The COVID-19 pandemic has led to the rapid development and deployment of multiple coronavirus vaccines, each with unique characteristics and mechanisms of action. Understanding the differences between these vaccines is crucial for informed decision-making and public health strategies. Key distinctions include the type of technology used, such as mRNA (e.g., Pfizer-BioNTech, Moderna), viral vector (e.g., AstraZeneca, Johnson & Johnson), or inactivated virus (e.g., Sinovac, Sinopharm), as well as variations in efficacy rates, dosing regimens, storage requirements, and potential side effects. These differences are influenced by factors like the target population, regional availability, and ongoing research on long-term immunity and effectiveness against emerging variants. Comparing these vaccines highlights the diversity of scientific approaches in combating the virus and underscores the importance of global vaccination efforts tailored to specific needs.
Explore related products






What You'll Learn
- Vaccine Technologies: mRNA, viral vector, protein subunit, and whole virus differences explained
- Efficacy Rates: Comparison of effectiveness against COVID-19 symptoms and hospitalization
- Side Effects: Common reactions, severity, and duration for each vaccine type
- Dosage & Schedule: Number of shots, timing, and booster recommendations per vaccine
- Approval Status: Emergency use, full approval, and global regulatory differences
![]()
Vaccine Technologies: mRNA, viral vector, protein subunit, and whole virus differences explained
The COVID-19 pandemic spurred an unprecedented global effort to develop vaccines using diverse technologies, each with unique mechanisms and implications. Four primary platforms emerged: mRNA, viral vector, protein subunit, and whole virus. Understanding their differences is crucial for informed decision-making and addressing vaccine hesitancy.
MRNA vaccines, like Pfizer-BioNTech and Moderna, operate by delivering genetic instructions to cells. These instructions prompt the production of a harmless spike protein, mimicking SARS-CoV-2, which triggers an immune response. Notably, mRNA does not alter DNA; it degrades after use. A standard regimen involves two doses, 3–4 weeks apart, with a booster recommended 6 months later for sustained immunity. These vaccines boast high efficacy (90–95% initially) and rapid development timelines, but require ultra-cold storage, complicating distribution in resource-limited settings.
Viral vector vaccines, such as AstraZeneca and Johnson & Johnson, use a modified adenovirus to transport genetic material encoding the spike protein. Unlike mRNA vaccines, they do not require extreme refrigeration, making them more accessible globally. AstraZeneca typically requires two doses, 4–12 weeks apart, while Johnson & Johnson offers a single-dose regimen, appealing for hard-to-reach populations. However, rare side effects like thrombosis with thrombocytopenia syndrome (TTS) have been reported, primarily in younger adults, prompting age-based restrictions in some countries.
Protein subunit vaccines, exemplified by Novavax, introduce a lab-created spike protein directly into the body. This approach avoids genetic material, potentially easing concerns about novel technologies. Novavax’s two-dose series, administered 3 weeks apart, has shown 90% efficacy and a favorable safety profile, including reduced risk of myocarditis compared to mRNA vaccines. Its storage at standard refrigerator temperatures enhances distribution feasibility, particularly in low-income regions.
Whole virus vaccines, such as Sinopharm and Sinovac, use inactivated SARS-CoV-2 particles to stimulate immunity. This traditional method has been employed for decades in vaccines like influenza. A typical regimen involves two doses, 2–4 weeks apart, with a third dose often recommended due to lower initial efficacy (50–80%). While these vaccines are stable at standard refrigeration temperatures, their efficacy against variants like Omicron has been less robust, necessitating frequent boosters.
Practical takeaways: mRNA vaccines offer high efficacy but pose logistical challenges; viral vectors provide convenience but carry rare risks; protein subunits balance safety and accessibility; and whole virus vaccines rely on proven technology but may require more frequent doses. Choosing a vaccine depends on availability, individual health risks, and regional variant prevalence. Always consult healthcare providers for personalized advice.
How Vaccines Work: A Journey Through Your Immune System
You may want to see also
Explore related products






![]()
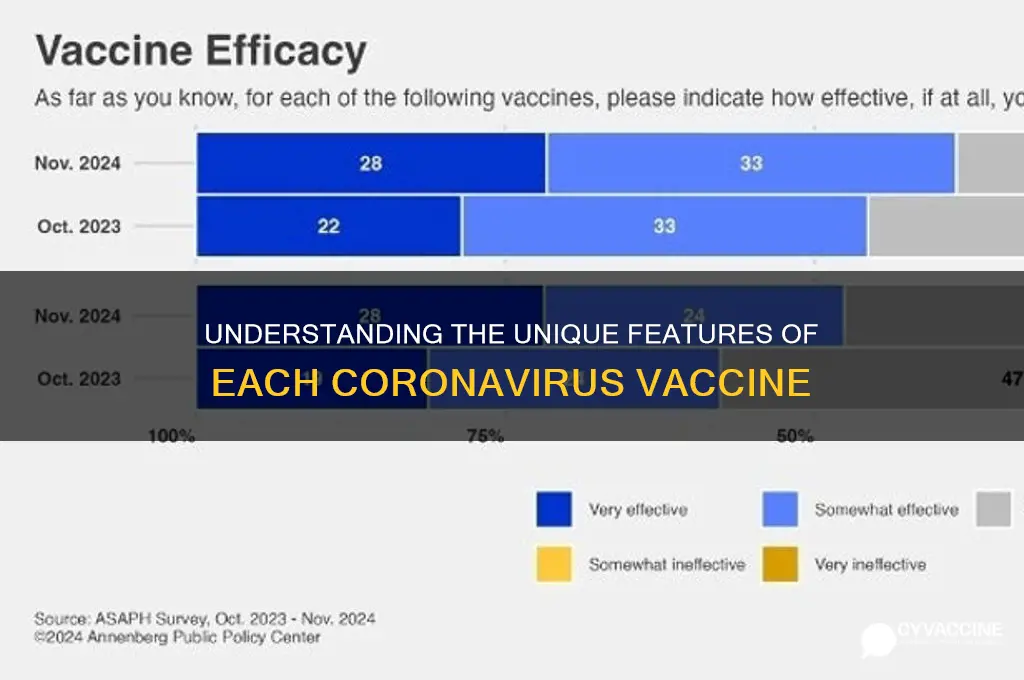
Efficacy Rates: Comparison of effectiveness against COVID-19 symptoms and hospitalization
The efficacy rates of COVID-19 vaccines are a critical measure of their ability to prevent symptoms and hospitalization, but these rates vary significantly across different vaccines and populations. For instance, the Pfizer-BioNTech mRNA vaccine demonstrated 95% efficacy in preventing symptomatic COVID-19 in clinical trials, while the Oxford-AstraZeneca viral vector vaccine showed 70-80% efficacy depending on dosing intervals. These numbers, however, are not static; real-world data often reveals lower but still substantial effectiveness due to factors like variant emergence and population health differences. Understanding these nuances is essential for informed decision-making.
Consider the impact of dosage and administration. Pfizer-BioNTech’s two-dose regimen, administered 21 days apart, achieved its high efficacy in trials involving participants aged 16 and older. In contrast, Moderna’s mRNA vaccine, given 28 days apart, showed 94.1% efficacy in a similar demographic. The Oxford-AstraZeneca vaccine’s efficacy was influenced by dosing intervals: a 12-week gap between doses resulted in higher efficacy than a shorter interval. Practical tip: Follow the recommended dosing schedule for your vaccine, as deviations can reduce effectiveness. For example, delaying the second dose of an mRNA vaccine beyond the advised timeframe may compromise immunity.
When comparing vaccines, it’s crucial to examine their performance against hospitalization, a more severe outcome. All authorized vaccines have proven highly effective in preventing severe illness and hospitalization. For example, real-world data from the UK showed that two doses of Pfizer-BioNTech and Oxford-AstraZeneca vaccines reduced hospitalization risk by over 90% against the Alpha variant. However, efficacy against newer variants like Delta and Omicron has waned, emphasizing the need for booster doses. Persuasive point: While breakthrough infections can occur, vaccination remains the most effective tool to prevent severe COVID-19 outcomes, particularly in vulnerable populations such as the elderly and immunocompromised.
A comparative analysis reveals that mRNA vaccines (Pfizer-BioNTech and Moderna) generally outperform viral vector vaccines (Oxford-AstraZeneca and Johnson & Johnson) in terms of symptom prevention, but all significantly reduce hospitalization risk. Johnson & Johnson’s single-dose vaccine, for instance, showed 72% efficacy against symptomatic COVID-19 in the U.S. but 85% efficacy against severe disease. This highlights the vaccines’ tiered effectiveness: while they may not always prevent infection, they excel at protecting against critical illness. Takeaway: Choose the vaccine available to you, as any vaccination is far superior to none in preventing severe outcomes.
Finally, age and health status play a role in vaccine efficacy. Clinical trials often exclude older adults or those with comorbidities, yet real-world data shows that efficacy tends to decrease in these groups. For example, Pfizer-BioNTech’s vaccine was 94% effective in preventing hospitalization in adults aged 65-74 but dropped to 74% in those over 85. Practical tip: If you’re in a high-risk category, discuss booster doses and additional precautions with your healthcare provider. Monitoring local variant prevalence and staying updated with vaccine recommendations can further optimize protection.
Sam's Club: J&J Vaccine Availability and Access
You may want to see also
Explore related products






![]()
Side Effects: Common reactions, severity, and duration for each vaccine type
All COVID-19 vaccines authorized for use have been rigorously tested for safety, but side effects are a normal part of the body's immune response. Understanding these reactions is crucial for informed decision-making. Let's break down the common side effects, their severity, and how long they typically last for the three main vaccine types: mRNA (Pfizer-BioNTech, Moderna), viral vector (Johnson & Johnson), and protein subunit (Novavax).
MRNA Vaccines (Pfizer-BioNTech, Moderna):
These vaccines, which teach cells to produce a harmless piece of the virus’s spike protein, often cause more noticeable side effects after the second dose. Common reactions include pain or swelling at the injection site, fatigue, headache, muscle pain, chills, fever, and nausea. For Pfizer, these symptoms usually peak within 24–48 hours post-vaccination and resolve within 1–3 days. Moderna’s side effects tend to be slightly more intense and longer-lasting, often persisting for 2–4 days, particularly after the second dose. Both vaccines are administered in two shots, typically 3–4 weeks apart for Pfizer and 4 weeks apart for Moderna.
Viral Vector Vaccine (Johnson & Johnson):
This single-dose vaccine uses a modified adenovirus to deliver genetic material. Side effects are generally milder than mRNA vaccines but include injection site pain, headache, fatigue, muscle aches, and nausea. These symptoms typically appear within 1–2 days and last 1–2 days. A rare but serious risk is thrombosis with thrombocytopenia syndrome (TTS), occurring in about 7 per 1 million vaccinated women aged 18–49. For this reason, the CDC recommends mRNA vaccines over Johnson & Johnson for most individuals.
Protein Subunit Vaccine (Novavax):
Novavax delivers the virus’s spike protein directly, paired with an adjuvant to enhance immune response. Common side effects include injection site tenderness, fatigue, headache, and muscle pain. These reactions are typically mild to moderate, appearing within 1–2 days and resolving within 1–3 days. Administered in two doses, 3–8 weeks apart, Novavax is a good option for those hesitant about mRNA or viral vector technologies.
Practical Tips:
- Schedule vaccinations when you can rest afterward, especially for mRNA vaccines.
- Use over-the-counter pain relievers like acetaminophen or ibuprofen for discomfort, but avoid taking them preemptively unless advised by a doctor.
- Stay hydrated and dress comfortably for your appointment.
- Monitor for severe reactions, such as difficulty breathing or persistent pain, and seek medical attention if they occur.
Understanding these differences empowers individuals to choose the vaccine that aligns best with their health needs and preferences.
MMR Vaccine and Colds: Should Your Child Get Vaccinated?
You may want to see also
Explore related products






![]()
Dosage & Schedule: Number of shots, timing, and booster recommendations per vaccine
The COVID-19 vaccines differ significantly in their dosage and scheduling requirements, which can impact their effectiveness and convenience. For instance, the Pfizer-BioNTech and Moderna vaccines both require two initial doses, but the timing between shots varies: Pfizer’s doses are administered 3 weeks apart, while Moderna’s are given 4 weeks apart. This difference is rooted in each vaccine’s formulation and clinical trial data, which optimized immune response at these intervals. Understanding these schedules is crucial for ensuring full protection, as deviating from the recommended timing may reduce efficacy.
Booster recommendations further highlight the vaccines’ distinct schedules. Pfizer and Moderna boosters are advised 5 months after the second dose for individuals aged 12 and older, while adults aged 50 and older may receive a second booster 4 months later. In contrast, the Johnson & Johnson (J&J) vaccine, which requires only a single initial dose, recommends a booster shot 2 months after the first dose for all adults. This accelerated timeline reflects the J&J vaccine’s lower initial efficacy compared to its mRNA counterparts. For immunocompromised individuals, additional doses are often required, with specific intervals tailored to their vaccine type.
Practical tips can help individuals navigate these schedules. For example, setting calendar reminders ensures timely receipt of doses, especially for vaccines with shorter intervals like Pfizer. Additionally, keeping a record of vaccination dates and types is essential for booster eligibility, as recommendations may evolve with new variants or research. Parents should note that Pfizer is the only vaccine authorized for children under 18, with a lower dosage (10 micrograms per shot for ages 5–11) compared to adults (30 micrograms). This age-specific dosing underscores the importance of following guidelines tailored to different populations.
Comparatively, the Novavax vaccine, a protein subunit option, offers another dosage schedule: two doses 3 weeks apart, similar to Pfizer. However, it is not yet approved for boosters, making it a distinct choice for those seeking an alternative to mRNA vaccines. This diversity in schedules emphasizes the need for personalized decision-making based on individual health needs, availability, and preferences. Ultimately, adhering to the recommended dosage and timing for each vaccine maximizes protection against severe illness, hospitalization, and death from COVID-19.
US Vaccine Shortage: Fact or Fiction? Analyzing Current Supply Challenges
You may want to see also
Explore related products






![]()
Approval Status: Emergency use, full approval, and global regulatory differences
The approval status of COVID-19 vaccines varies widely, reflecting the urgency of the pandemic and the diverse regulatory frameworks across the globe. Emergency Use Authorization (EUA) has been a critical tool, allowing vaccines to be distributed rapidly in response to the public health crisis. For instance, the Pfizer-BioNTech vaccine received EUA from the U.S. Food and Drug Administration (FDA) in December 2020, enabling its immediate use while clinical trials continued. This expedited process required manufacturers to provide evidence of safety and efficacy from Phase 3 trials, but without the extensive long-term data typically needed for full approval. Similarly, the Moderna and Johnson & Johnson vaccines followed suit, receiving EUA shortly after. These authorizations were pivotal in scaling up vaccination campaigns, but they also sparked questions about the rigor of the review process.
Full approval, on the other hand, demands a more comprehensive evaluation, including longer-term follow-up data to confirm safety and efficacy. In August 2021, the Pfizer-BioNTech vaccine became the first to receive full FDA approval for individuals aged 16 and older, followed by an expanded approval for those aged 12–15 in October 2021. This shift from EUA to full approval provided additional confidence to the public and healthcare providers, as it required at least six months of follow-up data on vaccine recipients. Full approval also allows vaccines to be marketed and administered without the constraints of an emergency declaration, potentially increasing accessibility. However, the process is time-consuming, which is why EUA remains a vital mechanism during crises.
Global regulatory differences further complicate the approval landscape. For example, the Oxford-AstraZeneca vaccine, widely used in Europe and low-income countries, faced delays in U.S. authorization due to differing regulatory requirements and data submission timelines. The European Medicines Agency (EMA) granted conditional marketing authorization, a process similar to EUA but tailored to the EU’s legal framework. In contrast, China’s Sinopharm and Sinovac vaccines received emergency approval in several countries but were not authorized in the U.S. or EU due to concerns over transparency and data standards. These disparities highlight the challenges of harmonizing regulatory processes across jurisdictions, even during a global health emergency.
Practical implications of these approval statuses are significant for individuals and healthcare systems. For instance, EUA vaccines may not be accepted for travel or employment requirements in certain regions, whereas fully approved vaccines carry broader recognition. Additionally, age-specific approvals—such as the Pfizer vaccine for children as young as 5 years old—require careful consideration of dosage, with younger age groups receiving lower doses (e.g., 10 micrograms for children 5–11, compared to 30 micrograms for adults). Understanding these distinctions empowers individuals to make informed decisions and navigate the complexities of vaccine availability and acceptance globally.
In conclusion, the approval status of COVID-19 vaccines—whether under emergency use, full approval, or varying global regulations—shapes their accessibility, public trust, and practical utility. While EUA has been instrumental in accelerating vaccine distribution, full approval provides a higher level of assurance. Global regulatory differences, however, underscore the need for international cooperation and standardized criteria to ensure equitable access and consistent safety standards. Staying informed about these nuances is essential for individuals and policymakers alike, as they continue to navigate the evolving landscape of pandemic response.
Church Attendance: Vaccination Requirements and Religious Exemptions
You may want to see also
Frequently asked questions
mRNA vaccines (Pfizer and Moderna) use genetic material called mRNA to teach cells to produce a harmless piece of the coronavirus spike protein, triggering an immune response. Viral vector vaccines (Johnson & Johnson) use a modified, harmless virus to deliver genetic instructions to cells to produce the spike protein, prompting immunity.
Pfizer and Moderna vaccines typically require two doses (with a recommended booster), while the Johnson & Johnson vaccine is administered as a single dose (with a booster recommended for some groups).
Side effects are generally mild to moderate across all vaccines but may vary. mRNA vaccines (Pfizer and Moderna) commonly cause fatigue, headache, and muscle pain, often more pronounced after the second dose. The Johnson & Johnson vaccine is associated with fewer systemic side effects but has a rare risk of blood clots with low platelets.
Pfizer and Moderna vaccines have shown around 90-95% efficacy against severe illness and hospitalization in clinical trials, while the Johnson & Johnson vaccine has shown around 66-72% efficacy in preventing moderate to severe disease, depending on the region. All vaccines remain highly effective at preventing severe outcomes.