The recommendation for the hepatitis A vaccine began to take shape in the early 1990s, following the development and approval of the first effective vaccines against the virus. In 1996, the Centers for Disease Control and Prevention (CDC) in the United States issued its initial guidelines, suggesting vaccination for high-risk groups, such as international travelers, men who have sex with men, and individuals with chronic liver disease. By 1999, the CDC expanded its recommendations to include routine vaccination of children living in states with the highest rates of hepatitis A. This shift marked a significant milestone in public health, as it aimed to reduce the incidence of the disease and its associated complications. Over time, as the vaccine proved safe and effective, recommendations were further broadened to include all children starting at age 1, as well as adults at risk, solidifying its role as a critical preventive measure against hepatitis A.
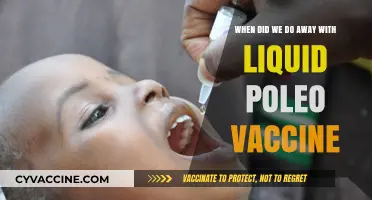
| Characteristics | Values |
|---|---|
| First Recommendation (USA) | 1996 (CDC recommended routine vaccination for children in high-risk areas) |
| Universal Pediatric Recommendation (USA) | 2006 (CDC expanded recommendation to all children aged 12-23 months) |
| Adult Recommendation (USA) | 1999 (CDC recommended for high-risk adults, later expanded to include travelers and certain groups) |
| Global Adoption | Varies by country; many adopted recommendations in the late 1990s to early 2000s |
| Vaccine Availability | First hepatitis A vaccines became available in the early 1990s |
| Target Groups | Children, travelers, men who have sex with men, people with chronic liver disease, and those in high-risk settings |
| Dosage Schedule | Typically 2 doses, 6-18 months apart, depending on the vaccine brand |
| Effectiveness | Over 95% effective in preventing hepatitis A infection |
| Impact on Disease Incidence | Significant decline in hepatitis A cases in countries with widespread vaccination |
| Current Status | Routine vaccination recommended in many countries, including the USA, EU, and others |
Explore related products






What You'll Learn
![]()
Early vaccine development milestones
The journey toward recommending the hepatitis A vaccine began with a series of critical milestones in vaccine development. The first inactivated hepatitis A vaccine was licensed in Europe in 1991, marking a turning point in preventing this highly contagious liver infection. This initial approval set the stage for global adoption, with the United States following suit in 1995 after rigorous clinical trials demonstrated its safety and efficacy. Administered in a two-dose series, typically at 0 and 6 to 12 months, this vaccine achieved over 95% seroprotection in recipients, a game-changer for public health.
One of the most significant milestones was the identification of hepatitis A virus (HAV) in 1973, which laid the groundwork for vaccine development. Researchers cultivated the virus in cell cultures, enabling the creation of an inactivated vaccine. This breakthrough was pivotal, as earlier attempts to develop a vaccine were hindered by the inability to isolate the virus. By the late 1980s, clinical trials were underway, targeting high-risk groups such as travelers to endemic regions and individuals with chronic liver disease. These trials confirmed the vaccine’s ability to prevent infection, even in those exposed to the virus.
The shift from recommending the vaccine only for high-risk groups to universal childhood immunization was another critical milestone. In 1999, the United States began recommending routine hepatitis A vaccination for children in states with the highest disease rates. By 2006, this recommendation expanded nationwide for all children aged 12 to 23 months. This decision was driven by data showing that vaccinating children not only protected them but also reduced community transmission, a concept known as herd immunity. The vaccine’s success in these programs led to a 95% decline in hepatitis A cases in the U.S. by 2014.
Practical considerations also played a role in early vaccine development. The vaccine’s stability at room temperature for up to one month made it accessible in resource-limited settings, though it is typically stored refrigerated. Additionally, its compatibility with other childhood vaccines streamlined immunization schedules. For adults, a single dose provides short-term protection, while the full two-dose series offers long-term immunity. Travelers were among the first to benefit from these advancements, as the vaccine became a standard recommendation for those visiting regions with high HAV prevalence.
In retrospect, the early milestones in hepatitis A vaccine development exemplify the power of scientific innovation and public health strategy. From virus isolation to universal immunization, each step addressed specific challenges, transforming a once-common infection into a preventable disease. Today, the vaccine stands as a testament to how targeted research and policy can reshape global health outcomes. For parents, travelers, and healthcare providers, understanding this history underscores the importance of adhering to vaccination schedules and staying informed about evolving recommendations.
Harvard's COVID-19 Vaccination Policy Explained
You may want to see also
Explore related products






![]()
Initial CDC recommendations timeline
The Centers for Disease Control and Prevention (CDC) first introduced recommendations for the hepatitis A vaccine in the early 1990s, marking a significant shift in public health strategy. Initially, the vaccine was targeted at high-risk groups, including international travelers to endemic areas, men who have sex with men, and individuals with chronic liver disease. This selective approach aimed to curb outbreaks and protect those most vulnerable to severe complications. By 1996, the CDC expanded its guidelines to include children living in communities with consistently elevated rates of hepatitis A, recognizing the vaccine’s potential to reduce community-wide transmission.
A pivotal moment came in 1999 when the CDC’s Advisory Committee on Immunization Practices (ACIP) recommended routine hepatitis A vaccination for all children aged 2 years and older in 17 states with the highest disease rates. This decision was based on data showing that targeted vaccination in these areas could significantly decrease the overall disease burden. The vaccine, administered in a two-dose series with a 6-month interval, proved highly effective in preventing infection and reducing asymptomatic transmission. This phased rollout allowed health officials to monitor the vaccine’s impact before broader implementation.
By 2006, the CDC extended its recommendation for routine hepatitis A vaccination to all children aged 12–23 months nationwide, regardless of geographic location. This shift reflected the vaccine’s success in high-risk states and the growing recognition of hepatitis A as a preventable disease. The two-dose regimen remained standard, with the first dose given at age 1 and the second dose administered 6–18 months later. This universal recommendation aimed to establish herd immunity and eliminate hepatitis A as a public health threat in the United States.
Practical implementation of these recommendations required collaboration between healthcare providers, schools, and public health agencies. Parents were encouraged to adhere to the vaccination schedule, and catch-up doses were recommended for older children and adolescents who had not previously been vaccinated. The CDC also emphasized the importance of vaccinating adults at risk, including those with occupational exposure or underlying health conditions. This comprehensive approach ensured that the vaccine’s benefits reached all age groups and risk categories.
In retrospect, the CDC’s initial recommendations for the hepatitis A vaccine demonstrate a strategic, data-driven approach to disease prevention. By starting with high-risk groups and gradually expanding to universal childhood vaccination, the agency maximized the vaccine’s impact while minimizing logistical challenges. Today, these early guidelines serve as a foundation for ongoing efforts to maintain low hepatitis A incidence rates and protect public health. For individuals unsure about their vaccination status, consulting a healthcare provider for a simple blood test or catch-up doses remains a practical and effective step.
Vaccinated vs. Unvaccinated: Who Fared Better?
You may want to see also
Explore related products






![]()
Global health organizations' adoption dates
The World Health Organization (WHO) first recommended hepatitis A vaccination in 1999, targeting high-risk groups in countries with intermediate to high endemicity. This initial guidance focused on travelers to endemic areas, men who have sex with men, and individuals with chronic liver disease. The recommendation was based on the growing availability of effective vaccines and the recognition of hepatitis A as a significant public health burden in certain regions. WHO’s strategic approach prioritized cost-effectiveness, advocating for vaccination campaigns in areas where the disease was most prevalent and impactful.
By contrast, the Centers for Disease Control and Prevention (CDC) in the United States began recommending hepatitis A vaccination for children in 1996, starting with those living in states with the highest disease rates. This recommendation was expanded in 1999 to include all children aged 12–23 months, with catch-up vaccination for older children. The CDC’s decision was driven by data showing that routine childhood immunization could reduce hepatitis A incidence dramatically, as evidenced by declines of over 90% in states implementing the vaccine early. The recommended dosage for children is a two-dose series, with the first dose administered at age 1 and the second 6–18 months later.
The European Centre for Disease Prevention and Control (ECDC) adopted a more tailored approach, leaving vaccination decisions to individual member states based on local epidemiology. Countries like Italy and Spain, with higher hepatitis A incidence, introduced universal childhood vaccination in the early 2000s, while others prioritized at-risk groups. This decentralized strategy reflects Europe’s diverse disease landscape, where vaccination policies must balance regional needs with resource allocation. Travelers from low-endemic European countries are often advised to receive the vaccine before visiting high-risk areas, with a single dose providing short-term protection and a second dose ensuring long-term immunity.
In low- and middle-income countries, adoption has been slower due to cost and competing health priorities. Gavi, the Vaccine Alliance, began supporting hepatitis A vaccination in eligible countries in 2019, offering financial assistance for vaccine introduction. This initiative targets nations with high disease burden and feasible delivery systems, such as those already implementing routine immunization programs. Practical considerations, like maintaining the vaccine’s cold chain and integrating it into existing health services, are critical for successful rollout in resource-limited settings.
A comparative analysis reveals that global health organizations’ adoption dates reflect both disease burden and economic feasibility. While WHO and CDC prioritized early implementation in high-risk populations, ECDC’s decentralized model and Gavi’s recent support highlight the importance of context-specific strategies. For individuals, understanding these recommendations underscores the need to consult local health guidelines and consider personal risk factors, such as travel plans or occupational exposure, when deciding on vaccination.
Puppy Vaccinations: What's Needed Before Selling?
You may want to see also
Explore related products





![Vaccines, The Biggest Medical Fraud In History [Graphically enhanced, Student Loose Leaf Facsimile Book with 30 Color Pages. Rev. 5]](https://m.media-amazon.com/images/I/81cgEWRFStL._AC_UY218_.jpg)
![]()
Pediatric vaccination schedule introduction
The hepatitis A vaccine was first licensed in the United States in 1995, but its integration into the pediatric vaccination schedule was a gradual process. Initially, the vaccine was recommended for high-risk groups, such as international travelers, men who have sex with men, and individuals with chronic liver disease. However, as the vaccine's safety and efficacy became well-established, public health officials began to consider its broader application. By 1999, the Centers for Disease Control and Prevention (CDC) recommended routine hepatitis A vaccination for children living in communities with the highest rates of the disease. This marked a significant shift in strategy, as it introduced the concept of population-based immunity through pediatric vaccination.
Analyzing the evolution of the pediatric vaccination schedule reveals a careful balance between disease prevalence and vaccine availability. For hepatitis A, the decision to include it in the routine schedule was influenced by several factors, including the vaccine's cost-effectiveness and the potential for herd immunity. In 2006, the CDC expanded its recommendation to include all children aged 12–23 months, regardless of geographic location. This change was driven by data showing that widespread vaccination could reduce the overall incidence of hepatitis A, even in areas with low disease rates. The schedule typically involves two doses, administered at least 6 months apart, with the first dose given around the child's first birthday. This timing ensures that children are protected during their early years, when they are most likely to encounter the virus through close contact with others.
From a practical standpoint, introducing the hepatitis A vaccine into the pediatric schedule requires coordination between healthcare providers and parents. Pediatricians play a crucial role in educating families about the importance of this vaccine, addressing concerns about safety, and ensuring timely administration. For example, parents should be informed that the vaccine is highly effective, with studies showing over 95% seroprotection after two doses. Additionally, the vaccine can be administered simultaneously with other routine childhood immunizations, such as MMR or varicella, simplifying the vaccination process. However, providers must also be aware of contraindications, such as severe allergic reactions to previous doses or vaccine components, and adjust the schedule accordingly.
Comparing the hepatitis A vaccine to other pediatric immunizations highlights its unique position in the schedule. Unlike vaccines for diseases like measles or polio, which have been routine for decades, the hepatitis A vaccine is a relatively recent addition. This novelty can sometimes lead to hesitancy among parents, who may question its necessity. To address this, healthcare providers can emphasize the vaccine's role in preventing a highly contagious disease that, while rarely fatal, can cause severe symptoms and long-term complications, especially in older children and adults. Moreover, the vaccine's inclusion in the schedule reflects a broader shift toward proactive public health measures, aiming to prevent diseases before outbreaks occur rather than reacting to them.
In conclusion, the introduction of the hepatitis A vaccine into the pediatric vaccination schedule exemplifies the dynamic nature of immunization policies. From its initial recommendation for high-risk groups to its current status as a routine childhood vaccine, this evolution underscores the importance of adapting public health strategies to new evidence and changing disease landscapes. For parents and providers, understanding the rationale behind this schedule ensures that children receive the maximum benefit from vaccination, contributing to both individual and community health. By staying informed and following the recommended guidelines, we can continue to protect future generations from preventable diseases.
Adults Missing Critical Vaccinations: Are You Up to Date?
You may want to see also
Explore related products






![]()
Travel-related vaccine advice history
The history of travel-related vaccine advice is a testament to how global mobility has shaped public health recommendations. In the mid-20th century, as international travel became more accessible, health authorities began issuing guidelines for diseases like cholera and yellow fever. However, it wasn’t until the 1990s that hepatitis A emerged as a significant concern for travelers, particularly those visiting regions with poor sanitation. This shift marked a turning point in travel medicine, as hepatitis A vaccination transitioned from a niche recommendation to a standard preventive measure.
Analyzing the timeline reveals a pattern of reactive and proactive measures. Initially, hepatitis A vaccine recommendations were limited to high-risk groups, such as travelers to developing countries or individuals with occupational exposure. The vaccine, first licensed in the U.S. in 1995, was initially administered in a two-dose series, with the second dose given 6 to 12 months after the first. By the early 2000s, as data on the vaccine’s efficacy and safety grew, health organizations like the CDC expanded their advice to include all travelers to endemic areas, regardless of age or health status.
A comparative look at global practices highlights regional differences in adoption. While North America and Europe swiftly integrated hepatitis A vaccination into travel advice, other regions were slower to follow. For instance, some Asian countries prioritized vaccines for diseases like typhoid fever, reflecting local disease burdens. This disparity underscores the importance of tailoring travel vaccine recommendations to both destination-specific risks and individual traveler profiles.
Practical tips for travelers have evolved alongside these recommendations. Today, the hepatitis A vaccine is typically given in a two-dose series, with the second dose administered 6 to 18 months after the first, depending on the formulation. Accelerated schedules are available for last-minute travelers, though efficacy may be slightly reduced. Combining hepatitis A vaccination with other travel vaccines, such as typhoid or hepatitis B, is now common practice, streamlining preparation for multi-destination trips.
In conclusion, the history of travel-related hepatitis A vaccine advice reflects broader trends in global health and travel medicine. From its initial focus on high-risk groups to its current status as a routine recommendation, this vaccine exemplifies how disease prevention strategies adapt to changing travel patterns and epidemiological data. For modern travelers, staying informed about destination-specific risks and adhering to vaccination schedules remains a cornerstone of safe international travel.
Vaccination Requirements in Denver: What You Need to Know
You may want to see also
Frequently asked questions
The CDC first recommended the hepatitis A vaccine in 1996 for specific high-risk groups, such as travelers to endemic areas, men who have sex with men, and individuals with chronic liver disease.
In 1999, the CDC’s Advisory Committee on Immunization Practices (ACIP) recommended routine hepatitis A vaccination for children living in states or communities with the highest rates of hepatitis A. By 2006, this recommendation was expanded to all children aged 12–23 months nationwide.
The WHO began recommending the hepatitis A vaccine in 1997, particularly for countries with intermediate to high endemicity, as part of comprehensive prevention strategies.
The CDC recommended the hepatitis A vaccine for food handlers in the early 2000s, following outbreaks linked to contaminated food. Healthcare workers were also advised to receive the vaccine if they were at increased risk of exposure.
The hepatitis A vaccine was included in routine adult vaccination recommendations in the early 2000s, particularly for adults with specific risk factors, such as international travelers, people with clotting-factor disorders, and those experiencing homelessness.