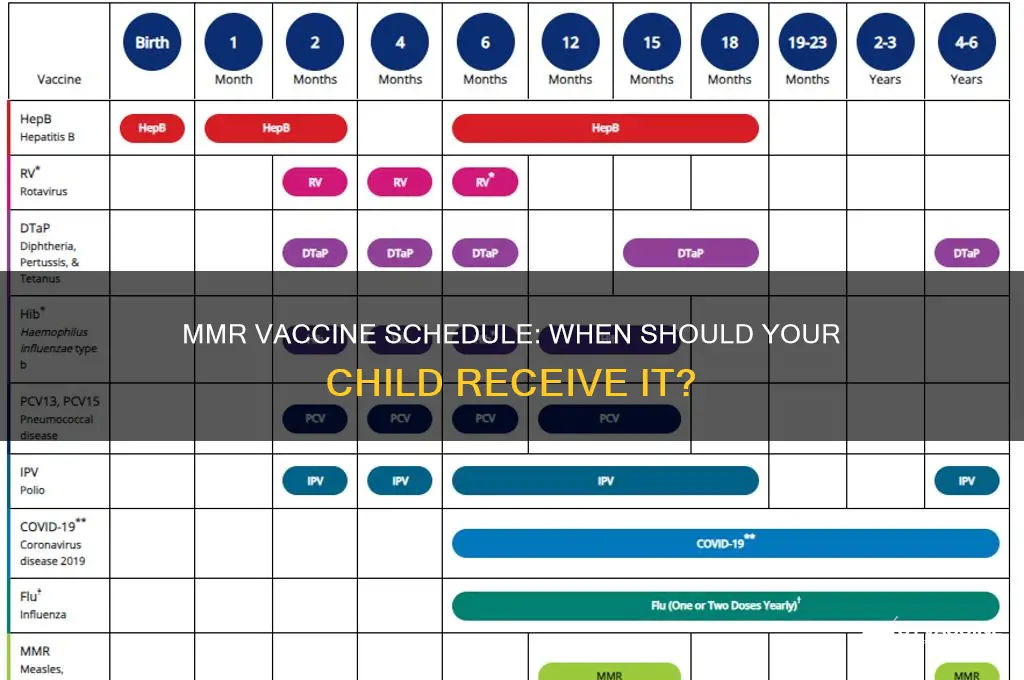
The MMR vaccine, which protects against measles, mumps, and rubella, is a crucial component of childhood immunization schedules worldwide. Typically, children receive their first dose of the MMR vaccine between 12 and 15 months of age, as recommended by health organizations such as the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC). A second dose is then administered between 4 and 6 years of age, often before a child starts school, to ensure full immunity and long-lasting protection against these highly contagious diseases. This two-dose schedule is designed to provide optimal defense against measles, mumps, and rubella, which can have severe complications if contracted.
| Characteristics | Values |
|---|---|
| Recommended Age (First Dose) | 12–15 months |
| Recommended Age (Second Dose) | 4–6 years |
| Vaccine Name | MMR (Measles, Mumps, Rubella) |
| Purpose | Protects against measles, mumps, and rubella |
| Minimum Age for First Dose | 6 months (in special circumstances, e.g., outbreaks or travel) |
| Interval Between Doses | At least 28 days between doses |
| Catch-Up Vaccination | Can be given to older children and adults who missed earlier doses |
| Effectiveness | ~97% effective after two doses |
| Side Effects | Mild fever, rash, soreness at injection site (rare severe reactions) |
| Global Recommendations | Follows WHO and CDC guidelines for routine immunization |
| Booster Dose | Not typically required after two doses |
| Contraindications | Severe allergic reaction to a previous dose or vaccine components |
Explore related products






What You'll Learn
![]()
Recommended Age for First Dose
The MMR vaccine, a cornerstone of childhood immunization, is typically administered in a carefully timed sequence to ensure optimal protection against measles, mumps, and rubella. The first dose is recommended between 12 and 15 months of age, a window chosen to balance the waning of maternal antibodies and the increasing vulnerability to these diseases. This timing is critical because maternal antibodies, which provide passive immunity to newborns, begin to decline around 6 months, leaving infants susceptible to infection. By 12 months, most infants have lost sufficient maternal protection, making this the ideal period to introduce the vaccine.
Administering the MMR vaccine at this age is not arbitrary but rooted in decades of research and clinical trials. Studies show that the immune response to the vaccine at 12–15 months is robust, with seroconversion rates (the development of detectable antibodies) exceeding 95% for measles and mumps and 90% for rubella. This high efficacy ensures that children are well-protected during their early years, a period when exposure to these viruses can have severe, even life-threatening, consequences. For instance, measles can lead to pneumonia, encephalitis, and death, particularly in young children, making timely vaccination a critical preventive measure.
However, there are exceptions to this age recommendation. In certain situations, such as during a measles outbreak or for children traveling to regions with high disease prevalence, the first dose may be given as early as 6 months of age. This earlier dose, known as a "dose zero," provides temporary protection but does not replace the routine 12–15-month dose. Parents should be aware that children who receive the MMR vaccine before their first birthday will still need two additional doses—one at 12–15 months and another at 4–6 years—to ensure long-term immunity.
Practical considerations also play a role in adhering to the recommended age. Pediatricians often schedule the 12–15-month visit to coincide with other routine vaccinations, such as the Hib and pneumococcal vaccines, streamlining the immunization process. Parents should ensure their child’s vaccination record is up to date and communicate any travel plans or outbreak concerns to their healthcare provider. Delaying the MMR vaccine beyond 15 months without a valid medical reason increases the risk of infection, particularly in community settings like daycare or preschool, where diseases spread easily.
In summary, the recommended age for the first dose of the MMR vaccine—12 to 15 months—strikes a balance between immunological readiness and disease risk. While exceptions exist for high-risk scenarios, adhering to this timeline is essential for individual and community protection. Parents and caregivers should work closely with healthcare providers to ensure timely vaccination, safeguarding children against preventable diseases and contributing to broader public health goals.
Vaccinated vs. Unvaccinated: Analyzing Disease-Related Deaths and Outcomes
You may want to see also
Explore related products






![]()
Timing of the Second Dose
The second dose of the MMR vaccine is a critical component in ensuring long-term immunity against measles, mumps, and rubella. Administered typically between the ages of 4 and 6 years, this dose serves as a booster, reinforcing the immune response initiated by the first dose. The timing is strategically planned to coincide with a child’s entry into school, where the risk of exposure to these highly contagious diseases increases significantly. This age range also aligns with the natural waning of maternal antibodies, ensuring the child’s immune system is fully receptive to the vaccine.
From an analytical perspective, the interval between the first and second doses is designed to maximize efficacy. The first dose, given around 12 to 15 months of age, provides initial protection, but studies show that a single dose is approximately 93% effective against measles, 78% against mumps, and 97% against rubella. The second dose elevates these rates to 97% for measles and 88% for mumps, while maintaining high rubella immunity. This significant increase underscores the importance of adhering to the recommended schedule. Deviating from this timeline may leave a child vulnerable during critical developmental years.
Practical considerations for parents include scheduling the second dose during a routine well-child visit to minimize additional trips to the healthcare provider. It’s essential to bring the child’s immunization record to ensure accurate documentation and adherence to local health guidelines. If a child misses the 4-to-6-year window, the vaccine can still be administered later, but delays should be avoided to maintain herd immunity. For families planning international travel, verifying MMR status is crucial, as some countries require proof of vaccination for entry.
Comparatively, the MMR second dose schedule differs from other childhood vaccines, such as those for chickenpox or DTaP, which may have shorter or longer intervals. This uniqueness highlights the tailored approach to vaccine scheduling based on disease epidemiology and immune response dynamics. For instance, the MMR’s second dose is not merely a repeat but a strategic reinforcement, whereas some vaccines require multiple doses to build initial immunity. Understanding this distinction helps parents appreciate the science behind vaccine timelines.
In conclusion, the timing of the second MMR dose is a carefully calibrated step in a child’s immunization journey. It bridges the gap between initial protection and long-term immunity, safeguarding not only the individual but also the community. By adhering to this schedule, parents play a vital role in preventing outbreaks and protecting public health. Clear communication with healthcare providers and proactive planning ensure that this critical dose is administered without delay, securing a child’s health for years to come.
Live Vaccines in the US: Types, Benefits, and Administration
You may want to see also
Explore related products






![]()
Reasons for Delayed Vaccination
In the United States, the Centers for Disease Control and Prevention (CDC) recommends the first dose of the MMR (measles, mumps, rubella) vaccine at 12-15 months of age, with a second dose typically given between 4-6 years. However, various factors can lead to delayed vaccination, potentially leaving children vulnerable to preventable diseases. One common reason is parental hesitancy, often fueled by misinformation about vaccine safety. Despite overwhelming evidence supporting the MMR vaccine's efficacy and safety, myths linking it to autism or other conditions persist, causing some parents to postpone or refuse vaccination. This delay can have serious consequences, as measles outbreaks continue to occur in communities with low vaccination rates.
Another significant factor is logistical barriers, particularly in underserved or rural areas. Limited access to healthcare facilities, transportation challenges, or lack of insurance can make it difficult for parents to adhere to the recommended vaccination schedule. For instance, a child living in a remote area might not receive their first MMR dose until 18 months or later, simply due to the distance to the nearest clinic. Additionally, missed appointments or gaps in medical records can contribute to delays, even when parents are willing to vaccinate.
Medical contraindications also play a role in delayed vaccination. Children with severe allergies to vaccine components, such as gelatin or neomycin, may require alternative schedules or precautions. Similarly, those with compromised immune systems, due to conditions like HIV or cancer treatment, might need to defer the MMR vaccine until their immune status improves. In such cases, healthcare providers must carefully weigh the risks and benefits, sometimes delaying vaccination until the child is medically cleared.
Finally, systemic issues within healthcare systems can inadvertently cause delays. Overburdened clinics, vaccine shortages, or administrative errors can disrupt the timely administration of vaccines. For example, during the COVID-19 pandemic, many routine immunizations were postponed due to lockdowns and resource reallocation, leading to a backlog of unvaccinated children. Addressing these systemic challenges requires coordinated efforts to improve healthcare infrastructure and ensure consistent vaccine availability.
To mitigate delays, parents and caregivers should proactively schedule vaccination appointments, keep detailed immunization records, and stay informed about the importance of timely vaccination. Healthcare providers, meanwhile, can offer flexible scheduling, educate parents about vaccine safety, and leverage reminder systems to reduce missed appointments. By addressing these multifaceted reasons for delayed vaccination, we can better protect children and communities from preventable diseases.
California's Religious Exemption for Vaccines: What's the Law?
You may want to see also
Explore related products






![]()
Possible Side Effects in Children
The MMR vaccine, a cornerstone of childhood immunization, typically begins its administration at 12 to 15 months of age, with a second dose recommended between 4 and 6 years. While its efficacy in preventing measles, mumps, and rubella is well-documented, understanding its potential side effects is crucial for informed decision-making. Most children experience mild reactions, if any, but awareness empowers parents to respond appropriately.
Mild Reactions: The Common Companions
Within 24 hours of vaccination, some children may develop a fever, often around 101°F (38.3°C), accompanied by soreness at the injection site. A transient rash, resembling mild measles, can appear 7 to 10 days post-vaccine. These symptoms, though unsettling, are short-lived, typically resolving within 2 to 3 days. Administering acetaminophen as directed by a pediatrician can alleviate discomfort, but aspirin should be avoided in children due to its association with Reye’s syndrome.
Moderate Concerns: When to Monitor Closely
Rarely, children may experience more pronounced reactions, such as a high fever (above 103°F or 39.4°C) or persistent crying for over 3 hours. Swollen glands or temporary joint stiffness, more common in adolescent girls and adult women, may also occur. These symptoms warrant observation but are generally not cause for alarm. However, if a fever persists beyond 48 hours or is accompanied by unusual lethargy, consulting a healthcare provider is essential.
Severe but Rare: The Critical Few
Serious side effects are exceedingly rare, occurring in fewer than 1 in 1 million doses. These include severe allergic reactions (anaphylaxis), characterized by difficulty breathing, swelling of the face, or rapid heartbeat, which require immediate medical attention. Very rarely, seizures caused by fever (febrile seizures) may occur in 1 out of every 3,000 to 4,000 doses. While frightening, these seizures are typically brief and do not lead to long-term neurological issues.
Practical Tips for Parents
To minimize discomfort, ensure your child is well-rested and hydrated before vaccination. After the shot, encourage gentle movement to ease injection site pain. Keep a digital thermometer handy to monitor fever accurately. Document any reactions, no matter how minor, to share with your pediatrician during follow-up visits. Remember, the MMR vaccine’s benefits in preventing life-threatening diseases far outweigh its minimal risks, making it a vital step in safeguarding your child’s health.
Exploring Vaccine Options for Colorectal Cancer Recurrence Prevention
You may want to see also
Explore related products






![]()
Importance of MMR Vaccine Schedule
The MMR vaccine, a cornerstone of childhood immunization, protects against measles, mumps, and rubella—diseases once commonplace but now largely preventable. Administered in two doses, the first at 12-15 months and the second at 4-6 years, this schedule is meticulously designed to maximize immunity during critical developmental stages. Deviating from this timeline can leave children vulnerable during outbreaks, as seen in recent measles resurgences linked to vaccine hesitancy.
Consider the biological rationale: the first dose primes the immune system, typically conferring 93% effectiveness against measles. The second dose acts as a booster, raising immunity to 97% and closing gaps for the 2-5% who didn’t respond initially. This two-tiered approach mirrors strategies for other vaccines like varicella, but the MMR’s timing is uniquely calibrated to avoid maternal antibody interference, which can neutralize the vaccine in infants under 12 months.
Logistically, adherence to the schedule reduces healthcare burden. Schools often require proof of the first dose for enrollment, while the second dose aligns with kindergarten entry—a natural checkpoint for compliance. Parents can streamline this by scheduling the second dose during the 4-6 year well-child visit, often paired with other boosters like DTaP. Pro tip: Use vaccine reminder apps or set calendar alerts to avoid delays, as missed doses require careful recalibration by a pediatrician.
Critics of rigid schedules argue for flexibility, but the MMR’s timing is non-negotiable for herd immunity. Measles, for instance, remains one of the most contagious pathogens, spreading through coughs up to two hours after exposure. A single unvaccinated child can trigger outbreaks in communities with vaccination rates below 95%. Historical data from the 2019 measles outbreak in the Pacific Northwest underscores this—78% of cases occurred in unvaccinated individuals, many of whom were eligible for the MMR but hadn’t received it.
Finally, the schedule accommodates catch-up scenarios. Children who miss the first dose at 12 months can receive it anytime thereafter, with the second dose separated by at least 28 days. For international travel to measles-endemic regions, infants 6-11 months may receive an early dose, though this doesn’t replace the standard series. Always consult a healthcare provider to tailor the schedule to individual needs, ensuring no child falls through the cracks of preventable disease.
Who Monitors Vaccine Safety? Understanding the Agency's Role and Responsibilities
You may want to see also
Frequently asked questions
The first dose of the MMR vaccine is usually administered when a child is 12 to 15 months old.
Yes, a second dose of the MMR vaccine is recommended and is typically given when the child is 4 to 6 years old, before they enter school.
Yes, the MMR vaccine can be given as early as 6 months of age in certain situations, such as during a measles outbreak or for international travel, but this dose does not replace the routine doses at 12-15 months and 4-6 years.
If a child misses the recommended MMR vaccine schedule, they can still receive the vaccine at a later age. It’s important to consult a healthcare provider to catch up on missed doses as soon as possible.