The varicella vaccine, commonly known as the chickenpox vaccine, is a crucial immunization that protects children from the highly contagious varicella-zoster virus. In the United States, the Centers for Disease Control and Prevention (CDC) recommends a two-dose schedule for the varicella vaccine. The first dose is typically administered between 12 and 15 months of age, while the second dose is given between 4 and 6 years old, often before a child enters kindergarten. This schedule ensures optimal protection against chickenpox, a once-common childhood illness characterized by an itchy rash, fever, and fatigue. By receiving the varicella vaccine according to the recommended timeline, children can significantly reduce their risk of contracting chickenpox and its potential complications, such as bacterial infections, pneumonia, and encephalitis.
| Characteristics | Values |
|---|---|
| Recommended Age (First Dose) | 12–15 months |
| Recommended Age (Second Dose) | 4–6 years (before starting school) |
| Minimum Age for First Dose | 12 months |
| Minimum Interval Between Doses | 3 months (if given earlier, the second dose should be repeated) |
| Vaccine Type | Varicella vaccine (live attenuated virus) |
| Brand Names | Varivax (common brand in the U.S.) |
| Route of Administration | Subcutaneous injection |
| Purpose | Prevention of chickenpox (varicella-zoster virus infection) |
| Effectiveness | ~90% effective after two doses |
| Side Effects | Mild fever, rash, soreness at injection site, temporary joint pain/stiffness |
| Contraindications | Severe immune deficiency, pregnancy, severe allergic reaction to previous dose |
| Catch-Up Vaccination | Children 7–12 years: 2 doses, 3 months apart; ≥13 years: 2 doses, 4–8 weeks apart |
| Global Recommendations | Varies by country; many follow U.S. CDC or WHO guidelines |
| Latest Update (as of 2023) | No significant changes to dosing schedule or recommendations |
Explore related products






What You'll Learn
![]()
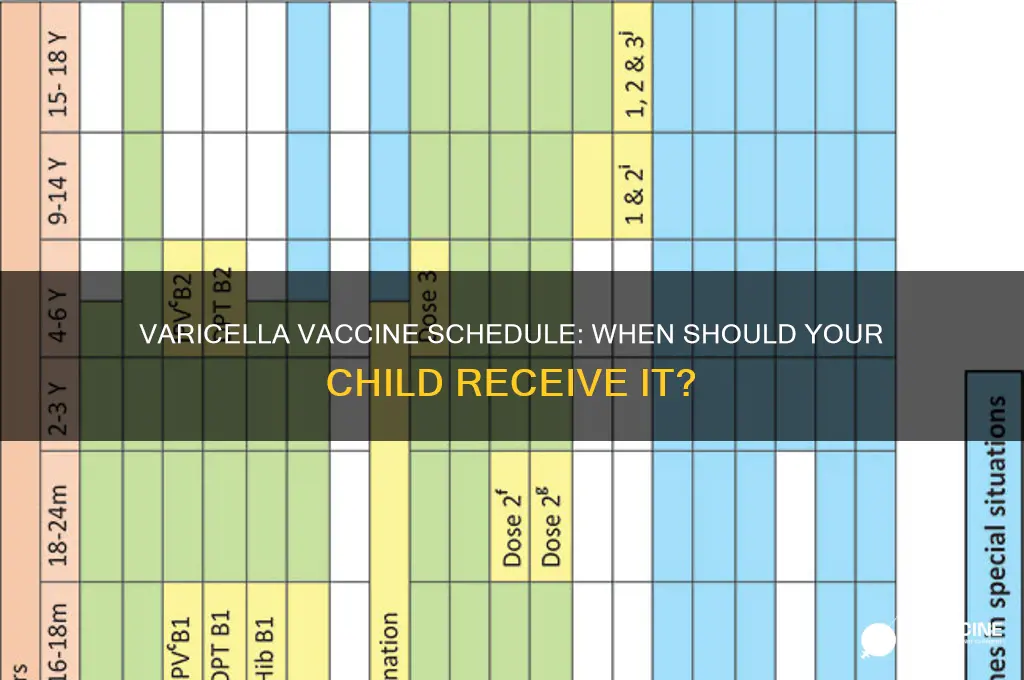
Recommended Age for First Dose
The Centers for Disease Control and Prevention (CDC) recommends that children receive their first dose of the varicella vaccine between 12 and 15 months of age. This narrow age range is strategically chosen to balance the child’s developing immune system with the need for early protection against chickenpox. Administering the vaccine too early may result in a weaker immune response, while delaying it increases the risk of exposure to the virus before immunity is established. This timing aligns with other routine childhood vaccinations, allowing parents and healthcare providers to streamline immunization schedules efficiently.
From a developmental perspective, a child’s immune system at 12 to 15 months is sufficiently mature to mount a robust response to the vaccine. The varicella vaccine contains a live but weakened form of the virus, which stimulates the production of antibodies without causing the disease itself. Studies show that 90% of children who receive the first dose within this age range develop immunity, significantly reducing their risk of severe complications from chickenpox, such as bacterial infections, dehydration, or pneumonia. This age-specific recommendation is a cornerstone of preventive pediatric care, backed by decades of research and clinical practice.
Practical considerations also play a role in this timing. By 12 months, most infants have completed their initial series of vaccines, such as those for measles, mumps, and rubella (MMR), which are often administered at 12 months. Combining the varicella vaccine with other shots during the same visit minimizes the number of clinic trips required, easing the burden on both parents and healthcare systems. However, if a child misses the 12-to-15-month window, the first dose can be given at any time thereafter, ensuring flexibility without compromising long-term protection.
It’s worth noting that the varicella vaccine is not a one-and-done solution. A second dose is recommended between 4 and 6 years of age, typically before a child enters school. This booster dose reinforces immunity, increasing protection to over 95% and reducing the likelihood of breakthrough infections. The two-dose regimen is particularly important in community settings like schools, where close contact can facilitate the spread of the virus. Parents should consult their pediatrician to ensure both doses are administered according to the CDC’s guidelines, as adherence to the schedule maximizes the vaccine’s effectiveness.
For parents, understanding this timeline is crucial for proactive healthcare planning. Marking the 12-month milestone as the target for the first varicella dose can help prevent delays. Additionally, keeping a vaccination record handy ensures that the second dose is not overlooked during the busy preschool years. While side effects from the vaccine are typically mild—such as soreness at the injection site or a mild rash—they are far less severe than the risks associated with natural chickenpox infection. By following the recommended age for the first dose, parents take a significant step in safeguarding their child’s health and contributing to broader community immunity.
Debunking Myths: The Truth About Chips in COVID-19 Vaccines
You may want to see also
Explore related products






![]()
Timing of the Second Dose
The timing of the second dose of the varicella vaccine is a critical aspect of ensuring robust immunity against chickenpox. According to the Centers for Disease Control and Prevention (CDC), the first dose is typically administered between 12 and 15 months of age. The second dose, however, is recommended between 4 and 6 years old, specifically before a child enters kindergarten or first grade. This interval allows the immune system to mature and respond more effectively to the vaccine, enhancing long-term protection.
From an analytical perspective, the spacing between doses is strategically designed to maximize immunogenicity. Studies show that a minimum interval of 3 months between doses is safe, but the 3-year gap commonly observed in the U.S. schedule aligns with school entry requirements and ensures immunity during peak exposure years. For example, if a child receives the first dose at 15 months, the second dose at age 4 would fall within this optimal window. This timing also reduces the risk of breakthrough infections, which, while typically mild, can still occur in vaccinated individuals.
Instructively, parents should consult their child’s healthcare provider to confirm the exact timing of the second dose, as individual health conditions or regional guidelines may influence scheduling. For instance, children with compromised immune systems might require a modified schedule. Practical tips include scheduling the second dose during a routine well-child visit to avoid missed appointments. Additionally, combining the varicella vaccine with other routine immunizations, such as MMR (measles, mumps, rubella), can streamline the process and minimize discomfort for the child.
Comparatively, the U.S. schedule contrasts with some international protocols, where a single dose of varicella vaccine is often sufficient. However, the two-dose regimen has been adopted in the U.S. due to higher efficacy rates, particularly in preventing moderate to severe disease. For instance, one dose provides approximately 85% protection, while two doses increase this to over 98%. This highlights the importance of adhering to the second dose for comprehensive immunity, especially in community settings like schools where the virus spreads easily.
Finally, a persuasive argument for timely administration of the second dose lies in its role in herd immunity. By ensuring that children receive both doses, communities can significantly reduce the circulation of varicella-zoster virus, protecting vulnerable populations who cannot be vaccinated. Parents play a pivotal role in this effort by staying informed and proactive about their child’s immunization schedule. In essence, the second dose is not just a follow-up—it’s a cornerstone of both individual and public health.
Top Booster Options for Johnson & Johnson COVID-19 Vaccine
You may want to see also
Explore related products






![]()
Catch-Up Vaccination Schedule
Children who miss the recommended varicella (chickenpox) vaccine doses at the standard ages of 12–15 months and 4–6 years aren’t permanently unprotected. A catch-up vaccination schedule ensures they can still build immunity against this highly contagious virus. For children aged 7–12 years who haven’t received any doses, the CDC recommends two doses administered 3 months apart. Adolescents 13 years and older require two doses spaced 4–8 weeks apart. This accelerated timeline ensures immunity is established quickly, reducing the risk of infection during outbreaks.
The catch-up schedule isn’t just about age—it’s also about dose spacing. For instance, if a child receives their first dose at age 10, the second dose must follow within 3 months to maximize effectiveness. Parents should consult a healthcare provider to confirm the exact timing, as individual health conditions or previous exposure to varicella may influence the plan. Schools and camps often require proof of vaccination, making adherence to the catch-up schedule critical for compliance and community protection.
One practical tip for parents is to integrate catch-up doses with other routine vaccinations, such as Tdap or HPV, to minimize clinic visits. However, ensure the varicella vaccine isn’t co-administered with other live vaccines unless at least 4 weeks apart, unless using the MMRV combination vaccine, which includes both measles/mumps/rubella and varicella components. This combination is approved for children aged 1–12 years but carries a slightly higher risk of fever and seizures, so discuss the benefits and risks with a healthcare provider.
A common misconception is that older children don’t need the varicella vaccine because chickenpox is a "mild" childhood illness. In reality, complications like bacterial skin infections, pneumonia, and encephalitis can occur at any age. The catch-up schedule isn’t just about individual protection—it contributes to herd immunity, shielding infants too young to be vaccinated and immunocompromised individuals. By adhering to this schedule, families play a vital role in eradicating varicella as a public health threat.
Understanding Vaccine Units: A Comprehensive Guide to Doses and Measurements
You may want to see also
Explore related products


![]()
Vaccine Administration Guidelines
The varicella vaccine, which protects against chickenpox, is typically administered in two doses to ensure robust immunity. The first dose is recommended for children between 12 and 15 months of age, while the second dose is given between 4 and 6 years old, often before entering kindergarten. This schedule aligns with the Centers for Disease Control and Prevention (CDC) guidelines and is designed to maximize protection during early childhood when the risk of exposure is highest. Adhering to this timeline is crucial, as it not only safeguards the child but also contributes to herd immunity, reducing the spread of varicella in communities.
While the recommended schedule is clear, there are exceptions and special considerations. For instance, if a child misses the first dose, it can be administered at any time after 12 months of age, with the second dose following at least 3 months later. This flexibility ensures that children who fall behind can still catch up without compromising immunity. Additionally, adolescents and adults who have never received the vaccine or had chickenpox should also get two doses, spaced 4 to 8 weeks apart. Healthcare providers must assess vaccination history and age to tailor the administration plan effectively.
Proper administration technique is equally important as timing. The varicella vaccine is given as an injection, typically in the deltoid muscle for older children and adults or the thigh muscle for infants and younger children. The dosage remains consistent across age groups: 0.5 mL per dose. It’s essential to use the correct needle length to ensure the vaccine reaches the appropriate muscle tissue, minimizing discomfort and maximizing efficacy. Healthcare professionals should also verify the vaccine’s storage conditions, as it must be kept frozen until reconstitution and then refrigerated to maintain potency.
Practical tips can enhance the vaccination experience for both children and caregivers. Scheduling the appointment during a calm time of day and bringing a favorite toy or book can help distract the child. After the vaccine, mild side effects like soreness at the injection site or a low-grade fever may occur, which can be managed with over-the-counter pain relievers. It’s also important to avoid giving aspirin to children, as it can lead to Reye’s syndrome, a rare but serious condition. Clear communication about what to expect can alleviate anxiety and ensure a smoother process.
In summary, the varicella vaccine’s administration guidelines are straightforward yet require attention to detail. By following the recommended age schedule, addressing exceptions thoughtfully, and employing proper technique, healthcare providers can ensure optimal protection against chickenpox. Caregivers play a vital role in supporting the process, from scheduling to post-vaccination care. Together, these efforts contribute to individual and community health, making the varicella vaccine a cornerstone of pediatric preventive care.
Washington Preschool Vaccine Mandate: Requirements and Compliance Explained
You may want to see also
![]()
Possible Side Effects Post-Vaccination
The varicella vaccine, commonly known as the chickenpox vaccine, is typically administered to children in two doses: the first dose between 12 and 15 months of age, and the second dose between 4 and 6 years. While this vaccine is highly effective in preventing severe cases of chickenpox, it’s essential to understand the possible side effects that may occur post-vaccination. These reactions are generally mild and short-lived, but awareness can help parents and caregivers respond appropriately.
Analytical Perspective:
Most children experience minimal side effects after receiving the varicella vaccine. Common reactions include soreness or swelling at the injection site, mild fever, and a temporary rash consisting of 1–5 blisters. These symptoms typically appear within 1–2 weeks post-vaccination and resolve within a few days. Rarely, some children may develop a more widespread rash resembling chickenpox, but it is usually milder and less contagious. Understanding these outcomes is crucial, as they are the body’s natural response to the vaccine, indicating the immune system is building protection against the varicella-zoster virus.
Instructive Approach:
To manage post-vaccination side effects, parents can follow simple steps. For injection site discomfort, applying a cool, damp cloth and encouraging gentle movement can alleviate pain. Mild fever can be addressed with age-appropriate doses of acetaminophen, but avoid aspirin in children due to the risk of Reye’s syndrome. If a rash develops, keep the area clean and avoid scratching by trimming the child’s nails or using mittens. Monitor the child for unusual symptoms, such as persistent high fever or signs of infection, and consult a healthcare provider if concerns arise.
Comparative Insight:
Compared to the risks of natural chickenpox infection, the side effects of the varicella vaccine are significantly milder. Chickenpox can lead to complications like bacterial skin infections, pneumonia, or encephalitis, particularly in immunocompromised individuals. The vaccine, on the other hand, has a safety profile supported by decades of use, with severe reactions such as allergic responses occurring in fewer than 1 in a million doses. This comparison underscores the vaccine’s role in preventing not only the disease but also its potentially severe complications.
Descriptive Detail:
Imagine a scenario where a 15-month-old receives their first varicella vaccine dose. Within 48 hours, the child may exhibit redness and tenderness at the injection site, accompanied by a low-grade fever of 100.4°F (38°C). By day 3, a small rash with 2–3 blisters appears on the arm, causing mild itchiness. The parent applies a cool compress, administers a child-safe fever reducer, and ensures the child stays hydrated. By day 5, all symptoms have subsided, leaving the child protected against a far more uncomfortable and risky natural infection.
Persuasive Argument:
While side effects post-varicella vaccination can be unsettling, they are a small price to pay for long-term immunity. The vaccine not only protects the individual child but also contributes to herd immunity, reducing the virus’s spread in communities. Parents should weigh the transient discomfort of mild reactions against the lasting benefits of prevention. Open communication with healthcare providers can address concerns and ensure informed decision-making, reinforcing the vaccine’s role as a safe and effective public health tool.
Recommended Age for Mumps Vaccine: A Complete Guide for Parents
You may want to see also
Frequently asked questions
The first dose of the varicella vaccine is typically given to children between 12 and 15 months of age.
Yes, a second dose is recommended for better protection. It is usually administered between 4 and 6 years of age, before a child enters school.
No, the varicella vaccine is not approved for children under 12 months of age. It should be given at the recommended age for safety and effectiveness.
If a child misses the vaccine, they can still receive it at a later age. Catch-up doses can be given, and the schedule may vary depending on the child’s age.
Yes, the varicella vaccine can be administered simultaneously with other routine childhood vaccines, such as MMR (measles, mumps, rubella), unless contraindicated.