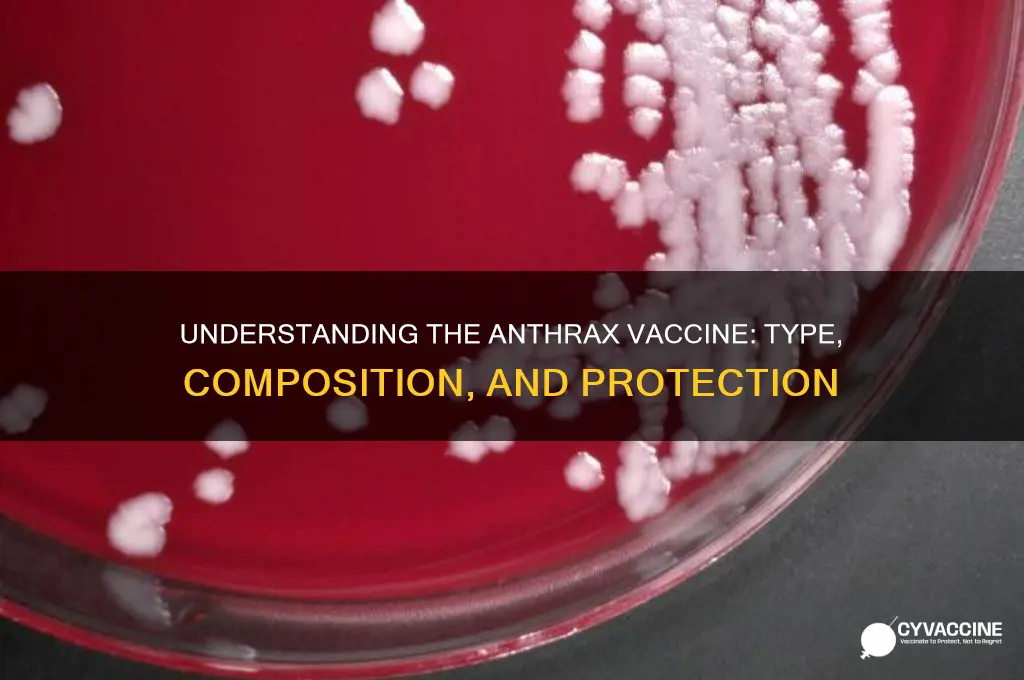
The anthrax vaccine is a biological preparation designed to provide immunity against anthrax, a potentially fatal disease caused by the bacterium *Bacillus anthracis*. It is classified as a subunit vaccine, meaning it contains specific components of the bacterium rather than the entire organism. The vaccine primarily targets protective antigen (PA), a key protein produced by *B. anthracis* during infection, which plays a critical role in the disease's pathogenicity. By stimulating the immune system to produce antibodies against PA, the vaccine effectively neutralizes the toxin and prevents the onset of anthrax. This type of vaccine has been widely used in both human and animal populations, particularly among individuals at high risk of exposure, such as military personnel, veterinarians, and laboratory workers. Its development and deployment have significantly contributed to reducing the threat of anthrax as a biological weapon and as a natural disease.
| Characteristics | Values |
|---|---|
| Vaccine Type | Subunit Vaccine |
| Specific Type | Recombinant Protein Vaccine |
| Target Antigen | Protective Antigen (PA) from Bacillus anthracis |
| Brand Names | BioThrax (U.S.), Anthrax Vaccine Adsorbed (AVA) |
| Route of Administration | Intramuscular Injection |
| Dose Schedule (Pre-exposure) | 3 doses: 0, 1, and 6 months, followed by annual boosters |
| Dose Schedule (Post-exposure) | 3 doses: 0, 2, and 4 weeks, plus antibiotics |
| Adjuvant | Aluminum hydroxide |
| Storage Temperature | 2°C to 8°C (36°F to 46°F) |
| Approval Status | FDA-approved for both pre-exposure prophylaxis and post-exposure prophylaxis (with antibiotics) |
| Primary Use | Prevention of anthrax disease in at-risk populations (e.g., military personnel, lab workers) |
| Efficacy | Demonstrated effectiveness in animal models; no large-scale human efficacy trials due to ethical considerations |
| Side Effects | Local reactions (pain, redness, swelling), fatigue, headache, muscle aches |
| Manufacturer | Emergent BioSolutions |
| Development Year | Licensed in 1970, modern formulation approved in 1998 |
Explore related products






What You'll Learn
- Live Attenuated vs. Inactivated: Anthrax vaccine is inactivated, meaning it uses killed bacteria to trigger immunity
- Component-Based Design: Contains purified parts of the anthrax bacterium, not the whole organism
- Adjuvant Inclusion: Aluminum hydroxide adjuvant enhances immune response to the vaccine components
- Protection Mechanism: Stimulates antibodies against anthrax toxin proteins, not the bacteria itself
- Approval and Use: Licensed by FDA in 1970, primarily for at-risk adults, not general public
![]()
Live Attenuated vs. Inactivated: Anthrax vaccine is inactivated, meaning it uses killed bacteria to trigger immunity
The anthrax vaccine stands apart from many others in its class due to its inactivated nature. Unlike live attenuated vaccines, which use weakened but still living pathogens to stimulate immunity, the anthrax vaccine employs killed *Bacillus anthracis* bacteria. This fundamental difference shapes its safety profile, efficacy, and administration protocol. For instance, the BioThrax vaccine, the only FDA-approved anthrax vaccine, contains purified extracts of the bacterium’s protective antigen (PA), a key component in triggering an immune response without the risk of causing disease.
From a practical standpoint, the inactivated nature of the anthrax vaccine makes it a safer option for specific populations. Live attenuated vaccines, while highly effective, carry a small risk of reverting to a virulent form or causing mild illness, particularly in immunocompromised individuals. In contrast, inactivated vaccines like BioThrax eliminate this risk entirely, making them suitable for people with weakened immune systems, such as those undergoing chemotherapy or living with HIV. However, this safety comes at a cost: inactivated vaccines often require multiple doses and adjuvants to achieve robust immunity. The anthrax vaccine, for example, is typically administered in a five-dose series over 18 months, followed by annual boosters for those at continued risk.
A comparative analysis highlights the trade-offs between live attenuated and inactivated vaccines. Live vaccines, like the MMR (measles, mumps, rubella) vaccine, often confer long-lasting immunity after just one or two doses due to their ability to mimic natural infection. Inactivated vaccines, however, rely on introducing non-replicating antigens, which the immune system may recognize as less threatening. This can result in a weaker initial response, necessitating additional doses and adjuvants like aluminum hydroxide to enhance immunogenicity. For the anthrax vaccine, this means a more complex dosing schedule but a significantly reduced risk of adverse effects, making it a preferred choice in high-risk scenarios like bioterrorism preparedness.
For those considering the anthrax vaccine, understanding its inactivated nature is crucial for managing expectations and adherence. Unlike a single-dose live vaccine, the anthrax vaccine’s multi-dose regimen requires commitment and planning. Practical tips include scheduling appointments well in advance, keeping a vaccination record, and discussing potential side effects (e.g., soreness at the injection site, mild fever) with a healthcare provider. Additionally, knowing that the vaccine targets only the protective antigen means it does not provide immediate protection against all components of the bacterium, underscoring the importance of completing the full series.
In conclusion, the inactivated design of the anthrax vaccine reflects a deliberate choice to prioritize safety over convenience. While it may not offer the simplicity of live attenuated vaccines, its ability to protect against a deadly pathogen without risk of infection makes it an invaluable tool in specific contexts. Whether for military personnel, lab workers, or individuals in high-threat areas, the anthrax vaccine’s inactivated formulation ensures that immunity can be achieved without compromising health, even if it demands a more rigorous vaccination schedule.
Double Puppy Vaccination: Potential Risks and What You Need to Know
You may want to see also
Explore related products






![]()
Component-Based Design: Contains purified parts of the anthrax bacterium, not the whole organism
The anthrax vaccine stands apart from many traditional vaccines due to its component-based design. Unlike live-attenuated or whole-cell vaccines, it doesn’t rely on introducing the entire bacterium into the body. Instead, it contains carefully purified parts of the *Bacillus anthracis* bacterium, specifically targeting the protective antigen (PA) protein, which plays a critical role in anthrax toxicity. This approach eliminates the risk of infection from the vaccine itself while focusing the immune response on the most relevant target.
This design choice is both strategic and safety-driven. By isolating the PA protein, the vaccine avoids the complexities and potential dangers of handling live or inactivated whole bacteria. The purification process ensures that only the essential component is delivered, minimizing the risk of adverse reactions. This is particularly important for anthrax, a disease with a high mortality rate when left untreated, as it allows for a focused and controlled immune response. For instance, the licensed anthrax vaccine in the U.S., BioThrax, contains 0.5 mg of PA per dose, administered in a series of shots over 18 months, followed by annual boosters for those at continued risk.
From a practical standpoint, this component-based approach simplifies storage and administration. The purified PA protein is more stable than whole-cell vaccines, reducing the need for stringent cold chain requirements. This makes it more feasible to distribute and administer in diverse settings, including remote or resource-limited areas. Additionally, the vaccine is approved for individuals aged 18 to 65, though off-label use in younger populations has been explored in high-risk scenarios, such as bioterrorism threats.
However, the component-based design isn’t without its limitations. While it effectively targets the PA protein, it doesn’t account for other bacterial components that might contribute to immunity. This has led to ongoing research into adjuvanted formulations, such as those containing aluminum hydroxide, to enhance the immune response. For example, the Anthrax Vaccine Adsorbed (AVA) uses an aluminum hydroxide adjuvant to improve the durability of protection. Recipients should be aware of potential side effects, such as soreness at the injection site or mild fever, which are generally mild and short-lived.
In conclusion, the component-based design of the anthrax vaccine represents a thoughtful balance of safety, efficacy, and practicality. By focusing on the purified PA protein, it provides targeted protection without the risks associated with whole-organism vaccines. For those in high-risk professions, such as military personnel or lab workers, understanding this design underscores the vaccine’s role in preventing a potentially deadly disease. Always consult healthcare providers for personalized advice, especially regarding dosage schedules and potential contraindications.
Is Skipping Child Vaccinations in NJ Against the Law?
You may want to see also
Explore related products






![]()
Adjuvant Inclusion: Aluminum hydroxide adjuvant enhances immune response to the vaccine components
The anthrax vaccine, specifically BioThrax (Anthrax Vaccine Adsorbed), is a critical tool in preventing a potentially deadly disease caused by Bacillus anthracis. Its formulation includes a key component: aluminum hydroxide adjuvant, which plays a pivotal role in enhancing the immune response. Adjuvants are substances added to vaccines to boost the body’s immune reaction to the antigen, ensuring a stronger and more durable defense. In the case of the anthrax vaccine, aluminum hydroxide acts as a delivery system, slowing the release of the antigen and directing it to immune cells for a more robust response.
From an analytical perspective, the inclusion of aluminum hydroxide in the anthrax vaccine is a strategic choice rooted in immunology. Aluminum salts, including aluminum hydroxide, have been used in vaccines since the 1930s due to their safety and efficacy. In the anthrax vaccine, the adjuvant binds to the protective antigen (PA) component, the primary target of the immune system. This binding process creates a depot effect, where the antigen remains localized at the injection site for a prolonged period. This slow release allows immune cells, such as dendritic cells, to process the antigen more effectively, leading to increased antibody production and a heightened immune memory. Studies have shown that vaccines without adjuvants often require higher doses or more frequent administrations to achieve comparable immunity, making aluminum hydroxide a practical and efficient solution.
For those administering or receiving the anthrax vaccine, understanding the role of aluminum hydroxide is essential. The vaccine is typically given in a series of five doses over 18 months, followed by annual boosters for individuals at continued risk, such as military personnel or lab workers. Each dose contains 0.8 mg of aluminum hydroxide, a level well within safe limits established by regulatory agencies. While some may experience mild side effects like soreness at the injection site, these are generally short-lived and outweighed by the vaccine’s protective benefits. It’s important to note that aluminum hydroxide is not absorbed systemically; it remains localized, minimizing potential risks.
Comparatively, the anthrax vaccine’s use of aluminum hydroxide sets it apart from other vaccines that employ different adjuvants or none at all. For instance, mRNA vaccines like those for COVID-19 use lipid nanoparticles to deliver genetic material, while some influenza vaccines contain oil-in-water emulsions. Aluminum hydroxide’s long history of safe use and its ability to enhance both humoral and cell-mediated immunity make it a preferred choice for subunit vaccines like the anthrax vaccine. Its inclusion ensures that even a relatively small amount of antigen can elicit a strong immune response, a critical factor in protecting against a disease as severe as anthrax.
In conclusion, the aluminum hydroxide adjuvant in the anthrax vaccine is a cornerstone of its effectiveness. By amplifying the immune response to the protective antigen, it ensures that recipients develop robust immunity with fewer doses and lower antigen concentrations. This adjuvant’s safety profile, combined with its immunological benefits, underscores its value in vaccine design. Whether you’re a healthcare provider, a recipient, or simply curious about vaccine science, understanding this component highlights the ingenuity behind modern immunization strategies.
Smallpox and Monkeypox: Are the Vaccines Similar?
You may want to see also
Explore related products






![]()
Protection Mechanism: Stimulates antibodies against anthrax toxin proteins, not the bacteria itself
The anthrax vaccine operates on a precise and innovative principle: it targets the toxins produced by the *Bacillus anthracis* bacteria rather than the bacteria itself. This approach is rooted in the understanding that anthrax’s lethality stems primarily from its potent toxins—lethal factor, edema factor, and protective antigen—which cause tissue damage, immune suppression, and systemic shock. By focusing on these toxin proteins, the vaccine circumvents the need to neutralize the entire bacterium, a strategy that simplifies the immune response and enhances efficacy.
Analytically, this mechanism is a strategic shift from traditional vaccines, which often aim to eliminate the pathogen directly. The anthrax vaccine, specifically BioThrax (Anthrax Vaccine Adsorbed), contains a cell-free filtrate of the *Bacillus anthracis* culture, purified to isolate the protective antigen (PA) protein. When administered in a series of doses—typically 0.5 mL intramuscularly in a 3-dose primary series over 6 months, followed by boosters—the vaccine stimulates the production of antibodies specifically tailored to neutralize PA. This antibody response blocks the toxin’s ability to bind to cells, effectively disarming anthrax’s most dangerous weapon without engaging the bacteria directly.
From an instructive standpoint, this protection mechanism has practical implications for vaccination protocols. For instance, individuals at high risk, such as military personnel or lab workers, must adhere strictly to the dosing schedule: initial doses at 0, 1, and 6 months, followed by annual boosters. The vaccine’s focus on toxin proteins also means it is less likely to cause severe bacterial infections in immunocompromised individuals, a critical advantage over live or attenuated vaccines. However, recipients should monitor for mild side effects, such as soreness at the injection site or fatigue, which typically resolve within days.
Comparatively, this toxin-based approach mirrors the strategy of vaccines like the tetanus toxoid, which also targets bacterial toxins rather than the pathogen. However, the anthrax vaccine’s specificity to protective antigen sets it apart, as PA is the critical component for toxin assembly. This focused immunity explains why the vaccine is effective against all forms of anthrax—cutaneous, inhalation, and gastrointestinal—despite not targeting the bacteria itself. It’s a testament to the principle that sometimes, neutralizing the weapon is more effective than defeating the enemy.
Descriptively, the immune response triggered by the anthrax vaccine is a symphony of precision. Upon injection, antigen-presenting cells recognize the protective antigen and activate B cells, which differentiate into plasma cells producing PA-specific antibodies. These antibodies circulate in the bloodstream, ready to intercept and neutralize PA if exposure occurs. This process is akin to deploying a specialized defense force trained to disarm a specific threat, ensuring rapid and effective protection without the collateral damage of a broader immune assault.
In conclusion, the anthrax vaccine’s protection mechanism is a masterclass in targeted immunity. By stimulating antibodies against anthrax toxin proteins, it offers robust defense without engaging the bacteria directly. This approach not only enhances safety and efficacy but also sets a precedent for vaccine design in combating toxin-mediated diseases. For those at risk, understanding this mechanism underscores the importance of adhering to vaccination schedules and appreciating the vaccine’s role as a precise, life-saving tool.
Alternative Healing: How Antivaxxers Approach Disease Without Vaccines
You may want to see also
Explore related products




![]()
Approval and Use: Licensed by FDA in 1970, primarily for at-risk adults, not general public
The anthrax vaccine, licensed by the FDA in 1970, is a targeted intervention designed for specific populations rather than a broad public health tool. Its approval was rooted in the need to protect individuals at highest risk of exposure to *Bacillus anthracis*, the bacterium causing anthrax. Unlike vaccines for diseases like influenza or measles, which are widely administered, the anthrax vaccine’s use is deliberately restricted. This narrow focus reflects both its development history and the unique threat anthrax poses—primarily occupational or bioterrorism-related rather than endemic.
Consider the vaccine’s administration protocol: a five-dose series given over 18 months, followed by annual boosters for continued protection. This regimen is not trivial, requiring commitment from recipients and coordination from healthcare providers. The initial doses are administered at 0, 2, 4, 6, and 12 months, with boosters every year thereafter for those at sustained risk. This schedule underscores the vaccine’s purpose: to build and maintain immunity in individuals whose occupations or environments expose them to anthrax, such as veterinarians, livestock handlers, and military personnel.
The decision to limit the vaccine’s use to at-risk adults, rather than the general public, is both practical and strategic. Anthrax is not a widespread disease; its incidence is low, and transmission is primarily through contact with infected animals or contaminated materials. Mass vaccination would be inefficient and unnecessary, diverting resources from more pressing public health needs. Instead, the vaccine serves as a critical tool for those in high-exposure roles, ensuring they can continue their work safely. For example, military personnel deployed to regions where bioterrorism is a concern rely on this vaccine to mitigate the risk of weaponized anthrax.
Practical considerations also shape the vaccine’s use. Side effects, though generally mild, include soreness at the injection site, fatigue, and muscle aches. These are manageable for healthy adults but could be more problematic for individuals with compromised immune systems or chronic conditions. Thus, the vaccine is contraindicated for pregnant women and those with severe allergies to its components. Healthcare providers must carefully screen candidates to ensure safety and efficacy, further emphasizing the vaccine’s specialized role.
In summary, the anthrax vaccine’s FDA approval in 1970 marked the creation of a niche yet vital tool in public health. Its use is tailored to protect those most vulnerable to anthrax exposure, balancing efficacy with practicality. By focusing on at-risk adults rather than the general population, the vaccine maximizes its impact while minimizing unnecessary administration. This targeted approach serves as a model for how vaccines can be deployed strategically to address specific threats, ensuring resources are allocated where they are most needed.
Texas Vaccine Ban: Separating Fact from Fiction with Snopes
You may want to see also
Frequently asked questions
The anthrax vaccine is a cell-free filtrate vaccine, meaning it contains no whole bacteria cells but instead uses purified proteins and toxins from the *Bacillus anthracis* bacterium.
No, the anthrax vaccine does not contain live bacteria. It is made from a sterile filtrate of the bacterium’s protective antigen (PA) protein, which is non-infectious.
The currently approved anthrax vaccine (BioThrax) is not a recombinant vaccine. However, newer anthrax vaccines in development, such as the recombinant protective antigen (rPA) vaccine, use genetically engineered proteins.
Yes, the anthrax vaccine (BioThrax) contains aluminum hydroxide as an adjuvant to enhance the immune response to the protective antigen (PA) protein.
No, the anthrax vaccine is not an mRNA vaccine. It is a protein-based vaccine that uses a purified component of the bacterium to stimulate immunity.