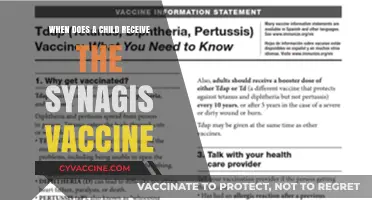
The Centers for Disease Control and Prevention (CDC) in the United States recommends the Measles, Mumps, and Rubella (MMR) vaccine as a critical component of routine childhood immunization. According to the CDC’s guidelines, children should receive the first dose of the MMR vaccine at 12 to 15 months of age, followed by a second dose at 4 to 6 years old, typically before starting kindergarten. This two-dose schedule provides optimal protection against these highly contagious diseases. Additionally, the CDC advises that individuals without evidence of immunity, such as international travelers, healthcare workers, and those in outbreak-prone settings, should also receive the MMR vaccine. The vaccine is safe, effective, and plays a vital role in preventing outbreaks and protecting public health.
| Characteristics | Values |
|---|---|
| Recommended Age for First Dose | 12-15 months |
| Recommended Age for Second Dose | 4-6 years |
| Minimum Interval Between Doses | 28 days |
| Catch-Up Vaccination (Children) | Administer 2 doses, separated by at least 28 days |
| Catch-Up Vaccination (Teens/Adults) | Administer 1-2 doses depending on prior vaccination history |
| Pregnancy Recommendation | Avoid MMR vaccination during pregnancy; defer until after delivery |
| Breastfeeding Recommendation | Safe to administer MMR vaccine to breastfeeding mothers |
| High-Risk Groups | International travelers, healthcare workers, students, and outbreak areas |
| Vaccine Components | Measles, Mumps, and Rubella (live attenuated viruses) |
| Contraindications | Severe allergic reaction to prior dose or vaccine component |
| Precautions | Moderate or severe acute illness, pregnancy, immunocompromised conditions |
| Booster Doses | Generally not needed for immunocompetent individuals |
| Vaccine Brand Names | M-M-R II, Priorix (commonly used in the U.S.) |
| CDC Vaccine Schedule Source | CDC Child & Adult Immunization Schedules |
Explore related products






What You'll Learn
- Recommended Age Schedule: CDC recommends MMR vaccine at 12-15 months and 4-6 years
- Infant Special Cases: High-risk infants may receive MMR as early as 6 months
- International Travel: MMR vaccine advised for travelers to regions with measles outbreaks
- Healthcare Workers: CDC mandates MMR vaccination for all healthcare personnel
- Outbreak Response: Additional MMR dose recommended during measles outbreaks for exposed individuals
![]()
Recommended Age Schedule: CDC recommends MMR vaccine at 12-15 months and 4-6 years
The CDC's recommended age schedule for the MMR vaccine is a carefully crafted strategy to protect children from measles, mumps, and rubella. This two-dose series begins with the first dose administered between 12 and 15 months of age, a critical window when a child's immune system is mature enough to respond effectively to the vaccine. The 0.5 mL dose, typically given subcutaneously, primes the immune system to recognize and combat these highly contagious diseases. This initial dose provides approximately 93% protection against measles, 78% against mumps, and 97% against rubella.
Parents and caregivers should mark their calendars for this first dose, as it sets the foundation for long-term immunity. It’s also a good time to discuss any concerns with a healthcare provider, such as potential mild side effects like fever or rash, which are rare but possible.
The second dose of the MMR vaccine is recommended between 4 and 6 years of age, just before children enter school. This booster dose, also 0.5 mL, significantly increases immunity, raising protection against measles and rubella to about 97% and mumps to around 88%. This timing is strategic, as schools are high-risk environments for disease transmission due to close contact among children. Ensuring children receive this dose before starting kindergarten is a proactive step in preventing outbreaks and protecting both individual children and the broader community.
Adhering to this schedule is crucial, but life sometimes gets in the way. If a child misses the 12-15 month dose, it’s never too late to catch up. Similarly, if the second dose is delayed, it can be given at any age thereafter, with a minimum interval of 28 days between doses. For children traveling internationally or during disease outbreaks, the second dose can be given as early as 4 weeks after the first, though this is an exception to the standard schedule.
Practical tips for parents include scheduling vaccine appointments well in advance, especially during back-to-school seasons when clinics may be busier. Keeping a detailed record of vaccinations is essential, as schools often require proof of immunization. Additionally, combining the MMR vaccine with other routine vaccinations, such as varicella (chickenpox), can streamline the process and reduce the number of visits.
In conclusion, the CDC’s MMR vaccine schedule is designed to maximize protection during the most vulnerable years of childhood. By following this timeline—12-15 months for the first dose and 4-6 years for the second—parents can ensure their children are shielded from serious diseases. This simple yet effective strategy not only safeguards individual health but also contributes to herd immunity, protecting those who cannot be vaccinated due to medical reasons.
When Do I Achieve Full Vaccination Status?
You may want to see also
Explore related products






![]()
Infant Special Cases: High-risk infants may receive MMR as early as 6 months
In certain high-risk scenarios, the CDC allows infants as young as 6 months to receive the MMR vaccine—a notable exception to the standard 12-month recommendation. This early administration is reserved for infants facing heightened exposure risks, such as international travel to measles-endemic areas or during community outbreaks. While this dose provides some protection, it does not count toward the standard two-dose series required for full immunity. Parents must ensure their child receives the first routine dose at 12 months and the second at 4–6 years, regardless of earlier vaccination.
Analytical Perspective: The rationale behind this exception lies in balancing risk versus benefit. Measles, mumps, and rubella pose severe threats to infants, particularly those under 12 months, whose immature immune systems make them highly susceptible. Early vaccination at 6 months leverages the window when maternal antibodies (transferred during pregnancy) begin to wane, allowing the vaccine to elicit a stronger immune response than if administered earlier. However, studies show that up to 25% of infants vaccinated before 9 months may not develop adequate immunity, necessitating the full two-dose series later.
Practical Instructions: For high-risk infants, healthcare providers typically administer a 0.5 mL dose of the MMR vaccine intramuscularly, using the same formulation as older children. Parents should consult a pediatrician or travel medicine specialist at least 4–6 weeks before travel to assess risks and ensure timely vaccination. Documentation of this early dose is critical, as it must be distinguished from the routine schedule to avoid confusion. Providers should use state immunization registries to track doses and ensure adherence to the full series.
Comparative Insight: Unlike the standard MMR schedule, which aligns with routine childhood immunizations, early vaccination for high-risk infants requires individualized assessment. For instance, an infant traveling to a region with a measles outbreak may receive the vaccine at 6 months, while a sibling without travel plans would follow the routine schedule. This tailored approach underscores the importance of context-specific decision-making in pediatric care, contrasting with the one-size-fits-all nature of most vaccine recommendations.
Takeaway for Parents: While the option to vaccinate infants as early as 6 months offers critical protection in high-risk situations, it is not a substitute for the standard MMR series. Parents must remain vigilant about completing all recommended doses to ensure long-term immunity. Proactive communication with healthcare providers is essential to navigate these special cases effectively, ensuring infants receive the right vaccine at the right time without compromising their overall immunization schedule.
Managing Vaccine Reactions: Effective Treatment Strategies and Relief Tips
You may want to see also
Explore related products






![]()
International Travel: MMR vaccine advised for travelers to regions with measles outbreaks
Travelers venturing to regions experiencing measles outbreaks should prioritize receiving the MMR (Measles, Mumps, Rubella) vaccine at least 2–3 weeks before departure to ensure adequate immunity. This pre-travel window allows the body to build sufficient protection, as the vaccine takes time to confer immunity. The CDC recommends this vaccine for international travelers of all ages, with specific guidelines depending on age and vaccination history. Infants as young as 6 months old can receive an early dose if traveling to high-risk areas, though this dose does not replace the routine MMR series starting at 12 months. For adults, two doses are required, with the second dose administered 28 days after the first.
The urgency of this recommendation stems from the highly contagious nature of measles, which spreads through respiratory droplets and can remain airborne for up to two hours. Countries with ongoing outbreaks, such as parts of Africa, Asia, and Europe, pose a significant risk to unvaccinated travelers. Even regions with historically low measles rates may experience sporadic outbreaks due to imported cases, underscoring the importance of vaccination regardless of destination. Travelers should consult a healthcare provider or travel clinic to assess their risk and determine if additional doses are necessary.
A comparative analysis reveals that while routine childhood vaccination schedules in the U.S. typically cover MMR, gaps in immunity can occur due to missed doses or waning protection over time. International travelers, particularly those born after 1957, should verify their vaccination status through medical records or antibody testing. If immunity is uncertain, receiving one or two doses of the MMR vaccine is a straightforward and effective preventive measure. This proactive approach not only protects the individual but also reduces the risk of importing measles to their home country.
Practical tips for travelers include carrying proof of vaccination, such as the International Certificate of Vaccination or Prophylaxis (ICVP), especially when entering countries with strict health regulations. Additionally, practicing good hygiene, such as frequent handwashing and avoiding close contact with sick individuals, complements vaccination efforts. For last-minute travelers who cannot complete the full vaccination series before departure, receiving even a single dose can provide partial protection and reduce the severity of illness if exposure occurs.
In conclusion, the MMR vaccine is a critical tool for safeguarding international travelers against measles, particularly in outbreak-prone regions. By adhering to CDC guidelines, verifying vaccination status, and taking preventive measures, travelers can minimize their risk and contribute to global efforts to control this preventable disease.
Air Traffic Controllers: Vaccination Requirements and Protocols
You may want to see also
Explore related products






![]()
Healthcare Workers: CDC mandates MMR vaccination for all healthcare personnel
The CDC mandates that all healthcare personnel receive the MMR (Measles, Mumps, Rubella) vaccine to protect both themselves and their patients from highly contagious diseases. This requirement is rooted in the critical role healthcare workers play in preventing outbreaks, especially in vulnerable populations such as immunocompromised patients, infants, and the elderly. The CDC recommends two doses of the MMR vaccine, with the first dose administered at 12–15 months of age and the second dose at 4–6 years. However, for healthcare workers who lack documented evidence of immunity or prior vaccination, the CDC advises two doses separated by at least 28 days, regardless of age.
Analyzing the rationale behind this mandate, healthcare settings are high-risk environments for disease transmission due to close patient contact and exposure to infectious agents. Measles, for instance, is so contagious that 90% of unvaccinated individuals near an infected person will contract it. Healthcare workers without MMR immunity not only risk severe illness but also become vectors for spreading these diseases to patients. By ensuring vaccination, the CDC aims to maintain herd immunity within healthcare facilities, reducing the likelihood of outbreaks and safeguarding public health.
Practical implementation of this mandate involves verifying immunity through vaccination records, serologic testing, or documentation of past diseases. For those without proof of immunity, vaccination is the next step. The MMR vaccine is safe and effective, with common side effects limited to soreness at the injection site, mild fever, or rash. Healthcare employers are encouraged to provide on-site vaccination clinics and educate staff about the importance of compliance. Notably, the CDC emphasizes that pregnant healthcare workers should defer MMR vaccination until after delivery, though breastfeeding is not a contraindication.
Comparatively, this mandate aligns with global health standards, as many countries require healthcare workers to be vaccinated against MMR and other preventable diseases. For example, the UK’s National Health Service (NHS) enforces similar policies, reflecting international consensus on the necessity of protecting healthcare environments. In the U.S., this mandate also complements state-level regulations, which often require healthcare workers to meet CDC immunization guidelines. By standardizing MMR vaccination, the CDC ensures consistency across healthcare systems, reducing disparities in infection control practices.
In conclusion, the CDC’s MMR vaccination mandate for healthcare workers is a proactive measure to prevent disease transmission in high-risk settings. By adhering to this requirement, healthcare personnel contribute to a safer environment for patients and colleagues alike. Employers and employees must collaborate to ensure compliance, leveraging available resources such as vaccination programs and immunity testing. Ultimately, this mandate underscores the principle that healthcare workers have a dual responsibility: to heal and to protect.
Daily COVID-19 Vaccination Rates in India: Tracking Progress and Trends
You may want to see also
Explore related products






![]()
Outbreak Response: Additional MMR dose recommended during measles outbreaks for exposed individuals
During a measles outbreak, the CDC recommends an additional dose of the MMR vaccine for exposed individuals who are at risk of infection. This strategy, known as post-exposure prophylaxis (PEP), aims to provide immediate protection to those who may have been exposed to the virus. The key is timing: the MMR vaccine must be administered within 72 hours of exposure to be effective in preventing or mitigating the disease. For those who cannot receive the MMR vaccine, immune globulin (IG) may be considered as an alternative within 6 days of exposure, particularly for high-risk groups such as infants, pregnant women, and immunocompromised individuals.
The rationale behind this recommendation lies in the vaccine’s ability to stimulate a rapid immune response. While the standard MMR schedule provides long-term immunity, an additional dose during an outbreak can offer a critical window of protection for those who may not be fully vaccinated or whose immunity has waned. This is especially important in settings like schools, healthcare facilities, or communities with low vaccination rates, where measles can spread rapidly. The additional dose does not replace the routine MMR schedule but acts as a temporary safeguard during heightened risk periods.
Practical implementation requires swift action and clear communication. Public health officials must identify exposed individuals promptly, assess their vaccination status, and administer the MMR vaccine or IG as appropriate. For children aged 6–11 months, who are typically too young for the first routine MMR dose, an early dose is recommended during an outbreak. However, this dose does not count toward the standard two-dose series, and they will still need the full schedule later. Adults without evidence of immunity (through vaccination records or lab tests) should receive one or two doses, depending on their risk factors.
A critical caution is that the additional MMR dose is not a one-size-fits-all solution. Immunocompromised individuals, pregnant women, and those with severe allergies to vaccine components may require alternative interventions. Additionally, while the MMR vaccine is safe and effective, it is not 100% protective in all cases, particularly when administered outside the 72-hour window. Public health efforts must therefore combine PEP with other measures, such as isolation of infected individuals and vaccination campaigns, to control outbreaks effectively.
In conclusion, the CDC’s recommendation for an additional MMR dose during measles outbreaks is a targeted, evidence-based strategy to protect vulnerable populations. Its success depends on rapid response, accurate risk assessment, and coordinated public health action. By understanding and implementing these guidelines, communities can minimize the impact of measles outbreaks and move closer to eliminating this preventable disease.
Is the Parvo Vaccine a One-Time Shot? What Pet Owners Need to Know
You may want to see also
Frequently asked questions
The CDC recommends the first dose of the MMR vaccine at 12 to 15 months of age.
The CDC recommends the second dose of the MMR vaccine at 4 to 6 years of age, before a child enters kindergarten or first grade.
Yes, the CDC recommends an early dose of the MMR vaccine for infants aged 6 to 11 months who are traveling internationally to areas with measles outbreaks.
Yes, the CDC recommends that adults born after 1956 who have no evidence of immunity or lack written documentation of vaccination should receive at least one dose of the MMR vaccine.
The CDC advises against the MMR vaccine for individuals with severe, life-threatening allergies to any component of the vaccine, pregnant women, and those with severely compromised immune systems.