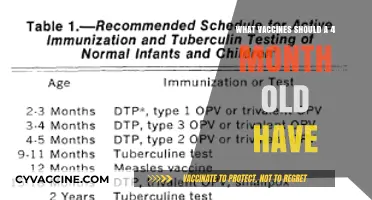
In the 1970s, the landscape of vaccination was marked by significant advancements and the widespread availability of several key vaccines that had been developed in the preceding decades. By this time, routine immunization programs had firmly established vaccines such as the DTP (diphtheria, tetanus, and pertussis), polio (both oral and inactivated forms), measles, mumps, and rubella (MMR) vaccines, which were becoming standard in many countries. The tetanus and diphtheria vaccines, introduced earlier, continued to be widely used, while the pertussis component was integrated into combination vaccines. Additionally, the influenza vaccine was available, though primarily recommended for high-risk groups. The decade also saw the introduction of the hepatitis B vaccine in its early stages, though it was not yet widely accessible. These vaccines played a crucial role in reducing the incidence of infectious diseases and laid the foundation for modern immunization practices.
| Characteristics | Values |
|---|---|
| Vaccines Available | DTP (Diphtheria, Tetanus, Pertussis), Polio (OPV), Measles, Mumps, Rubella |
| DTP Vaccine | Combination vaccine; whole-cell pertussis component; administered to infants and children |
| Polio Vaccine (OPV) | Oral Poliovirus Vaccine (OPV); live attenuated; widely used globally |
| Measles Vaccine | Live attenuated virus; single-antigen vaccine |
| Mumps Vaccine | Live attenuated virus; single-antigen vaccine |
| Rubella Vaccine | Live attenuated virus; single-antigen vaccine |
| Administration Route | Intramuscular (DTP, Measles, Mumps, Rubella), Oral (Polio) |
| Target Population | Infants, children, and adolescents |
| Schedule | Multiple doses starting at 2 months of age, with boosters as needed |
| Storage Requirements | Refrigerated (2°C to 8°C) for most vaccines |
| Manufacturer Examples | Merck, Sharp & Dohme, Wyeth, Lederle Laboratories |
| Global Availability | Widely available in developed countries; limited access in some regions |
| Side Effects | Mild fever, soreness at injection site, rare severe reactions (e.g., DTP) |
| Impact | Significant reduction in morbidity and mortality from targeted diseases |
Explore related products






What You'll Learn
- Childhood Vaccines: MMR, DPT, Polio, and smallpox vaccines were widely available and routinely administered
- Influenza Vaccines: Annual flu shots became more common for high-risk groups in the 1970s
- Tetanus and Diphtheria: Booster shots for adults were available to maintain immunity against these diseases
- Measles Elimination: Vaccination campaigns aimed to eradicate measles globally, with significant progress by 1978
- Rubella Prevention: The rubella vaccine was introduced to prevent congenital rubella syndrome in newborns
![]()
Childhood Vaccines: MMR, DPT, Polio, and smallpox vaccines were widely available and routinely administered
The 1970s marked a pivotal era in childhood immunization, with several vaccines becoming widely available and routinely administered. Among these, the MMR (Measles, Mumps, Rubella), DPT (Diphtheria, Pertussis, Tetanus), Polio, and smallpox vaccines stood out as cornerstones of public health. These vaccines were not just medical advancements but essential tools in preventing devastating diseases that had historically plagued childhood. By the 1970s, vaccination schedules were becoming standardized, ensuring that children received protection at critical developmental stages.
The MMR vaccine, introduced in 1971, revolutionized the fight against three highly contagious diseases. Administered typically at 12–15 months of age, with a second dose at 4–6 years, it provided lifelong immunity for most recipients. Measles, mumps, and rubella, once common causes of severe complications like encephalitis and congenital rubella syndrome, saw dramatic declines in incidence. Parents were advised to monitor children for mild fever or rash post-vaccination, but these side effects were far outweighed by the vaccine’s benefits. The MMR vaccine’s success underscored the power of combination vaccines in simplifying immunization efforts.
Similarly, the DPT vaccine was a staple in childhood immunization, protecting against diphtheria, pertussis (whooping cough), and tetanus. Given in a series of five doses starting at 2 months of age, it was a critical defense against pertussis, which could be life-threatening in infants. While concerns about side effects like fever and soreness led to the development of the acellular DTaP vaccine in later decades, the 1970s version remained a vital tool. Parents were often instructed to administer acetaminophen to manage post-vaccination discomfort, ensuring adherence to the schedule.
Polio vaccination in the 1970s was a testament to the triumph of science over a once-feared disease. The oral polio vaccine (OPV), introduced in the 1960s, was widely used alongside the inactivated polio vaccine (IPV). Children received multiple doses starting at 2 months, with boosters ensuring long-term immunity. By the 1970s, polio cases in the U.S. had plummeted, thanks to aggressive vaccination campaigns. The vaccine’s success was a global model, inspiring efforts to eradicate polio worldwide.
Smallpox vaccination, though less common by the 1970s, remained a symbol of vaccination’s potential. Routine smallpox vaccination had begun to phase out in many countries due to the disease’s near-eradication, but it was still administered in regions where the risk persisted. The vaccine’s distinctive scar on the upper arm became a badge of protection, a reminder of humanity’s victory over a disease that had killed millions. Its success paved the way for future eradication efforts, proving that vaccines could eliminate diseases entirely.
Together, these vaccines transformed childhood health in the 1970s, setting the stage for modern immunization programs. Their widespread availability and routine administration reflected a growing consensus on the importance of preventive medicine. For parents, adhering to vaccination schedules became a fundamental act of care, safeguarding children against diseases that had once been commonplace. The legacy of these vaccines endures, reminding us of the ongoing need to protect future generations through immunization.
Don't Neglect Your Vaccination: Stay Protected with a Simple Shot
You may want to see also
Explore related products






![]()
Influenza Vaccines: Annual flu shots became more common for high-risk groups in the 1970s
The 1970s marked a pivotal shift in influenza vaccination strategies, as annual flu shots transitioned from a niche intervention to a standard preventive measure for high-risk populations. Prior to this decade, flu vaccines were primarily administered during outbreaks or to specific occupational groups, such as healthcare workers. However, growing awareness of influenza's disproportionate impact on vulnerable individuals—elderly adults, pregnant women, and those with chronic conditions—spurred public health initiatives to prioritize these groups. By the mid-1970s, the Centers for Disease Control and Prevention (CDC) began formally recommending annual flu vaccination for high-risk individuals, laying the groundwork for today's widespread immunization campaigns.
From a practical standpoint, the 1970s flu vaccines were trivalent, targeting three influenza strains (two A subtypes and one B subtype) based on global surveillance data. These vaccines were typically administered as a single 0.5 mL intramuscular dose, often in the deltoid muscle for adults and the anterolateral thigh for young children. While the formulation process remained similar to earlier decades, advancements in strain selection and manufacturing consistency improved vaccine efficacy. However, cold chain logistics were still rudimentary, requiring careful storage at 2–8°C to maintain potency—a challenge in rural or underresourced areas.
One critical takeaway from this era is the importance of targeted vaccination campaigns. Public health messaging emphasized the flu's severity in high-risk groups, such as the 1968 H3N2 pandemic's disproportionate mortality among the elderly. For instance, individuals over 65 were encouraged to receive their flu shots in early fall, ideally by October, to ensure immunity before peak flu season. Similarly, pregnant women were advised to vaccinate during any trimester, as maternal antibodies provided passive protection to newborns. These tailored recommendations reflected a growing understanding of immunology and disease transmission dynamics.
Despite progress, the 1970s influenza vaccination efforts faced limitations. Vaccine uptake remained modest, partly due to skepticism and limited access. For example, rural communities often lacked nearby clinics offering flu shots, while urban areas struggled with inconsistent supply. Additionally, the vaccines' effectiveness varied annually, depending on the match between circulating strains and those in the vaccine. This unpredictability underscored the need for ongoing research and surveillance, which would later lead to more sophisticated vaccine development and distribution systems.
In retrospect, the 1970s were a formative decade for influenza vaccination, establishing the framework for modern high-risk group prioritization. Practical lessons from this era—such as early-season vaccination, targeted outreach, and cold chain management—remain relevant today. While challenges persisted, the decade's efforts demonstrated the power of preventive medicine in reducing flu-related morbidity and mortality, setting the stage for the universal flu vaccination programs we recognize now.
Vaccinated Children: Allergic Reaction Rates and Safety Concerns
You may want to see also
Explore related products






![]()
Tetanus and Diphtheria: Booster shots for adults were available to maintain immunity against these diseases
In the 1970s, tetanus and diphtheria were not relics of the past but ongoing threats, particularly for adults whose childhood immunizations had waned. Booster shots for these diseases were a cornerstone of adult vaccination schedules, designed to reinforce immunity and prevent severe complications. The combined tetanus-diphtheria (Td) vaccine was the standard, typically administered every 10 years after the initial childhood series. This regimen ensured that adults maintained protection against tetanus, a bacterial infection causing painful muscle stiffness, and diphtheria, a respiratory illness marked by a thick, gray membrane in the throat. For those at higher risk, such as healthcare workers or travelers to regions with poor sanitation, more frequent boosters were often recommended.
The Td vaccine was straightforward in its administration: a single intramuscular injection, usually in the deltoid muscle of the upper arm. Side effects were generally mild, including soreness at the injection site, fatigue, or low-grade fever. Despite its simplicity, adherence to the booster schedule was critical. Tetanus spores, found in soil and dust, could enter the body through even minor wounds, while diphtheria spread through respiratory droplets, making both diseases ever-present dangers. Adults who neglected their boosters risked not only severe illness but also long-term complications like heart damage or nerve issues from diphtheria, or tetanus’s potentially fatal muscle spasms.
One notable advancement in the 1970s was the introduction of the tetanus-diphtheria-pertussis (Tdap) vaccine, which added protection against pertussis (whooping cough). While initially targeted at adolescents and adults, Tdap eventually replaced Td as the preferred booster for all age groups. This shift underscored the evolving understanding of pertussis as a significant threat not only to infants but also to adults, who could unknowingly transmit the disease. The Tdap vaccine’s inclusion of pertussis antigen provided a three-in-one defense, streamlining adult immunization efforts.
Practical tips for adults in the 1970s included keeping a record of vaccination dates to ensure timely boosters and consulting healthcare providers before travel, especially to areas with high disease prevalence. For those with uncertain vaccination histories, a Td or Tdap shot was often recommended, followed by a booster every 10 years. Pregnant women, in particular, were advised to receive Tdap during each pregnancy to pass on protective antibodies to their newborns, a practice that became standard in later decades. These measures reflected a growing awareness of the lifelong need for immunization, moving beyond childhood vaccines to encompass adult health.
In retrospect, the availability of tetanus and diphtheria booster shots in the 1970s marked a pivotal step in public health, bridging the gap between childhood immunity and lifelong protection. While the vaccines themselves were not new, their integration into adult healthcare routines highlighted a shift toward preventive medicine. Today, the legacy of these boosters endures in modern vaccination protocols, reminding us that immunity is not a one-time achievement but a continuous commitment. For adults in the 1970s, these shots were more than just a jab—they were a shield against diseases that, though preventable, remained ever-present.
Montessori School Attendance: Are Vaccinations Required?
You may want to see also
Explore related products

$11.93 $21.99





![]()
Measles Elimination: Vaccination campaigns aimed to eradicate measles globally, with significant progress by 1978
By the 1970s, measles was a leading cause of childhood mortality globally, claiming millions of lives annually. The introduction of the measles vaccine in 1963 marked a turning point, but widespread immunization campaigns were necessary to curb the virus’s devastating impact. By 1978, these efforts had gained significant traction, particularly in developed nations. The measles vaccine, typically administered as a single dose to children aged 12–15 months, demonstrated remarkable efficacy, reducing cases by over 90% in countries with high vaccination coverage. This success was a testament to the power of coordinated public health initiatives, setting the stage for global eradication efforts.
The 1970s saw a shift from reactive measles control to proactive elimination strategies. Countries like the United States and the United Kingdom implemented school-based vaccination programs, ensuring children received the vaccine before entering primary education. In the U.S., the Measles, Mumps, and Rubella (MMR) combination vaccine, introduced in 1971, streamlined immunization efforts, reducing the number of injections required. Public health officials also targeted high-risk populations, such as urban slum dwellers and rural communities, with mobile clinics and door-to-door campaigns. These measures not only lowered measles incidence but also decreased complications like pneumonia and encephalitis, which were major contributors to measles-related deaths.
Despite progress, challenges persisted. Vaccine hesitancy, logistical hurdles in low-income countries, and the virus’s highly contagious nature slowed eradication efforts. Measles’ basic reproduction number (R0) of 12–18 meant that 95% vaccination coverage was necessary to achieve herd immunity. By 1978, while some regions had surpassed this threshold, others lagged far behind. International organizations like the World Health Organization (WHO) began advocating for global vaccine equity, recognizing that measles elimination in one country could be undermined by outbreaks elsewhere. This era laid the groundwork for the modern concept of global health interdependence.
A critical takeaway from the 1970s measles campaigns is the importance of sustained political commitment and community engagement. Successful programs combined top-down policy with grassroots mobilization, leveraging local leaders, schools, and media to promote vaccination. For instance, the U.S. Centers for Disease Control and Prevention (CDC) partnered with Disney to create educational materials featuring Mickey Mouse, increasing vaccine acceptance among children. Such innovative approaches, coupled with rigorous data collection to track progress, ensured that measles elimination remained a priority even as other health issues competed for attention.
By 1978, measles was no longer the unstoppable killer it had once been, thanks to the tireless efforts of vaccinators, policymakers, and communities worldwide. While global eradication remained elusive, the 1970s campaigns demonstrated that with sufficient resources and coordination, even the most pervasive diseases could be brought to heel. This legacy continues to inspire modern vaccination efforts, reminding us that the fight against infectious diseases is won not just through science, but through solidarity.
Zóster Vaccine Cost in Twin Cities: What to Expect
You may want to see also
Explore related products






![]()
Rubella Prevention: The rubella vaccine was introduced to prevent congenital rubella syndrome in newborns
The 1970s marked a pivotal era in vaccine development, with several key immunizations becoming widely available to the public. Among these, the rubella vaccine stands out for its profound impact on public health, particularly in preventing congenital rubella syndrome (CRS) in newborns. Before its introduction, rubella outbreaks were common, and the virus posed a significant risk to pregnant women and their unborn children. CRS could lead to severe birth defects, including deafness, cataracts, heart defects, and developmental delays. The rubella vaccine, first licensed in 1969 and widely distributed in the 1970s, became a cornerstone in eradicating this threat.
Administered as part of the MMR (measles, mumps, rubella) vaccine, the rubella component is typically given in two doses: the first at 12–15 months of age and the second at 4–6 years. This schedule ensures long-term immunity, reducing the risk of infection during pregnancy. For women of childbearing age, verifying immunity through blood tests is crucial, as contracting rubella during pregnancy can have devastating consequences. If non-immune, vaccination is recommended, but it must be administered at least one month before conception to ensure safety.
The introduction of the rubella vaccine in the 1970s exemplifies the power of preventive medicine. By targeting a specific vulnerability—the risk of CRS—this vaccine not only protected individuals but also disrupted the virus's transmission chains. Its success is evident in the dramatic decline of rubella cases globally, with many countries now reporting near-elimination of the disease. This achievement underscores the importance of widespread vaccination and public health education in combating infectious diseases.
Practical tips for ensuring rubella prevention include maintaining vaccination records, staying informed about local outbreaks, and consulting healthcare providers before pregnancy. Schools and workplaces can also play a role by promoting vaccine awareness and compliance. While the rubella vaccine is highly effective, no medical intervention is without considerations. Mild side effects, such as fever or rash, may occur, but these are far outweighed by the benefits of protection against CRS. The rubella vaccine’s legacy in the 1970s serves as a testament to the transformative potential of targeted immunization efforts.
Toddler and Baby Safety: Post-Vaccine Precautions for Young Siblings
You may want to see also
Frequently asked questions
In the 1970s, commonly available vaccines included those for diphtheria, tetanus, pertussis (DTaP), polio (oral and inactivated), measles, mumps, rubella (MMR), and smallpox.
Yes, the influenza (flu) vaccine was available in the 1970s, though it was less widely used compared to today and primarily recommended for high-risk groups.
Yes, the combined measles, mumps, and rubella (MMR) vaccine was introduced in the 1970s, replacing individual vaccines for each disease.
Yes, the smallpox vaccine was still in use in the 1970s, particularly in global eradication efforts. Routine vaccination in the U.S. ended in 1972, but it continued in other parts of the world until smallpox was declared eradicated in 1980.