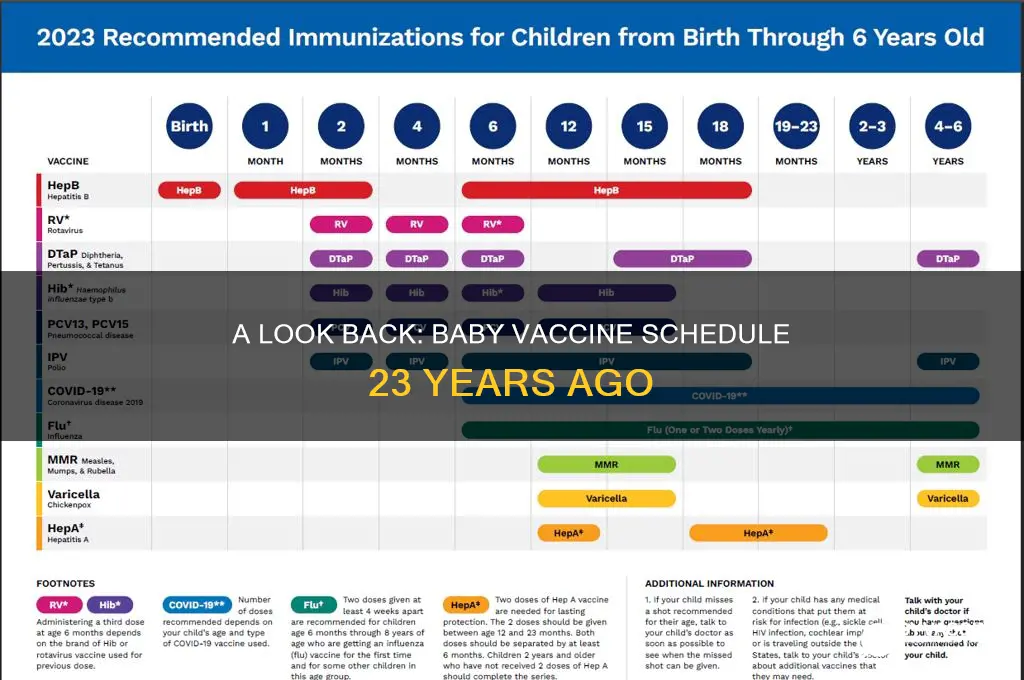
Twenty-three years ago, in the year 2000, the vaccine schedule for infants in many countries, including the United States, followed guidelines established by health organizations like the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO). At that time, the schedule included vaccines to protect against diseases such as hepatitis B, diphtheria, tetanus, pertussis (DTaP), polio (IPV), *Haemophilus influenzae* type b (Hib), pneumococcal disease, and measles, mumps, and rubella (MMR). The timing of doses typically began at birth or within the first few months of life, with subsequent doses administered at 2, 4, 6, and 12–15 months, followed by booster shots in early childhood. Notably, vaccines like the rotavirus vaccine and the chickenpox (varicella) vaccine were either in early stages of implementation or not yet widely included in the routine schedule, reflecting the evolving nature of immunization practices over time.
Explore related products






What You'll Learn
- Routine Immunizations: DTaP, IPV, MMR, Hib, HepB, Varicella, PCV7, and annual flu shots
- Hepatitis B Series: Birth dose followed by two additional doses at 1-2 months and 6-18 months
- MMR Timing: First dose at 12-15 months, second dose at 4-6 years
- Chickenpox Vaccine: Introduced in 1995, one dose at 12-15 months
- Rotavirus Vaccine: Not available 23 years ago; introduced in 2006 for infants
![]()
Routine Immunizations: DTaP, IPV, MMR, Hib, HepB, Varicella, PCV7, and annual flu shots
Twenty-three years ago, a baby’s vaccine schedule was already robust but differed slightly from today’s recommendations. The core immunizations—DTaP, IPV, MMR, Hib, HepB, and annual flu shots—were standard, but newer vaccines like Varicella and PCV7 were either emerging or being integrated into routine care. For instance, the Varicella (chickenpox) vaccine was licensed in the U.S. in 1995, so by 2000, it was becoming a staple, though not yet universally adopted. PCV7, the first pneumococcal conjugate vaccine, was introduced in 2000, targeting seven strains of Streptococcus pneumoniae, a leading cause of bacterial meningitis and pneumonia in infants.
The DTaP vaccine, protecting against diphtheria, tetanus, and pertussis, was typically administered in a series of five doses starting at 2 months, with boosters at 4, 6, 15-18 months, and 4-6 years. IPV (inactivated polio vaccine) followed a similar schedule, replacing the oral polio vaccine in many regions due to safety concerns. MMR (measles, mumps, rubella) was given in two doses, the first at 12-15 months and the second at 4-6 years, though some providers opted for earlier administration during outbreaks. Hib (Haemophilus influenzae type b) vaccine was given in three or four doses, depending on the brand, starting at 2 months to prevent meningitis and pneumonia.
Hepatitis B vaccination began at birth, with the second dose at 1-2 months and the third at 6-18 months, reflecting growing awareness of the virus’s transmission risks. Annual flu shots were recommended starting at 6 months, though compliance varied due to misconceptions about safety and efficacy. The introduction of Varicella and PCV7 added complexity but also expanded protection against previously common childhood illnesses. Varicella was given in one or two doses, depending on age, while PCV7 was administered in a 4-dose series starting at 2 months.
Practical tips for parents included keeping a detailed immunization record, scheduling appointments well in advance, and monitoring for mild side effects like fever or soreness. Combination vaccines, such as those merging DTaP, IPV, and Hib, streamlined the process but required careful coordination with healthcare providers. While the schedule 23 years ago was less crowded than today’s, it laid the groundwork for modern immunization practices, emphasizing early and consistent protection against preventable diseases.
In retrospect, the vaccine schedule of the early 2000s balanced established protocols with emerging innovations, reflecting the evolving science of immunology. Parents today benefit from refinements and additions, but the core principle remains: timely vaccination is a cornerstone of pediatric health. Understanding this historical context highlights the progress made while underscoring the ongoing importance of routine immunizations.
Did I Receive the Hepatitis B Vaccine in School?
You may want to see also
Explore related products






![]()
Hepatitis B Series: Birth dose followed by two additional doses at 1-2 months and 6-18 months
Two decades ago, the Hepatitis B vaccine series for infants was a critical component of early childhood immunization, designed to protect against a virus that can lead to chronic liver disease, cirrhosis, and liver cancer. The schedule was straightforward yet precise: a birth dose, followed by two additional doses at 1-2 months and 6-18 months. This timing was intentional, leveraging the infant’s developing immune system to establish robust immunity. The birth dose, typically administered within 12 hours of delivery, was a proactive measure to neutralize any potential exposure to the virus from the mother or environment. This initial step was non-negotiable, especially in regions with higher prevalence rates, as it significantly reduced the risk of perinatal transmission.
The second dose, given at 1-2 months, served as a critical booster to reinforce the immune response initiated at birth. This interval allowed the infant’s immune system sufficient time to process the first dose while ensuring continuity in protection. Parents were often advised to schedule this dose during routine well-child visits, making it easier to integrate into their healthcare routine. The vaccine, typically administered as a 0.5 mL intramuscular injection in the anterolateral thigh (for infants), was well-tolerated, with mild side effects like soreness at the injection site being the most common.
The final dose, administered between 6-18 months, cemented long-term immunity. This broader window provided flexibility for families while ensuring the dose was given before the child’s first birthday, a milestone age for vaccine completion. Healthcare providers often emphasized the importance of completing the series, as partial vaccination could leave the child vulnerable. For example, a study from the early 2000s highlighted that infants who received all three doses had seroprotection rates exceeding 95%, compared to significantly lower rates in those who missed doses.
Practical tips for parents included keeping a detailed record of vaccination dates, as this series often overlapped with other vaccines like DTaP and Hib. Using a vaccine tracker or app could help manage appointments and ensure no dose was missed. Additionally, parents were encouraged to discuss any concerns about vaccine safety or side effects with their pediatrician, as misinformation was a barrier to adherence even then. The Hepatitis B series was not just a medical protocol but a foundational step in safeguarding a child’s health for years to come.
Vaccines and Virus Mutations: What's the Connection?
You may want to see also
Explore related products






![]()
MMR Timing: First dose at 12-15 months, second dose at 4-6 years
Twenty-three years ago, the MMR vaccine—protecting against measles, mumps, and rubella—was a cornerstone of childhood immunization schedules. The timing of its administration was carefully calibrated to balance immune system readiness and disease risk. The first dose was typically given between 12 and 15 months of age, a window chosen because maternal antibodies, which can interfere with vaccine efficacy, naturally wane by this time. This allowed the child’s immune system to mount a robust response to the vaccine. The second dose was administered between 4 and 6 years of age, often just before a child entered school, providing a critical booster to ensure long-term immunity and community protection.
This staggered approach wasn’t arbitrary. Measles, in particular, posed a significant threat to young children, with complications like pneumonia and encephalitis being more severe in those under 5. By delaying the first dose until 12–15 months, health authorities ensured the vaccine’s effectiveness while minimizing the risk of antibody interference. The second dose at 4–6 years acted as a safety net, catching any children who might not have developed full immunity from the first dose and reinforcing protection during a period of increased social exposure, such as starting kindergarten.
Practical considerations also factored into this schedule. Parents were advised to avoid scheduling the MMR vaccine too close to other live vaccines, as they could potentially interfere with each other’s efficacy. For instance, if a child received the varicella (chickenpox) vaccine, a 4-week interval was recommended before or after the MMR dose. Additionally, if a child missed the 12–15-month window, the vaccine could be given at any time thereafter, with the second dose following at least 28 days later. This flexibility ensured that children remained on track for protection.
Comparatively, this schedule contrasts with earlier practices, where measles vaccines were sometimes given as early as 9 months in high-risk areas. However, by standardizing the first dose at 12–15 months, health systems achieved better consistency and efficacy across populations. The 4–6-year booster, meanwhile, aligned with school entry requirements, making it easier for parents to remember and for healthcare providers to track. This dual-dose strategy not only protected individual children but also contributed to herd immunity, reducing outbreaks in communities.
In retrospect, the MMR timing of 23 years ago reflects a thoughtful balance of immunology, epidemiology, and practical logistics. It underscores the importance of age-specific dosing and the need for boosters to maintain immunity. For parents today, understanding this historical context highlights how vaccine schedules are designed to maximize protection while minimizing risks—a principle that remains unchanged despite evolving medical knowledge.
The End of Polio Vaccination: When Did It Happen?
You may want to see also
Explore related products






![]()
Chickenpox Vaccine: Introduced in 1995, one dose at 12-15 months
In 1995, the chickenpox vaccine emerged as a groundbreaking addition to pediatric immunization schedules, offering parents a new tool to protect their children from a once-common childhood illness. Prior to its introduction, chickenpox (varicella) was a rite of passage for most children, often accompanied by itchy rashes, fever, and discomfort. The vaccine’s arrival marked a shift toward prevention rather than treatment, but its integration into the schedule was deliberate and specific. Administered as a single dose between 12 and 15 months of age, it was designed to align with a baby’s developing immune system while minimizing the risk of severe complications later in life. This timing ensured that infants were protected before potential exposure in daycare or preschool settings, where the virus spreads easily.
From a practical standpoint, the chickenpox vaccine’s introduction required careful planning for parents and healthcare providers. Unlike some vaccines given at birth or during the first six months, this one fell into the toddler immunization window, often coinciding with the measles, mumps, and rubella (MMR) vaccine. Parents were advised to schedule a well-child visit around 12 to 15 months to ensure timely administration. The vaccine itself was a live, attenuated virus, meaning it contained a weakened form of the varicella virus to stimulate immunity without causing the disease. Side effects were generally mild, such as soreness at the injection site or a mild rash, but these were far less disruptive than the actual illness.
Comparatively, the chickenpox vaccine’s rollout contrasted with other vaccines of the era. While vaccines like DTaP (diphtheria, tetanus, and pertussis) and Hib (Haemophilus influenzae type b) had been staples for decades, the chickenpox vaccine addressed a disease often perceived as mild. However, its introduction highlighted growing awareness of varicella’s potential complications, including bacterial infections, pneumonia, and, in rare cases, encephalitis. By vaccinating at 12-15 months, public health officials aimed to reduce both the disease’s prevalence and its associated risks, particularly for vulnerable populations like pregnant women and immunocompromised individuals.
Persuasively, the chickenpox vaccine’s single-dose regimen at 12-15 months underscored the balance between simplicity and efficacy. While a second dose was later recommended for enhanced protection, the initial schedule reflected the vaccine’s high effectiveness in preventing severe disease. For parents 23 years ago, this meant a straightforward addition to their child’s immunization plan, without the complexity of multiple doses or frequent clinic visits. It also reinforced the broader shift toward proactive healthcare, where preventable diseases were targeted early in life to ensure long-term well-being.
In conclusion, the chickenpox vaccine’s introduction in 1995, with its single dose at 12-15 months, was a pivotal moment in pediatric immunization. It exemplified how medical advancements could transform the management of once-common illnesses, offering protection with minimal inconvenience. For parents navigating the vaccine schedule 23 years ago, this addition was both a practical update and a testament to the evolving understanding of childhood health. By adhering to this timeline, they contributed to a collective effort to reduce the burden of chickenpox, setting a precedent for future vaccine developments.
Overcoming Vaccine Hesitancy: The Greatest Challenge to Global Immunization Efforts
You may want to see also
Explore related products






![]()
Rotavirus Vaccine: Not available 23 years ago; introduced in 2006 for infants
A baby born 23 years ago would have missed out on a critical layer of protection against a highly contagious and potentially severe illness: rotavirus. This common childhood infection, causing severe diarrhea, dehydration, and sometimes hospitalization, was a significant concern for parents and pediatricians alike. The rotavirus vaccine, a game-changer in preventing this disease, was not yet available in the early 2000s.
The introduction of the rotavirus vaccine in 2006 marked a significant advancement in pediatric healthcare. This vaccine, administered orally in a liquid form, is typically given in a series of doses starting at 2 months of age. The specific schedule may vary slightly depending on the brand, but generally, infants receive the first dose at 2 months, followed by a second dose at 4 months, and sometimes a third dose at 6 months. This timing is crucial, as it ensures protection during the period when infants are most vulnerable to rotavirus infection.
Imagine a world where this vaccine didn't exist. Parents would have relied solely on hygiene practices and quick response to symptoms, which, while important, are not foolproof. The rotavirus vaccine has dramatically reduced the incidence of severe rotavirus disease, leading to fewer hospitalizations and a significant decrease in healthcare costs associated with treating this illness. Its impact is particularly notable in developing countries, where access to medical care might be limited, and the consequences of dehydration can be life-threatening.
The absence of the rotavirus vaccine 23 years ago highlights the rapid progress in medical science. It serves as a reminder that vaccine schedules are not static but evolve as new vaccines are developed and approved. This evolution ensures that each generation of children receives the best possible protection against preventable diseases. For parents today, the inclusion of the rotavirus vaccine in the routine immunization schedule provides peace of mind, knowing their infants are shielded from a once-common and potentially serious illness.
In practical terms, the introduction of the rotavirus vaccine has simplified the management of infant health. Instead of solely focusing on reactive measures, healthcare providers can now proactively prevent rotavirus infections. This shift not only benefits individual children but also contributes to herd immunity, reducing the overall circulation of the virus in communities. As we reflect on the vaccine schedule from 23 years ago, the absence of the rotavirus vaccine stands out as a significant gap, now thankfully filled by a safe and effective preventive measure.
Essential Puppy Vaccinations: Understanding the 5-Way Shot Components
You may want to see also
Frequently asked questions
23 years ago (around 2000), the vaccine schedule for babies in the U.S. included vaccines like DTaP (Diphtheria, Tetanus, Pertussis), IPV (Polio), Hib (Haemophilus influenzae type b), Hepatitis B, MMR (Measles, Mumps, Rubella), and Varicella (Chickenpox). The schedule was similar to today’s but with fewer doses and no vaccines like Rotavirus or PCV13, which were introduced later.
Yes, 23 years ago, some vaccines were given at slightly different ages. For example, the Hepatitis B vaccine series often started at 2 months instead of birth, and the Varicella vaccine was typically given around 12-18 months, with no second dose recommended yet. The Rotavirus vaccine was not available, and the PCV (Pneumococcal) vaccine had fewer doses.
The oral Polio vaccine (OPV) was still in use 23 years ago, though it was being phased out in favor of the inactivated Polio vaccine (IPV) due to safety concerns. Additionally, older versions of the Hib vaccine were used, and the combination vaccines were less common, so babies might have received more individual shots.