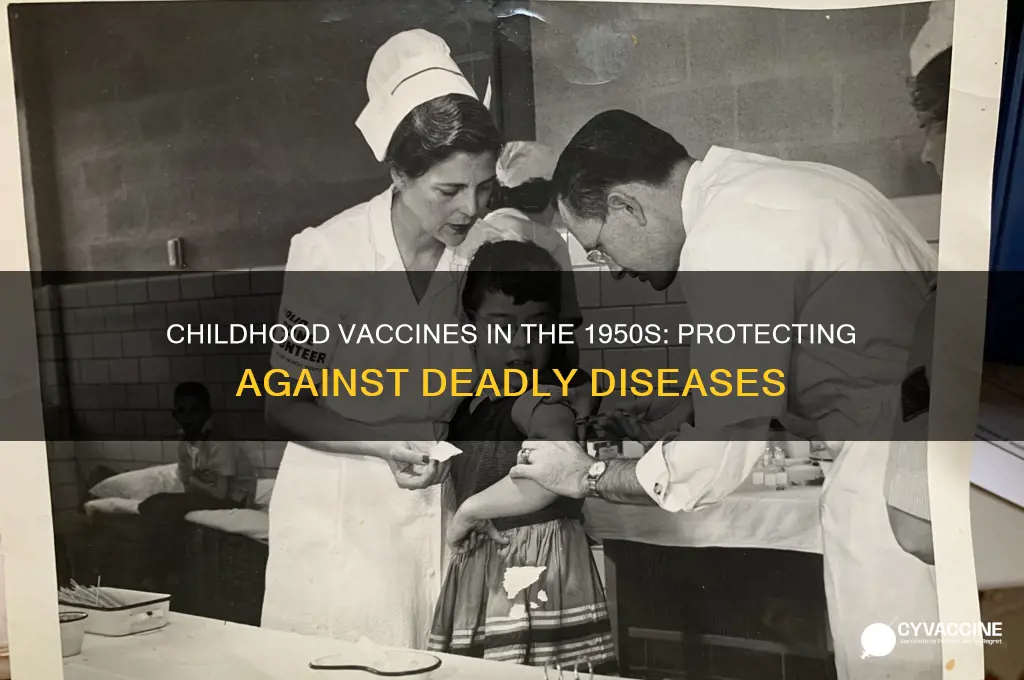
In the 1950s, childhood vaccination programs were significantly expanding, driven by advancements in medical science and public health initiatives. Children during this era were primarily vaccinated against diseases that were once widespread and often deadly, including diphtheria, pertussis (whooping cough), tetanus, polio, and smallpox. The development of the polio vaccine by Jonas Salk in 1955 marked a pivotal moment, drastically reducing the incidence of this crippling disease. Additionally, the DPT (diphtheria, pertussis, and tetanus) vaccine became a standard part of childhood immunization schedules, protecting against these bacterial infections. Smallpox vaccination, though older, continued to be administered, contributing to its eventual eradication. These vaccines not only saved countless lives but also laid the foundation for modern immunization practices, shaping public health strategies for decades to come.
| Characteristics | Values |
|---|---|
| Vaccines Available | Diphtheria, Tetanus, Pertussis (DTP), Smallpox, Polio, Measles, Mumps, Rubella (MMR introduced later but diseases were prevalent) |
| Polio Vaccine | Jonas Salk's inactivated polio vaccine (IPV) introduced in 1955 |
| Smallpox Vaccine | Routine smallpox vaccination was still common in the 1950s |
| DTP Vaccine | Combined vaccine for Diphtheria, Tetanus, and Pertussis was widely used |
| Measles Vaccine | No measles vaccine available in the 1950s; first licensed in 1963 |
| Mumps Vaccine | No mumps vaccine available in the 1950s; first licensed in 1967 |
| Rubella Vaccine | No rubella vaccine available in the 1950s; first licensed in 1969 |
| Vaccine Schedule | Less standardized compared to modern schedules |
| Disease Prevalence | High rates of polio, measles, mumps, rubella, diphtheria, and tetanus |
| Vaccine Technology | Primarily whole-cell or inactivated vaccines |
| Global Vaccination | Vaccination efforts were more localized, with varying access globally |
| Public Health Impact | Significant reduction in childhood mortality and morbidity post-1950s |
Explore related products






What You'll Learn
![]()
Polio vaccine rollout and impact on child health
The 1950s marked a pivotal era in child health with the rollout of the polio vaccine, a breakthrough that reshaped public health globally. Before its introduction, polio was a dreaded disease, paralyzing or killing thousands of children annually, particularly during summer outbreaks. The vaccine’s arrival wasn’t just a medical achievement; it was a cultural turning point, shifting societal perceptions of disease prevention. Developed by Jonas Salk in 1955, the inactivated polio vaccine (IPV) was administered via injection, offering robust protection against the poliovirus. This innovation set the stage for a dramatic decline in polio cases, transforming it from a widespread threat to a rare disease in many parts of the world.
The rollout of the polio vaccine was a meticulously planned campaign, targeting children as the primary recipients due to their heightened vulnerability. Initially, the vaccine was administered in three doses, spaced over several months, to ensure full immunity. Public health officials prioritized children aged 6 to 9, as they were most at risk during outbreaks. Schools and community centers became hubs for vaccination drives, with parents urged to bring their children for inoculation. The campaign’s success relied on mass participation, and the results were striking: within a decade, polio cases in the U.S. plummeted from over 15,000 annually to a few hundred. This rapid decline underscored the vaccine’s efficacy and the power of collective action in public health.
Beyond its immediate health benefits, the polio vaccine rollout had profound societal implications. It fostered a new era of trust in vaccines, encouraging further research and development in immunology. The success of the polio campaign laid the groundwork for future vaccination programs, such as those for measles, mumps, and rubella. For parents, the vaccine offered peace of mind, freeing children from the constant fear of paralysis or death. However, the campaign wasn’t without challenges. Misinformation and skepticism initially slowed uptake in some communities, highlighting the need for clear, accessible communication in public health initiatives.
Today, the legacy of the polio vaccine rollout endures as a testament to the impact of preventive medicine. While polio remains endemic in a few countries, global efforts continue to eradicate it entirely. For parents and caregivers, the story of the polio vaccine serves as a reminder of the importance of timely vaccinations. Ensuring children receive their polio immunizations, typically starting at 2 months of age with a series of shots, remains critical. The 1950s polio vaccine rollout wasn’t just a medical triumph; it was a lesson in how science, community, and policy can unite to safeguard the health of future generations.
Wisconsin's Next Vaccination Phase: Who's Up for COVID-19 Shots?
You may want to see also
Explore related products






![]()
Measles vaccination efforts and early prevention strategies
The 1950s marked a pivotal era in the fight against measles, a highly contagious disease that had long plagued childhood populations. Before the advent of the measles vaccine, the disease was a rite of passage, infecting nearly all children by age 15. Complications such as pneumonia, encephalitis, and death were not uncommon, making measles a significant public health concern. The development of the first measles vaccine in 1963 was a breakthrough, but the groundwork for its success was laid in the 1950s through early prevention strategies and a growing understanding of the virus.
Analytical Perspective:
Early prevention strategies in the 1950s relied heavily on isolation and quarantine measures. When a child contracted measles, health departments would advise families to keep the infected child at home, away from school and public spaces, for at least 10 days. This approach, while effective in limiting immediate spread, was reactive rather than proactive. Public health campaigns also emphasized hygiene, such as frequent handwashing and avoiding close contact with infected individuals. However, these measures were insufficient to curb widespread outbreaks, highlighting the urgent need for a more robust solution.
Instructive Approach:
One of the most critical steps in the 1950s was the identification and study of the measles virus itself. In 1954, John F. Enders and his team successfully isolated the measles virus in cell culture, a breakthrough that paved the way for vaccine development. This discovery allowed researchers to study the virus’s behavior, transmission patterns, and potential vulnerabilities. Parents were encouraged to report cases promptly to local health authorities, enabling better tracking of outbreaks and more targeted isolation efforts. While vaccination was not yet available, this period laid the scientific foundation for future immunization programs.
Comparative Analysis:
Compared to other vaccine-preventable diseases like polio, measles presented unique challenges in the 1950s. Polio had a more visible and immediate impact, with images of children in iron lungs galvanizing public support for vaccination. Measles, while equally dangerous, was often dismissed as a "mild" childhood illness. This perception hindered early prevention efforts, as public awareness and funding lagged. However, the 1950s saw a shift in this mindset, with health organizations like the WHO and CDC beginning to prioritize measles as a target for eradication. This shift in focus was crucial, as it set the stage for the vaccine’s eventual rollout in the 1960s.
Descriptive Narrative:
Imagine a 1950s household where measles has struck. The infected child is confined to a dimly lit room, curtains drawn to protect their sensitive eyes from light. Siblings are kept at a distance, and the family anxiously awaits the telltale rash to fade. This scene was commonplace, but it also fueled determination among scientists and health workers. By the late 1950s, clinical trials for early measles vaccines were underway, though these initial attempts were not yet fully effective. The persistence of researchers during this decade was instrumental, as they refined techniques and learned from failures, ultimately leading to the creation of the safe and effective vaccine that would transform measles prevention.
Practical Takeaway:
While the 1950s did not see widespread measles vaccination, the decade’s efforts in isolation, research, and public awareness were indispensable. Parents today can draw parallels to modern prevention strategies: prompt reporting of symptoms, adherence to quarantine guidelines, and support for vaccination programs. The lessons of the 1950s remind us that even without a vaccine, proactive measures can save lives. For those born after the 1960s, the measles vaccine is typically administered in two doses—the first at 12–15 months and the second at 4–6 years—a direct result of the groundwork laid in this critical decade.
Understanding RTS,S/AS01: The Malaria Vaccine and Its Composition
You may want to see also
Explore related products






![]()
Diphtheria immunization programs in schools and communities
In the 1950s, diphtheria immunization programs became a cornerstone of public health efforts in schools and communities, targeting a disease that had historically caused widespread morbidity and mortality among children. These programs were designed to administer the diphtheria toxoid vaccine, often combined with tetanus and pertussis (DTaP), to children aged 2 months to 6 years. The standard schedule included a series of three doses, each 4–8 weeks apart, followed by booster shots at 12–18 months and 4–6 years. School nurses and local health departments played a critical role in organizing mass vaccination clinics, ensuring that children received their doses on time and maintaining records to track compliance.
The success of these programs relied on community engagement and education. Parents were informed about the vaccine’s safety and efficacy through pamphlets, public meetings, and school newsletters. Common concerns, such as mild side effects (e.g., soreness at the injection site or low-grade fever), were addressed to build trust. In underserved areas, mobile clinics were deployed to reach children who might otherwise lack access to healthcare. This proactive approach not only reduced diphtheria cases but also set a precedent for future school-based immunization campaigns, such as those for polio and measles.
Analyzing the impact of these programs reveals a dramatic decline in diphtheria incidence. In the United States, cases dropped from over 200,000 annually in the 1920s to fewer than 1,000 by the late 1950s. This reduction was directly linked to high vaccination rates achieved through school and community initiatives. However, challenges persisted, including vaccine hesitancy and logistical hurdles in rural areas. Health officials addressed these issues by partnering with local leaders and emphasizing the collective benefit of herd immunity, a concept that gained prominence during this era.
A comparative look at global efforts highlights the adaptability of diphtheria immunization programs. In the United Kingdom, the National Health Service integrated vaccination into routine school health checks, while in developing countries, international organizations like UNICEF supported campaigns in high-risk regions. Despite differences in resources, the core strategy remained consistent: prioritize children, leverage community networks, and ensure consistent vaccine supply. This global collaboration underscored the importance of localized yet coordinated efforts in combating infectious diseases.
For modern readers, the 1950s diphtheria programs offer practical takeaways. First, successful immunization campaigns require clear communication and community involvement. Second, integrating vaccination into existing systems, such as schools, maximizes reach and efficiency. Finally, addressing hesitancy through education and transparency remains crucial. While diphtheria is now rare in many parts of the world, the lessons from these early programs continue to inform public health strategies, reminding us that prevention through vaccination is both a science and a social endeavor.
Hepatitis B Vaccine: Understanding the Injection Schedule and Doses
You may want to see also
Explore related products






![]()
Pertussis (whooping cough) vaccine development and distribution
The 1950s marked a pivotal era in childhood vaccination, with pertussis (whooping cough) emerging as a primary target due to its devastating impact on infants and young children. Before the vaccine, pertussis caused approximately 200,000 cases and 4,000 deaths annually in the United States alone. The development of the whole-cell pertussis vaccine in the 1940s laid the groundwork, but it was in the 1950s that its distribution became widespread, integrated into the diphtheria-tetanus-pertussis (DTP) combination vaccine. This innovation streamlined immunization efforts, protecting children against three deadly diseases with a single series of shots.
The DTP vaccine was typically administered in a series of three doses, starting at 2 months of age, followed by boosters at 4 and 6 months. A fourth dose was often given between 15 and 18 months, with a final booster before entering school. Each dose contained 5–10 µg of pertussis antigen, a concentration sufficient to induce immunity but later criticized for causing mild to moderate side effects, such as fever, irritability, and localized swelling. Despite these drawbacks, the vaccine’s efficacy was undeniable, reducing pertussis cases by over 80% within a decade of its widespread use.
However, the whole-cell pertussis vaccine’s success was not without controversy. Reports of rare but severe adverse events, including seizures and hypotonic-hyporesponsive episodes, sparked public concern in the 1970s and 1980s. This led to a decline in vaccination rates in some regions, resulting in pertussis outbreaks that underscored the vaccine’s importance. The 1950s distribution efforts, though imperfect, established a critical framework for herd immunity, saving countless lives and paving the way for safer acellular pertussis vaccines developed in the 1990s.
Practical tips for parents in the 1950s included monitoring children for 24–48 hours post-vaccination, using cool compresses for injection site pain, and consulting a physician if fever exceeded 102°F. Public health campaigns emphasized the vaccine’s role in preventing a disease that often left children gasping for air with a distinctive "whoop" sound—a harrowing symptom that could last for weeks. By the end of the decade, the pertussis vaccine had become a cornerstone of pediatric care, a testament to the era’s commitment to eradicating preventable childhood diseases.
Meningitis Vaccination During Pregnancy: Safety, Benefits, and Recommendations
You may want to see also
Explore related products






![]()
Tetanus shots for children and injury prevention measures
In the 1950s, tetanus shots were a critical component of childhood vaccination schedules, primarily due to the prevalence of tetanus-prone injuries in environments where sanitation was often inadequate. Tetanus, caused by the bacterium *Clostridium tetani*, enters the body through wounds, particularly those contaminated with soil, dust, or manure. For children, who were frequently exposed to outdoor hazards while playing, this vaccine was a lifeline. The tetanus toxoid vaccine, typically administered as a combination with diphtheria and pertussis (DTP), provided robust immunity against this potentially fatal disease. A standard series involved three doses in infancy, followed by boosters every 5–10 years, ensuring long-term protection.
One of the most effective injury prevention measures tied to tetanus shots was the emphasis on wound care. Parents were instructed to clean all cuts, scrapes, and punctures thoroughly with soap and water, followed by the application of an antiseptic. Deep or dirty wounds, especially those involving rusted metal, required immediate medical attention to assess the need for a tetanus booster. This dual approach—vaccination and vigilant wound management—significantly reduced tetanus cases in children. For instance, a child who stepped on a rusty nail would receive a booster if their last dose was over five years prior, ensuring ongoing immunity.
The analytical perspective reveals that tetanus shots were not just about vaccination but part of a broader strategy to mitigate risks in daily life. In the 1950s, playgrounds often featured metal equipment, and rural areas exposed children to farm hazards. Vaccination campaigns were paired with public health education, teaching parents and children to avoid risky behaviors like playing in construction sites or handling sharp objects. This proactive stance underscores the era’s focus on prevention over cure, a principle still relevant today.
From a practical standpoint, administering tetanus shots to children required careful planning. The vaccine was typically given at 2, 4, and 6 months of age, with a booster at 15–18 months and another between 4–6 years. Side effects were generally mild—soreness at the injection site, low-grade fever, or fussiness—but parents were advised to monitor for rare allergic reactions. Combining tetanus vaccination with routine pediatric visits ensured compliance, as did school entry requirements that mandated up-to-date immunizations. This structured approach made tetanus prevention a seamless part of childhood healthcare.
In conclusion, tetanus shots in the 1950s were more than a medical intervention; they were a cornerstone of child safety, intertwined with injury prevention measures that addressed the realities of the time. By vaccinating children and educating families on wound care and hazard avoidance, public health officials dramatically reduced tetanus cases, setting a precedent for modern immunization practices. This legacy reminds us that vaccines are most effective when paired with practical, everyday precautions.
Canceling Your Publix Vaccine Appointment: A Quick and Easy Guide
You may want to see also
Frequently asked questions
In the 1950s, children were commonly vaccinated for diseases such as diphtheria, pertussis (whooping cough), tetanus, smallpox, and polio.
Yes, the polio vaccine became widely available in the mid-1950s after Jonas Salk developed the inactivated polio vaccine (IPV) in 1955, leading to mass vaccination campaigns.
No, the measles vaccine was not available in the 1950s. It was first licensed in 1963, and the combined measles, mumps, and rubella (MMR) vaccine was introduced later.
Influenza vaccines were not routinely given to children in the 1950s. The first flu vaccines were developed in the 1940s, but widespread childhood vaccination for flu did not become common until later decades.
No, vaccines for mumps and rubella were not available in the 1950s. The mumps vaccine was licensed in 1967, and the rubella vaccine followed in 1969, with the combined MMR vaccine introduced in the 1970s.