As of the latest updates, the timeline for when all adults are due to be vaccinated against COVID-19 varies by country and region, largely depending on vaccine availability, distribution strategies, and local health priorities. Many developed nations have already achieved widespread vaccination coverage for their adult populations, with some now focusing on booster shots and vaccinating younger age groups. However, in many low- and middle-income countries, vaccine access remains limited, delaying the goal of full adult vaccination. Global initiatives like COVAX aim to accelerate equitable distribution, but challenges such as supply chain issues and vaccine hesitancy persist. As a result, the target date for vaccinating all adults worldwide remains uncertain, with estimates ranging from late 2023 to 2024 or beyond.
Explore related products






What You'll Learn
- Vaccine Rollout Timeline: Phased distribution plans and estimated completion dates for adult vaccination globally
- Priority Groups: Criteria for prioritizing adults based on age, health, and occupation
- Vaccine Availability: Supply chain challenges and production rates affecting adult vaccination schedules
- Booster Shots: Timing and eligibility for additional doses to maintain immunity in adults
- Global Disparities: Variations in adult vaccination timelines across countries due to resource differences
![]()
Vaccine Rollout Timeline: Phased distribution plans and estimated completion dates for adult vaccination globally
The global vaccine rollout has been a complex, phased process, with countries adopting diverse strategies to prioritize populations and manage distribution. Most nations began by vaccinating high-risk groups—healthcare workers, the elderly, and those with comorbidities—before expanding to younger adults. For instance, the U.S. and U.K. initially targeted individuals over 65 and frontline workers, while India prioritized those above 45. These early phases were critical in reducing severe outcomes and hospital burdens, but they also highlighted logistical challenges, such as supply chain bottlenecks and vaccine hesitancy.
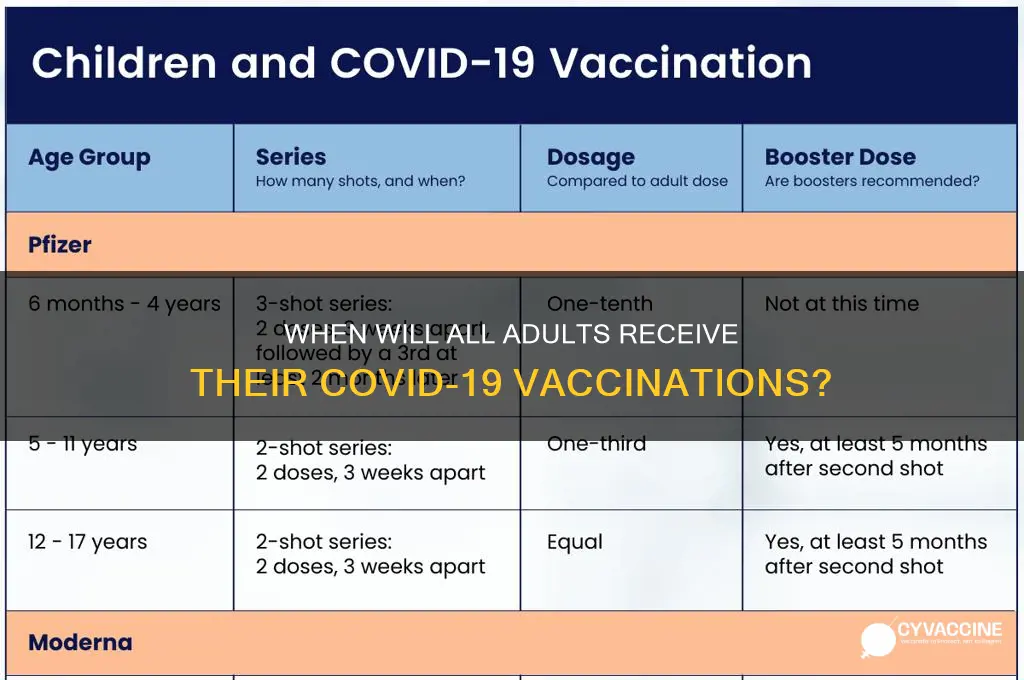
Phased distribution plans often follow a tiered approach, with each phase triggered by vaccine availability and epidemiological data. In many countries, Phase 1 included healthcare workers and long-term care residents, Phase 2 covered essential workers and those over 65, and Phase 3 expanded to all adults aged 16 or 18 and above, depending on the vaccine. For example, the Pfizer-BioNTech vaccine is authorized for individuals 12 and older, while Moderna and AstraZeneca are typically administered to those 18 and above. Completion of Phase 3, which marks the point when all adults are due to be vaccinated, varies widely. Wealthier nations like the U.S. and U.K. achieved this milestone by mid-2021, while many low-income countries are still working toward it, with estimates extending into 2024.
A critical factor in these timelines is the two-dose regimen required for most vaccines, with a gap of 3–12 weeks between doses. For instance, Pfizer recommends a 3-week interval, while AstraZeneca allows up to 12 weeks. This spacing, combined with the need for booster shots, complicates planning. Practical tips for individuals include scheduling doses well in advance, especially in countries with high demand, and staying informed about local guidelines, as eligibility criteria and vaccine types can vary by region.
Comparatively, countries with robust healthcare infrastructure and early vaccine procurement deals have outpaced others. For example, Israel vaccinated its entire adult population by March 2021, thanks to a swift rollout and a single-dose agreement with Pfizer. In contrast, African nations, reliant on COVAX and facing supply shortages, have struggled to vaccinate even 20% of their adult populations. This disparity underscores the need for global cooperation and equitable distribution to meet the estimated completion dates for adult vaccination worldwide.
Looking ahead, the focus is shifting from initial vaccination to booster campaigns and reaching unvaccinated adults. WHO data suggests that as of late 2023, over 60% of the global adult population has received at least one dose, but disparities persist. To accelerate progress, countries must address hesitancy through education, streamline registration processes, and ensure vaccine accessibility in remote areas. By learning from successful rollouts and adapting strategies, the global community can work toward the common goal of vaccinating all adults, with estimated completion dates hinging on continued collaboration and resource allocation.
Coronavirus Vaccine and Stem Cells: Separating Fact from Fiction
You may want to see also
Explore related products






![]()
Priority Groups: Criteria for prioritizing adults based on age, health, and occupation
The rollout of vaccines often begins with a phased approach, targeting specific groups before expanding to the general population. This strategy is crucial for maximizing the impact of limited resources and minimizing severe outcomes. Priority groups are typically identified based on age, health conditions, and occupation, each criterion serving a distinct purpose in protecting public health.
Age is a primary factor due to the correlation between advancing years and increased vulnerability to severe illness. For instance, individuals aged 65 and older are often prioritized because their immune systems naturally weaken, making them more susceptible to complications. In many vaccination campaigns, this group receives the first doses, followed by younger age brackets in descending order. For example, the 50-64 age group might be next in line, with subsequent phases targeting those in their 40s, and so on. This tiered approach ensures that those at highest risk are protected first, reducing hospitalizations and deaths.
Health conditions further refine prioritization, as certain medical issues exacerbate the risk of severe outcomes. Chronic illnesses such as diabetes, heart disease, and respiratory conditions are common criteria for early vaccination. Pregnant individuals and those with compromised immune systems, such as cancer patients undergoing chemotherapy, are also often prioritized. These groups may require specific dosages or formulations, such as mRNA vaccines, which have shown high efficacy and safety profiles. For example, immunocompromised individuals might need a third dose to achieve adequate protection, a strategy supported by guidelines from health organizations like the CDC and WHO.
Occupation plays a critical role in prioritization, particularly for essential workers who face higher exposure risks. Healthcare workers, teachers, grocery store employees, and first responders are often among the first to receive vaccines. Their roles not only put them at personal risk but also make them potential vectors for community spread. For instance, vaccinating healthcare workers early helps maintain the functionality of the healthcare system, while protecting teachers supports the safe reopening of schools. Occupational prioritization often involves collaboration with employers to organize vaccination drives, ensuring efficient distribution and minimal disruption to essential services.
Balancing these criteria requires careful planning and ethical consideration. While age and health conditions focus on individual risk, occupational prioritization addresses societal needs. For example, a 40-year-old teacher with no underlying conditions might be vaccinated before a 55-year-old remote worker with low exposure risk. This approach underscores the dual goals of protecting vulnerable individuals and maintaining critical infrastructure. Practical tips for implementation include clear communication of eligibility criteria, accessible vaccination sites, and flexible scheduling to accommodate work obligations.
In conclusion, prioritizing adults based on age, health, and occupation is a strategic approach to vaccination that maximizes public health benefits. By targeting those at highest risk and those essential to societal functioning, this method ensures that limited resources are used effectively. As vaccination campaigns progress, ongoing monitoring and adjustments to priority groups may be necessary to address emerging challenges, such as new variants or vaccine hesitancy. This dynamic process highlights the importance of data-driven decision-making and adaptability in public health strategies.
Lot Numbers in Vaccines: Ensuring Safety, Traceability, and Quality Control
You may want to see also
Explore related products






![]()
Vaccine Availability: Supply chain challenges and production rates affecting adult vaccination schedules
The global rollout of COVID-19 vaccines has been a monumental task, with the goal of vaccinating all adults as quickly as possible. However, the timeline for achieving this goal is heavily influenced by vaccine availability, which is in turn affected by supply chain challenges and production rates. To understand when all adults are due to be vaccinated, it's essential to examine the complex interplay between these factors.
Consider the production rates of leading vaccine manufacturers. Pfizer-BioNTech, for instance, initially aimed to produce 1.3 billion doses in 2021, while Moderna targeted 600 million doses. These numbers, though impressive, were soon revised upwards due to increased demand and expanded manufacturing capabilities. However, production is only half the battle. The supply chain, a delicate network of transportation, storage, and distribution, has proven to be a significant bottleneck. For example, the Pfizer-BioNTech vaccine requires ultra-cold storage at -70°C, necessitating specialized equipment and infrastructure that many countries lack. This has led to delays in distribution, particularly in low- and middle-income countries.
A critical aspect of vaccine availability is the allocation and prioritization of doses. High-income countries have secured a disproportionate share of available vaccines through advance purchase agreements, leaving many low-income countries reliant on initiatives like COVAX. This disparity has significant implications for global vaccination schedules. For instance, while some countries have already vaccinated a substantial portion of their adult populations, others are still awaiting their first shipments. To address this, manufacturers and global health organizations must collaborate to ensure equitable distribution, taking into account factors such as population size, infection rates, and healthcare infrastructure.
The impact of supply chain challenges and production rates on adult vaccination schedules is further compounded by the need for multiple doses. Most COVID-19 vaccines require two doses, administered several weeks apart. This means that production and distribution must be carefully coordinated to ensure a consistent supply of both initial and follow-up doses. For example, if a country receives a shipment of 1 million first doses but only 500,000 second doses, it risks leaving a significant portion of its population partially vaccinated. To mitigate this, countries must work closely with manufacturers to forecast demand and plan for contingencies, such as dose sharing or alternative vaccine platforms.
Ultimately, the question of when all adults are due to be vaccinated hinges on our ability to overcome these supply chain challenges and scale up production rates. Practical steps can be taken to accelerate this process, such as increasing investment in manufacturing infrastructure, streamlining regulatory approvals, and fostering international cooperation. For individuals, staying informed about local vaccination plans and being prepared to receive a vaccine when it becomes available can help ensure a smoother rollout. By addressing these challenges head-on, we can work towards a more precise timeline for global adult vaccination, bringing an end to the pandemic and its devastating impacts.
Can Employers Legally Request Employee Vaccination Records? Exploring Privacy Rights
You may want to see also
Explore related products






![]()
Booster Shots: Timing and eligibility for additional doses to maintain immunity in adults
As of the latest updates, many countries have outlined plans for booster shots to maintain immunity against COVID-19, with timing and eligibility varying based on age, health status, and initial vaccination dates. For instance, in the United States, adults are generally eligible for a booster shot 5 months after completing their primary Pfizer or Moderna series, or 2 months after the single-dose Johnson & Johnson vaccine. This accelerated timeline reflects the emergence of variants like Omicron, which have underscored the need for enhanced protection. Understanding these specifics is crucial for individuals to stay informed and proactive about their health.
Analyzing the rationale behind booster timing reveals a balance between waning immunity and the body’s response to additional doses. Studies show that antibody levels decline approximately 6 months after the initial vaccination, particularly in older adults and immunocompromised individuals. However, boosters have been proven to restore antibody levels to peak values, reducing the risk of severe illness and hospitalization. For example, a Pfizer booster increases neutralizing antibodies 25-fold within a week of administration. This data highlights why timing is not arbitrary but rooted in immunological science, emphasizing the importance of adhering to recommended intervals.
Eligibility criteria for boosters often prioritize high-risk groups, such as those over 65, individuals with underlying health conditions, and frontline workers. However, as vaccine supply stabilizes, many regions are expanding eligibility to all adults. In the UK, for instance, all adults over 18 are now eligible for a booster, with a 3-month gap between the second dose and the booster. This broader approach aims to maximize population-level immunity, particularly during winter months when respiratory viruses circulate more widely. Practical tips include scheduling boosters during periods of low community transmission to minimize exposure risk and ensuring access to vaccination sites through online booking systems.
Comparing booster strategies globally reveals both similarities and disparities. While the U.S. and EU recommend mRNA boosters (Pfizer or Moderna) for all adults, some countries, like Israel, have pioneered fourth doses for vulnerable populations. This variation reflects differing risk assessments and vaccine availability. For travelers, understanding these differences is essential, as booster requirements may impact international mobility. For instance, some countries mandate boosters for entry, while others accept primary series completion. Staying updated on global guidelines ensures compliance and uninterrupted travel plans.
In conclusion, booster shots are a critical component of maintaining immunity in adults, with timing and eligibility tailored to individual and public health needs. By adhering to recommended intervals, prioritizing high-risk groups, and staying informed about global trends, individuals can maximize their protection against evolving threats. Practical steps, such as monitoring local health advisories and utilizing digital tools for scheduling, further empower proactive health management. As vaccination strategies continue to evolve, clarity and adaptability remain key to navigating this ongoing process effectively.
Listeria Vaccines for Chickens: Available Options and Protection Strategies
You may want to see also
Explore related products






![]()
Global Disparities: Variations in adult vaccination timelines across countries due to resource differences
The COVID-19 pandemic exposed a stark reality: wealthy nations raced to vaccinate their populations while many low-income countries struggled to secure even a fraction of the doses. This disparity wasn't merely a matter of timing; it was a symptom of a deeper inequality in global healthcare resources. While countries like the United States and the United Kingdom aimed to vaccinate all adults within months, others faced timelines stretching into years, highlighting the critical role of infrastructure, funding, and global cooperation in vaccine distribution.
Consider the logistical hurdles. High-income countries possess robust cold chain systems, essential for storing vaccines like Pfizer-BioNTech, which require ultra-cold temperatures (-70°C). In contrast, many African nations lack such infrastructure, limiting their access to these vaccines and forcing reliance on alternatives like AstraZeneca, which are less effective against certain variants. This isn't just about money; it's about the ability to transport, store, and administer vaccines efficiently, a capability often absent in resource-constrained settings.
The purchasing power of nations further exacerbates this divide. Wealthy countries secured billions of doses through advance purchase agreements, sometimes hoarding more than needed. Meanwhile, the COVAX initiative, designed to ensure equitable access, faced funding shortfalls and delays in delivery. For instance, as of mid-2021, while over 50% of adults in the U.S. were fully vaccinated, many African countries had vaccinated less than 5% of their populations. This disparity isn't merely a moral failing; it's a practical one, as unchecked virus spread in any region increases the risk of new variants that could threaten global progress.
To address this, a multi-faceted approach is necessary. First, wealthier nations must fulfill their dose-sharing commitments and support initiatives like COVAX financially and logistically. Second, investment in local manufacturing capabilities in low-income countries can reduce dependency on imports and ensure sustainable vaccine supply. Finally, global health organizations must prioritize transparency and accountability in vaccine distribution, ensuring that resources reach those most in need. Without these steps, the promise of "vaccines for all" will remain an unfulfilled ideal, leaving billions vulnerable and the world at risk.
Exploring Controversial Smallpox Vaccine Debates: Ethics, Efficacy, and Public Health
You may want to see also
Frequently asked questions
As of the latest updates, the U.S. government aimed to make all adults eligible for vaccination by May 1, 2021, though actual vaccination timelines varied by state and availability.
The EU targeted mid-2021 for offering vaccination to all adults, with member states implementing their own distribution schedules based on vaccine supply and logistics.
Global vaccination timelines vary widely due to disparities in vaccine access and distribution. Wealthier nations aimed to vaccinate most adults by late 2021, while many low-income countries faced delays into 2022 or later.