systems like VAERS (Vaccine Adverse Event Reporting System). Practical tips for the public include understanding that EUA-approved vaccines are thoroughly vetted but may have less long-term data compared to fully approved vaccines. Additionally, dosage instructions, such as the two-dose regimen for Pfizer (30 mcg per dose) and Moderna (100 mcg per dose), are clearly outlined by the FDA to ensure proper administration.
Comparatively, the EUA process highlights the balance between speed and safety. While full FDA approval requires longer-term follow-up data, the EUA allows for immediate distribution based on preliminary evidence. This approach has been instrumental in vaccinating millions of Americans, particularly high-risk groups like healthcare workers and the elderly. For example, the Pfizer vaccine received EUA in December 2020 for individuals aged 16 and older, followed by an expansion to adolescents aged 12-15 in May 2021. This phased rollout demonstrates the FDA’s adaptability in responding to emerging data and evolving public health needs.
In conclusion, the FDA’s Emergency Use Authorization plays a vital role in making coronavirus vaccines rapidly available while maintaining safety standards. By streamlining the approval process without compromising rigor, the EUA has been a cornerstone of the U.S. pandemic response. For the public, understanding this process fosters trust and encourages informed decision-making. As the pandemic continues to evolve, the FDA’s ability to act swiftly yet responsibly remains essential in protecting public health.
Add Alberta Vaccine Records to Apple Wallet: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Distribution Phases: Prioritization of high-risk groups and general population rollout plans
The COVID-19 vaccine distribution in the U.S. is a phased approach, prioritizing those at highest risk of severe illness and death. Phase 1a includes healthcare workers and long-term care facility residents, who received the first doses in December 2020. Phase 1b expands to frontline essential workers and individuals aged 75 and older, while Phase 1c targets those aged 65–74, people with underlying medical conditions, and other essential workers. This tiered strategy ensures that limited vaccine supplies are allocated to those most vulnerable first.
Consider the logistical challenges of this rollout. For instance, the Pfizer-BioNTech vaccine requires ultra-cold storage at -94°F, necessitating specialized equipment and careful handling. In contrast, the Moderna vaccine can be stored at standard freezer temperatures, making it more accessible for rural or less-equipped facilities. Both vaccines require two doses, administered 3–4 weeks apart, emphasizing the need for precise scheduling and patient tracking systems. These details underscore the complexity of distributing vaccines to prioritized groups efficiently.
Persuasively, prioritizing high-risk groups is not just a matter of fairness but of public health strategy. By protecting those most likely to suffer severe outcomes, we reduce hospitalizations and deaths, alleviating strain on healthcare systems. For example, vaccinating 80% of long-term care facility residents could prevent thousands of fatalities. Similarly, shielding essential workers ensures societal functions continue uninterrupted. This phased approach is a critical step toward achieving herd immunity, estimated to require vaccinating 70–85% of the population.
Comparatively, the U.S. distribution plan contrasts with countries like Israel, which rapidly vaccinated a large portion of its population by securing ample doses early. However, the U.S. faces unique challenges, including a larger, more geographically dispersed population and varying state-level implementation. For instance, some states prioritized teachers in early phases, while others focused on age-based thresholds. These differences highlight the need for flexibility and local adaptation in rollout plans.
Practically, individuals should stay informed about their eligibility phase through state health department websites or tools like the CDC’s VaccineFinder. Once eligible, schedule appointments promptly and ensure you receive both doses for full protection. Keep a record of your vaccination card and consider digital tools for tracking. For those in high-risk groups, consult healthcare providers to address concerns or contraindications. Finally, continue adhering to mask-wearing and social distancing until a significant portion of the population is vaccinated, as these measures remain critical during the rollout.
ACL Surgery and COVID-19 Vaccination Requirements
You may want to see also
Explore related products






![]()
Manufacturing Capacity: Scaling production to meet U.S. demand and global supply chains
The U.S. demand for coronavirus vaccines is staggering: hundreds of millions of doses needed within months. Meeting this demand requires a manufacturing scale-up unlike any in history. Existing global vaccine production capacity, even when combined, falls short.
Consider the logistical ballet required. Each vaccine type has unique production needs. mRNA vaccines, like Pfizer-BioNTech's, require specialized lipid nanoparticles and ultra-cold storage, demanding new infrastructure and training. Viral vector vaccines, such as Johnson & Johnson's, rely on cell cultures and bioreactors, necessitating expansions in both facilities and skilled personnel.
Scaling production isn't just about building more factories. It's about securing raw materials, from specialized enzymes to glass vials, in a global market already strained by the pandemic. Supply chains, disrupted by border closures and transportation bottlenecks, must be reconfigured for speed and reliability.
Skipping the 15-Minute Wait Post-Vaccine: Risks and Consequences
You may want to see also
Explore related products






![]()
Public Acceptance: Strategies to address vaccine hesitancy and ensure widespread adoption
The COVID-19 vaccine rollout in the US has been a monumental effort, but its success hinges on public acceptance. Despite widespread availability, vaccine hesitancy remains a significant barrier to achieving herd immunity. Addressing this reluctance requires a multi-faceted approach that combines education, accessibility, and trust-building strategies.
Leveraging Trusted Messengers: One effective strategy is to engage trusted community leaders and healthcare professionals as vaccine advocates. For instance, local doctors, nurses, and religious figures can share their personal experiences with vaccination, dispelling myths and reassuring hesitant individuals. A study by the Kaiser Family Foundation found that 71% of unvaccinated adults trust their personal healthcare provider’s advice about vaccines. Hosting town hall meetings or virtual Q&A sessions with these figures can create safe spaces for dialogue, allowing people to ask questions and receive evidence-based answers. For example, a pediatrician could explain the rigorous testing process of the Pfizer-BioNTech vaccine, which involved 44,000 participants and demonstrated 95% efficacy after two doses administered 21 days apart.
Tailored Messaging for Diverse Audiences: Vaccine hesitancy is not a monolithic issue; it varies across demographics, cultures, and age groups. Tailoring communication strategies to address specific concerns is crucial. For younger adults, emphasizing the vaccine’s role in returning to social activities and protecting loved ones may resonate. For older adults, focusing on the reduced risk of severe illness and hospitalization—such as the 86% efficacy in preventing COVID-19 in those over 65 for the Moderna vaccine—can be persuasive. Additionally, multilingual materials and culturally sensitive campaigns can bridge gaps in understanding, ensuring that messaging is inclusive and accessible.
Addressing Logistical Barriers: Even those willing to get vaccinated may face obstacles like transportation, time constraints, or lack of nearby vaccination sites. Implementing mobile clinics in underserved areas, offering flexible scheduling, and providing incentives such as paid time off for vaccination can alleviate these barriers. For example, pop-up clinics at schools, churches, or workplaces have proven effective in reaching hesitant populations. Furthermore, simplifying the registration process and ensuring clear instructions—such as the need for a second dose of the Pfizer or Moderna vaccines 3–4 weeks after the first—can reduce confusion and increase uptake.
Combating Misinformation with Transparency: Misinformation spreads rapidly, often exploiting fears and uncertainties. Proactive efforts to counter false narratives are essential. Public health agencies can partner with social media platforms to flag and correct misleading content while promoting reliable sources like the CDC or WHO. Fact-checking campaigns that debunk myths—such as the false claim that vaccines alter DNA—can empower individuals to make informed decisions. Transparency about potential side effects, such as mild fever or soreness after receiving a dose, builds trust and reduces anxiety.
By combining these strategies, public health officials can address vaccine hesitancy holistically, ensuring that the coronavirus vaccine reaches as many Americans as possible. The goal is not just to distribute doses but to foster confidence and understanding, turning hesitation into acceptance and protecting communities nationwide.
New York's Vaccine Waste: What's Happening?
You may want to see also
Frequently asked questions
The first COVID-19 vaccines in the US were authorized for emergency use in December 2020, with Pfizer-BioNTech and Moderna vaccines leading the rollout.
Healthcare workers, long-term care facility residents, and high-risk individuals were prioritized for the initial vaccine distribution phases.
The timeline depends on vaccine production, distribution efficiency, and public uptake, but widespread availability was achieved by mid-2021, with ongoing efforts to reach full vaccination coverage.
The COVID-19 vaccine is not federally mandated, but some employers, schools, and organizations may require vaccination as a condition for participation or employment.