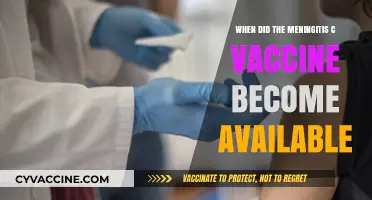
The hepatitis B vaccine, a groundbreaking development in the fight against viral hepatitis, became commercially available in 1981, marking a significant milestone in public health. Developed by Dr. Baruch Blumberg and his team, this vaccine was the first to prevent a major human cancer (hepatocellular carcinoma) by targeting a viral infection. Initially created using purified hepatitis B surface antigen from the blood of infected individuals, the vaccine was later produced through recombinant DNA technology in yeast, ensuring greater safety and efficacy. Its introduction revolutionized hepatitis B prevention, reducing the global burden of chronic liver disease and liver cancer, and setting a precedent for the development of other viral vaccines.
| Characteristics | Values |
|---|---|
| First Availability | 1981 (Plasma-derived vaccine) |
| Recombinant Vaccine Availability | 1986 |
| FDA Approval (Recombinant) | 1986 |
| Global Use Expansion | 1990s (widely adopted in national immunization programs) |
| WHO Recommendation | 1992 (included in routine infant immunization schedules) |
| Combination Vaccines | Late 1990s (e.g., with hepatitis A, DTaP, etc.) |
| Current Status | Widely available globally, part of standard vaccination schedules |
| Key Manufacturers | Merck (Recombivax HB), GlaxoSmithKline (Engerix-B), others |
| Vaccine Type | Recombinant DNA vaccine |
| Target Population | Infants, adolescents, high-risk adults |
| Dosing Schedule | Typically 3 doses over 6 months (0, 1, 6 months) |
| Efficacy | >95% protection against hepatitis B infection |
| Long-term Immunity | At least 20-30 years, often lifelong |
| Adverse Effects | Generally mild (soreness, fever) |
| Global Impact | Significant reduction in hepatitis B prevalence worldwide |
Explore related products






What You'll Learn
- Initial Development: Early research and trials leading to the first hepatitis B vaccine
- First Approval: The year and country where the vaccine was first officially approved
- Global Rollout: Timeline of vaccine availability in different regions worldwide
- Key Milestones: Significant advancements in vaccine technology and accessibility
- Impact on Public Health: Reduction in hepatitis B cases post-vaccine introduction
![]()
Initial Development: Early research and trials leading to the first hepatitis B vaccine
The journey to the first hepatitis B vaccine began in the 1960s, spurred by the discovery of the Australia antigen (later identified as the hepatitis B surface antigen) by Baruch Blumberg and colleagues. This breakthrough laid the groundwork for understanding the virus and its potential prevention. Early research focused on isolating and purifying the surface antigen, which would eventually serve as the key component of the vaccine. By the late 1960s, scientists recognized that this antigen could stimulate an immune response, offering a glimmer of hope for a vaccine.
In the 1970s, the first trials of a hepatitis B vaccine began, using plasma from chronic carriers as the source of the antigen. These early vaccines, though effective, raised safety concerns due to the risk of transmitting blood-borne pathogens. To address this, researchers turned to recombinant DNA technology, a revolutionary approach at the time. In 1976, the first recombinant hepatitis B vaccine was produced by inserting the gene for the surface antigen into yeast cells, allowing for mass production of a safer, purified antigen.
Clinical trials of the recombinant vaccine commenced in the early 1980s, targeting high-risk groups such as healthcare workers and individuals with hemophilia. These trials demonstrated the vaccine’s efficacy, with a typical dosage regimen of three intramuscular injections over six months (0, 1, and 6 months). The vaccine induced protective antibody levels in over 90% of recipients, marking a significant milestone in infectious disease prevention. By 1981, the first hepatitis B vaccine, known as Hepatitis B Vaccine (Heptavax B), was approved for use in the United States, though it was later replaced by safer recombinant versions.
The development of the hepatitis B vaccine was not without challenges. Ensuring consistent antigen purity, optimizing dosage schedules, and addressing public skepticism about vaccine safety were critical hurdles. However, the success of these early efforts paved the way for global immunization programs, reducing hepatitis B prevalence dramatically. Today, the vaccine is administered to infants within 24 hours of birth in many countries, a testament to the foresight and perseverance of those early researchers. Their work not only saved millions of lives but also set a precedent for the development of other viral vaccines.
Debunking Myths: The Truth About Chips in COVID-19 Vaccines
You may want to see also
Explore related products






![]()
First Approval: The year and country where the vaccine was first officially approved
The hepatitis B vaccine's journey to global availability began with a pivotal moment in 1981, when the United States became the first country to officially approve its use. This groundbreaking development marked a turning point in the fight against a virus that had long been a significant public health concern. The vaccine, initially developed by Dr. Maurice Hilleman and his team at Merck & Sons, was a recombinant DNA product, a technological marvel at the time. It was the first vaccine created using genetic engineering techniques, showcasing the potential of modern biotechnology in medicine.
This initial approval was specifically for the plasma-derived vaccine, which was recommended for high-risk groups, including healthcare workers, individuals with multiple sexual partners, and those with a history of sexually transmitted infections. The dosage regimen typically involved a series of three intramuscular injections, administered over a period of several months. For adults, the standard dose was 20 micrograms, while children received a reduced dose based on their age and weight. This targeted approach ensured that those most vulnerable to the virus were protected first, a strategic move to maximize the vaccine's impact.
The United States' approval set a precedent for other countries to follow suit, but it also highlighted the challenges of global vaccine accessibility. While the U.S. and other developed nations began implementing vaccination programs, many low-income countries faced barriers to access due to cost and distribution logistics. This disparity in availability became a critical issue, as hepatitis B disproportionately affected regions with limited healthcare resources. The initial approval, therefore, was not just a scientific achievement but also a call to action for global health equity.
In the years following the U.S. approval, the vaccine's reach expanded, and by the late 1980s and early 1990s, many countries had incorporated it into their national immunization programs. The World Health Organization (WHO) played a crucial role in this expansion, recommending the vaccine for all infants and promoting its inclusion in routine childhood immunization schedules. This shift from targeted high-risk groups to universal vaccination was a significant strategy change, aiming to prevent hepatitis B transmission at its source.
The first approval of the hepatitis B vaccine in the United States in 1981 was a milestone in medical history, demonstrating the power of scientific innovation to combat infectious diseases. It also underscored the importance of equitable access to vaccines, a lesson that continues to resonate in global health initiatives today. As we reflect on this achievement, it serves as a reminder that the development of a vaccine is just the beginning; ensuring its availability to all who need it is the ultimate goal.
Walk-In Vaccination Essentials: Your Must-Have Checklist for a Smooth Visit
You may want to see also
Explore related products






![]()
Global Rollout: Timeline of vaccine availability in different regions worldwide
The hepatitis B vaccine, a cornerstone of modern preventive medicine, began its global rollout in the early 1980s, but its availability varied widely across regions due to economic, logistical, and policy differences. Developed in 1981 by Dr. Maurice Hilleman and his team at Merck, the first hepatitis B vaccine was a plasma-derived product. By 1986, a safer recombinant DNA version became available, marking a pivotal shift in vaccine accessibility and efficacy. However, the journey from laboratory to widespread distribution was far from uniform.
In high-income countries like the United States, Canada, and Western Europe, the vaccine was introduced into routine immunization schedules by the late 1980s and early 1990s. For instance, the U.S. recommended the vaccine for infants in 1991, with a three-dose series typically administered at birth, 1–2 months, and 6–18 months. These regions prioritized at-risk groups, such as healthcare workers and individuals with multiple sexual partners, before expanding to universal childhood vaccination. The availability of resources and robust healthcare infrastructure facilitated rapid adoption, significantly reducing hepatitis B prevalence in these areas.
In contrast, low- and middle-income countries faced delays due to cost, supply chain challenges, and competing public health priorities. The World Health Organization (WHO) endorsed the hepatitis B vaccine for global use in 1992, but many countries in Africa, Asia, and Latin America did not introduce it into their national immunization programs until the late 1990s or early 2000s. For example, China, a country with a high burden of hepatitis B, began nationwide infant vaccination in 2002, while some African nations relied on Gavi, the Vaccine Alliance, for financial support to implement the vaccine. These disparities highlight the critical role of international partnerships in bridging the gap between vaccine development and equitable access.
Regional variations also emerged in vaccine formulations and schedules. In resource-limited settings, a reduced two-dose schedule (at birth and 6 months) was often adopted to maximize coverage with limited supplies. This approach, endorsed by the WHO, proved effective in preventing mother-to-child transmission, a major route of infection in endemic areas. Meanwhile, some countries, like France, initially targeted adolescents and adults due to the vaccine’s high cost, only later shifting to infant immunization. These adaptations underscore the flexibility required to tailor vaccine strategies to local contexts.
Today, the hepatitis B vaccine is available in over 180 countries, with global coverage among infants reaching approximately 84% as of 2021. However, challenges persist, particularly in reaching underserved populations and maintaining high vaccination rates. Practical tips for ensuring vaccine effectiveness include adhering to the recommended schedule, storing vaccines at 2–8°C to maintain potency, and integrating hepatitis B vaccination with other routine immunizations to improve uptake. The global rollout of the hepatitis B vaccine serves as a testament to the power of scientific innovation and international collaboration, while also reminding us of the ongoing need to address disparities in access and implementation.
Understanding Sterile Diluent for Feline FVRC Vaccine Administration
You may want to see also
Explore related products






![]()
Key Milestones: Significant advancements in vaccine technology and accessibility
The hepatitis B vaccine, a cornerstone of modern preventive medicine, became commercially available in 1981, marking a pivotal moment in the fight against viral hepatitis. This milestone was the culmination of decades of research, beginning with the discovery of the hepatitis B virus (HBV) in 1965 by Dr. Baruch Blumberg. The vaccine’s development was revolutionary, as it was the first to be produced using recombinant DNA technology, a breakthrough that paved the way for safer, more efficient vaccine production. Initially, the vaccine was derived from the blood of chronic carriers, but the shift to a yeast-based, genetically engineered version in the 1980s eliminated the risk of blood-borne contamination, making it accessible to a global population.
One of the most significant advancements in vaccine technology was the introduction of combination vaccines, which streamlined immunization schedules and improved compliance. In 1996, the hepatitis B vaccine was combined with the diphtheria, tetanus, and pertussis (DTaP) vaccine, creating a single shot that protected against multiple diseases. This innovation was particularly beneficial for infants, who could now receive protection against HBV as part of their routine vaccinations starting at birth. The recommended schedule for infants includes a dose at birth, followed by doses at 1–2 months and 6–18 months, ensuring early and comprehensive immunity.
Accessibility to the hepatitis B vaccine has expanded dramatically since its inception, thanks to global health initiatives like the World Health Organization’s (WHO) Expanded Programme on Immunization (EPI). By 2009, over 170 countries had incorporated the hepatitis B vaccine into their national immunization programs, reaching an estimated 79% of infants worldwide. This widespread adoption has led to a significant decline in HBV prevalence, particularly in regions with high infection rates such as Asia and Africa. For example, in China, where chronic HBV infection once affected 10% of the population, vaccination efforts have reduced the rate to less than 1% among children under 5.
Despite these successes, challenges remain in ensuring equitable access to the vaccine. Cost, infrastructure limitations, and vaccine hesitancy continue to hinder full coverage in some low-income countries. To address these barriers, organizations like Gavi, the Vaccine Alliance, have played a critical role in subsidizing vaccine costs and strengthening healthcare systems in underserved regions. Additionally, the development of thermostable vaccine formulations, which do not require constant refrigeration, has improved distribution in areas with limited cold chain infrastructure.
Looking ahead, ongoing research aims to further enhance vaccine efficacy and accessibility. Novel delivery methods, such as needle-free injections and oral vaccines, are being explored to simplify administration and reduce costs. Moreover, efforts to integrate hepatitis B vaccination with other health services, such as maternal and child health programs, could maximize reach and impact. As we reflect on the journey of the hepatitis B vaccine, it is clear that continued innovation and collaboration are essential to achieving a world free from the burden of this preventable disease.
Vaccination and MSG: What's the Connection?
You may want to see also
Explore related products

![Vaccines, The Biggest Medical Fraud In History [Graphically enhanced, Student Loose Leaf Facsimile Book with 30 Color Pages. Rev. 5]](https://m.media-amazon.com/images/I/81cgEWRFStL._AC_UY218_.jpg)




![]()
Impact on Public Health: Reduction in hepatitis B cases post-vaccine introduction
The hepatitis B vaccine, first approved for use in 1981, marked a turning point in the fight against a virus that causes chronic liver disease, cirrhosis, and liver cancer. Its introduction was a significant milestone in public health, offering a preventive measure against a highly contagious and potentially deadly infection. The vaccine's impact on reducing hepatitis B cases is a testament to the power of immunization programs.
A Dramatic Decline in Cases
Following the vaccine's availability, public health initiatives focused on targeted vaccination campaigns. Initially, high-risk groups such as healthcare workers, infants born to infected mothers, and individuals with multiple sexual partners were prioritized. This strategic approach led to a substantial decrease in acute hepatitis B cases. For instance, in the United States, the incidence rate plummeted from 8.5 cases per 100,000 population in 1987 to 1.1 cases per 100,000 in 2017, a remarkable 87% reduction. This success story is not limited to the US; global efforts have resulted in an estimated 84% decline in new infections between 1990 and 2015, according to the World Health Organization (WHO).
Vaccine Efficacy and Schedule
The hepatitis B vaccine is highly effective, providing over 90% protection against the virus when the full series is administered. The standard schedule involves three doses: the initial dose, followed by a second dose one month later, and a third dose five months after the second. This regimen ensures long-term immunity, with studies showing that protection lasts for at least 20 years in healthy individuals. For newborns, the vaccine is typically given within 24 hours of birth, followed by two to three additional doses in the first year, providing a crucial early defense against the virus.
Global Impact and Challenges
The introduction of the hepatitis B vaccine has had a profound global impact, particularly in regions with high disease prevalence. In China, for example, a nationwide vaccination program led to a 97% reduction in chronic infections among children under 5 years old between 1992 and 2006. However, challenges remain. Ensuring access to the vaccine in low-resource settings and maintaining high coverage rates are essential to sustaining these public health gains. The WHO's goal of eliminating viral hepatitis as a public health threat by 2030 relies heavily on continued vaccination efforts and addressing disparities in access.
Long-Term Benefits and Future Directions
The reduction in hepatitis B cases post-vaccine introduction has far-reaching consequences. It not only prevents acute infections but also significantly lowers the risk of chronic liver diseases and liver cancer, reducing the burden on healthcare systems. Moreover, the success of the hepatitis B vaccine has paved the way for the development and implementation of other viral hepatitis vaccines, such as hepatitis A and E. As research advances, the potential for therapeutic vaccines and improved formulations offers hope for even greater control of hepatitis B and other infectious diseases.
In summary, the availability of the hepatitis B vaccine has led to a dramatic decline in cases, demonstrating the critical role of immunization in public health. Its impact extends beyond immediate infection prevention, contributing to long-term liver health and reducing the global burden of liver-related diseases. Continued efforts to improve vaccine accessibility and coverage are vital to sustaining and building upon these achievements.
Whooping Cough Vaccine: Is It Covered by Medicare?
You may want to see also
Frequently asked questions
The first hepatitis B vaccine was approved for use in 1981, developed by Dr. Maurice Hilleman and his team at Merck.
Yes, the first hepatitis B vaccine (Heptavax B) was derived from the blood of donors with high levels of hepatitis B surface antigen.
The recombinant DNA hepatitis B vaccine, which is safer and more widely used today, became available in 1986.
In the United States, the hepatitis B vaccine was recommended for routine infant immunization in 1991.
The hepatitis B vaccine was included in the World Health Organization’s (WHO) Expanded Programme on Immunization (EPI) in 1992, making it widely accessible globally.