The year 1945 marked a significant milestone in the history of medicine with the debut of the first inactivated influenza vaccine. Developed in response to the devastating 1918 influenza pandemic, this vaccine represented a breakthrough in preventing viral infections. Unlike live-attenuated vaccines, which use weakened forms of the virus, the inactivated influenza vaccine contained killed virus particles, rendering it incapable of causing disease while still eliciting a protective immune response. This innovation laid the foundation for modern vaccine technology and paved the way for the development of numerous other inactivated vaccines, revolutionizing public health and disease prevention.
| Characteristics | Values |
|---|---|
| Type of Vaccine | Inactivated (Whole-Cell) Pertussis Vaccine |
| Year of Debut | 1945 |
| Disease Targeted | Pertussis (Whooping Cough) |
| Mechanism | Contains killed Bordetella pertussis bacteria to stimulate immune response |
| Efficacy | ~80% effectiveness in preventing severe disease |
| Side Effects | Local reactions (pain, redness, swelling), fever, irritability, rare severe reactions |
| Administration Route | Intramuscular injection |
| Dose Schedule | Multiple doses (typically part of DTP/DTaP combination vaccines) |
| Age Group | Infants and young children (starting at 2 months) |
| Replacement | Largely replaced by acellular pertussis (aP) vaccines due to fewer side effects |
| Current Use | Rarely used in developed countries; still used in some low-income settings |
| Impact | Significantly reduced pertussis mortality and morbidity globally |
| Combination Vaccines | Often combined with Diphtheria and Tetanus (DTP/DTaP) |
| Storage Requirements | Refrigerated (2-8°C) |
| Manufacturer Examples | Early versions by various pharmaceutical companies; no longer widely produced |
Explore related products






What You'll Learn
![]()
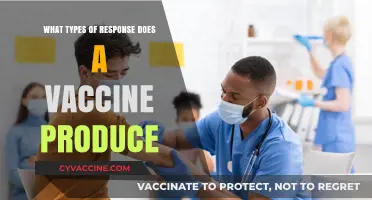
First inactivated flu vaccine
The year 1945 marked a pivotal moment in medical history with the debut of the first inactivated flu vaccine. Developed by researchers at the University of Michigan, this vaccine represented a breakthrough in the fight against influenza, a disease that had caused widespread morbidity and mortality for centuries. Unlike live-attenuated vaccines, which use a weakened form of the virus, inactivated vaccines contain viruses that have been killed, making them safer for individuals with compromised immune systems. This innovation laid the foundation for modern flu vaccination programs, which today protect millions of people worldwide.
From a technical standpoint, the production of the first inactivated flu vaccine involved a meticulous process. The virus was grown in fertilized chicken eggs, a method still widely used today, and then inactivated using formaldehyde. This ensured the virus could no longer replicate but retained its ability to stimulate an immune response. The vaccine was initially administered in two doses, spaced several weeks apart, to maximize immunity. While the dosage and formulation have evolved over the decades, the core principle remains the same: introducing the immune system to the virus in a safe, controlled manner.
One of the most significant advantages of the inactivated flu vaccine is its broad applicability. It was initially targeted at military personnel during World War II, as influenza posed a substantial threat to troop health. However, its success quickly led to its adoption for the general public, including children over six months of age, adults, and the elderly. For older adults, who are at higher risk of severe complications from the flu, this vaccine offered a critical layer of protection. Practical tips for recipients included monitoring for mild side effects, such as soreness at the injection site or low-grade fever, and scheduling annual vaccinations to account for evolving flu strains.
Comparatively, the debut of the inactivated flu vaccine in 1945 contrasts sharply with earlier attempts to combat influenza. During the 1918 Spanish flu pandemic, medical interventions were limited to rudimentary measures like quarantine and aspirin. The development of the inactivated vaccine demonstrated the power of scientific advancement and set a precedent for rapid vaccine development in response to public health crises. Its success also underscored the importance of international collaboration, as researchers shared data and techniques across borders to refine the vaccine’s efficacy.
Today, the legacy of the first inactivated flu vaccine endures in the annual flu shots administered globally. While newer technologies, such as mRNA vaccines, have emerged, the inactivated vaccine remains a cornerstone of preventive medicine. Its debut in 1945 not only saved countless lives but also transformed our approach to infectious disease control. As we face new challenges, from pandemic influenza to emerging viruses, the lessons learned from this pioneering vaccine continue to guide innovation and public health strategy.
Lyme Disease Vaccine: Hope on the Horizon for Prevention?
You may want to see also
Explore related products





![]()
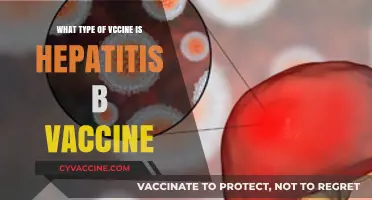
Jonas Salk's polio breakthrough
The year 1955, not 1945, marked a pivotal moment in medical history with the debut of Jonas Salk's inactivated poliovirus vaccine (IPV). This breakthrough came after years of devastating polio outbreaks that left thousands paralyzed or dead, particularly children. Salk's vaccine, administered via injection, used killed poliovirus to trigger an immune response without the risk of causing the disease itself. This approach contrasted with the later development of the oral polio vaccine (OPV) by Albert Sabin, which used a live but weakened virus.
Salk's IPV was a product of meticulous research and collaboration. His team at the University of Pittsburgh cultivated the poliovirus in monkey kidney cells, then inactivated it with formaldehyde to ensure safety. Clinical trials involving 1.8 million children in 1954 demonstrated the vaccine's efficacy, leading to its approval in 1955. The recommended dosage for children was three injections, spaced over several months, typically starting at 2 months of age. This regimen provided robust immunity, reducing polio cases in the U.S. by 90% within five years.
One of the most compelling aspects of Salk's breakthrough was his decision not to patent the vaccine. When asked who owned the patent, he famously replied, "Well, the people, I would say. There is no patent. Could you patent the sun?" This altruistic act ensured widespread accessibility, saving countless lives globally. However, the IPV's reliance on injections and the need for medical personnel limited its use in remote or resource-poor areas, paving the way for Sabin's OPV in the 1960s.
Implementing Salk's vaccine required careful planning. Parents were advised to adhere strictly to the vaccination schedule to ensure full protection. Side effects were minimal, typically limited to soreness at the injection site. Public health campaigns played a crucial role in dispelling myths and encouraging vaccination, a lesson relevant even today. For instance, storing the vaccine at 2–8°C (36–46°F) was essential to maintain its potency, a logistical challenge in some regions.
In retrospect, Salk's IPV was more than a medical achievement; it was a testament to the power of scientific collaboration and public trust. While it debuted a decade after the question's reference year of 1945, its impact on eradicating polio remains unparalleled. Today, as we face new global health challenges, Salk's legacy reminds us of the importance of innovation, accessibility, and collective action in safeguarding public health.
Puppy 8-in-1 Vaccine: Essential Protection for Your Furry Friend
You may want to see also
Explore related products






![]()
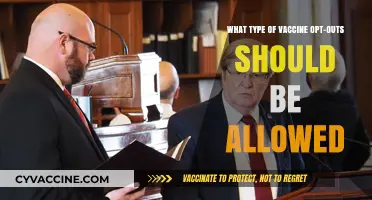
Mass production techniques
The year 1945 marked the debut of the inactivated influenza vaccine, a breakthrough that revolutionized disease prevention. This vaccine type, developed during World War II, relied on a killed version of the influenza virus to stimulate immunity without causing illness. Its success hinged not just on scientific innovation but on the mass production techniques that made it accessible to millions. These techniques laid the groundwork for modern vaccine manufacturing, blending precision, scalability, and safety.
One of the key mass production techniques employed was large-scale virus cultivation. Scientists grew influenza viruses in fertilized chicken eggs, a method still used today for many flu vaccines. Each egg could produce enough virus for multiple doses, enabling the rapid production of millions of vaccines. This process required strict quality control to ensure the virus was fully inactivated, typically using formaldehyde. For instance, a single batch could yield up to 10,000 doses, with each dose containing 15 micrograms of hemagglutinin antigen—the critical component for immune response.
Another critical technique was standardization and automation. Early vaccine production was labor-intensive, but the introduction of automated machinery streamlined processes like egg inoculation, incubation, and harvesting. This reduced human error and increased consistency. For example, automated systems could inoculate 1,000 eggs per hour, compared to the 100 eggs manually processed in the same time. Standardized protocols ensured that every dose met safety and efficacy criteria, such as maintaining a pH of 7.2 during virus inactivation.
Cold chain logistics emerged as a vital component of mass production. Inactivated vaccines require refrigeration to remain stable, typically between 2°C and 8°C. In 1945, this posed a challenge, but the development of insulated storage units and refrigerated transport systems ensured vaccines reached their destinations without spoiling. Practical tips for distribution included pre-cooling storage units and using temperature monitors to track conditions during transit. These measures were essential for maintaining vaccine potency, especially in remote or war-affected areas.
Finally, regulatory oversight and public health campaigns played a pivotal role in scaling production. Governments and health organizations established guidelines for vaccine safety and efficacy, ensuring mass-produced doses met rigorous standards. Public education campaigns, such as those during the 1947 influenza outbreak, encouraged widespread vaccination, driving demand and justifying increased production. For instance, the U.S. Public Health Service vaccinated over 10 million people in 1947, a feat made possible by these combined techniques.
In summary, the mass production techniques of 1945—large-scale virus cultivation, automation, cold chain logistics, and regulatory oversight—transformed the inactivated influenza vaccine from a scientific achievement into a public health tool. These innovations not only addressed the immediate needs of the time but also set the stage for future vaccine development, proving that scalability and accessibility are as crucial as the vaccine itself.
Understanding Vaccine-Induced Immunity: Types, Duration, and Protection Levels
You may want to see also
Explore related products





![]()
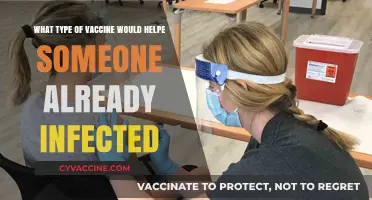
Impact on public health
The year 1945 marked the debut of the inactivated influenza vaccine, a groundbreaking development in the fight against a virus that had caused global pandemics, most notably the 1918 Spanish Flu. This vaccine type, unlike its live-attenuated counterparts, uses killed virus particles to trigger an immune response, making it safer for individuals with compromised immune systems. Its introduction was a pivotal moment in public health, offering a new tool to combat seasonal flu outbreaks and reduce the burden of influenza-related complications.
From an analytical perspective, the inactivated influenza vaccine’s impact on public health is measurable through reduced hospitalization rates and mortality. Studies show that annual vaccination can lower the risk of flu-related hospitalizations by 40–60% in the general population, with even higher efficacy in preventing severe outcomes in high-risk groups like the elderly and pregnant women. For instance, a standard dose (0.5 mL for adults) administered intramuscularly stimulates the production of antibodies within 2–4 weeks, providing protection during peak flu seasons. However, its effectiveness hinges on annual updates to match circulating strains, highlighting the need for ongoing surveillance and vaccine reformulation.
Instructively, the rollout of the inactivated influenza vaccine in 1945 set a precedent for mass vaccination campaigns, emphasizing accessibility and education. Public health initiatives, such as workplace clinics and school-based programs, have since become staples of flu prevention strategies. Practical tips for maximizing vaccine impact include scheduling vaccinations by October (before flu activity peaks) and ensuring high-risk individuals receive the appropriate formulation, such as the high-dose vaccine for those over 65. Combining vaccination with hygiene practices like handwashing and masking amplifies its protective effects, particularly in crowded settings.
Persuasively, the inactivated influenza vaccine’s debut underscored the importance of proactive public health measures in preventing widespread disease. Its introduction not only saved lives but also reduced economic burdens by decreasing absenteeism and healthcare costs. For example, a 10% increase in flu vaccination rates could save up to $1 billion annually in the U.S. alone. Critics often cite concerns about side effects, but data show that adverse reactions are rare, with the most common being mild soreness at the injection site. The vaccine’s benefits far outweigh these minimal risks, making it a cornerstone of global health strategies.
Comparatively, the inactivated influenza vaccine’s impact contrasts with that of earlier preventive measures, such as quarantine and limited antiviral treatments. While these methods were reactive, the vaccine represented a shift toward prevention, empowering individuals to take control of their health. Unlike live vaccines, its inactivated nature made it suitable for broader populations, including those with chronic conditions. This inclusivity has been critical in achieving herd immunity, particularly in densely populated areas. Over time, its success paved the way for the development of other inactivated vaccines, such as those for polio and hepatitis A, further solidifying its legacy in public health.
Roundworm vs. Tapeworm Vaccines: Key Differences and Uses Explained
You may want to see also
Explore related products






![]()
Shift from live to inactivated vaccines
The year 1945 marked a pivotal moment in vaccine history with the debut of the first inactivated influenza vaccine, a significant departure from the live, attenuated vaccines that had dominated earlier efforts. This shift was driven by the need for safer, more stable immunizations, particularly for vulnerable populations like the elderly and those with compromised immune systems. Inactivated vaccines, unlike their live counterparts, contain viruses or bacteria that have been killed, eliminating the risk of the pathogen reverting to a virulent form. This innovation laid the groundwork for a new era in vaccinology, balancing efficacy with enhanced safety profiles.
Consider the practical implications of this transition. Live vaccines, such as the early yellow fever vaccine, require careful handling and storage to maintain the viability of the attenuated pathogen. In contrast, inactivated vaccines are more robust, tolerating a wider range of temperatures and conditions. For instance, the 1945 influenza vaccine could be stored at standard refrigeration temperatures (2–8°C), making distribution and administration more feasible, especially in resource-limited settings. This logistical advantage became a critical factor in scaling up vaccination campaigns during global health crises.
From a safety perspective, the shift to inactivated vaccines addressed concerns about adverse reactions. Live vaccines, while highly effective, carry a small risk of causing disease in immunocompromised individuals. The inactivated polio vaccine (IPV), introduced in 1955 as a successor to the live oral polio vaccine (OPV), exemplifies this. IPV eliminated the rare but serious risk of vaccine-associated paralytic polio (VAPP), which occurred in approximately 1 in 2.7 million OPV recipients. This shift underscored the principle that vaccine development must prioritize minimizing harm without compromising immunity, a lesson that continues to guide modern vaccine design.
However, the transition was not without trade-offs. Inactivated vaccines often require multiple doses and adjuvants to achieve robust immunity, as they lack the inherent immunogenicity of live pathogens. For example, the 1945 influenza vaccine typically required a primary series of two doses, spaced 3–4 weeks apart, followed by annual boosters to account for viral drift. This regimen, while effective, placed greater demands on healthcare systems and individual compliance. Balancing convenience, cost, and efficacy remains a central challenge in vaccine development, highlighting the complexity of this evolutionary shift.
In conclusion, the debut of inactivated vaccines in 1945 represented a critical turning point in immunology, driven by the need for safer, more stable alternatives to live vaccines. This shift introduced practical benefits, such as improved storage and reduced risks, but also necessitated innovations to enhance immunogenicity. As we continue to refine vaccine technologies, the lessons from this transition remind us that progress in vaccinology is a delicate balance between safety, efficacy, and accessibility. Understanding this history equips us to address current and future challenges in global health.
Vaccine vs. Natural Immunity: Understanding the Key Differences
You may want to see also
Frequently asked questions
The inactivated influenza vaccine made its debut in 1945.
The first inactivated influenza vaccine was developed by Thomas Francis Jr. and his team at the University of Michigan, in collaboration with the U.S. Army.
The 1945 influenza vaccine was the first to use inactivated (killed) virus particles, which made it safer and more effective than earlier attempts using live or partially inactivated viruses.
The debut of the inactivated influenza vaccine in 1945 was significant because it marked the first successful large-scale production of a flu vaccine, paving the way for annual influenza vaccination programs and reducing the impact of flu epidemics.