Vaccines are essential tools in preventing infectious diseases, and they work by training the immune system to recognize and combat pathogens. Two prominent types of vaccines are mRNA vaccines and protein vaccines, each with distinct mechanisms and characteristics. mRNA vaccines, such as those developed for COVID-19 by Pfizer-BioNTech and Moderna, deliver genetic material (messenger RNA) that instructs cells to produce a specific viral protein, triggering an immune response. In contrast, protein vaccines, like Novavax’s COVID-19 vaccine, directly introduce a purified viral protein (antigen) into the body, bypassing the need for cellular protein synthesis. While mRNA vaccines harness the body’s own machinery to produce the antigen, protein vaccines rely on pre-manufactured proteins, often combined with adjuvants to enhance immunity. Understanding these differences is crucial for appreciating their efficacy, storage requirements, and potential applications in modern medicine.
| Characteristics | mRNA Vaccine | Protein Vaccine |
|---|---|---|
| Mechanism of Action | Delivers genetic material (mRNA) encoding a viral protein (e.g., spike protein) into cells, where it is translated into protein, triggering an immune response. | Directly delivers a pre-made viral protein (e.g., spike protein) to the immune system. |
| Type of Antigen | Produces antigen (protein) inside the body's cells. | Contains the antigen (protein) itself, ready for immune recognition. |
| Immune Response | Stimulates both humoral (antibody) and cellular (T-cell) immunity. | Primarily stimulates humoral immunity (antibody production). |
| Storage & Stability | Requires ultra-cold storage (-70°C to -20°C) for Pfizer-BioNTech, -20°C for Moderna; less stable due to mRNA fragility. | More stable, typically stored at 2°C to 8°C (refrigerator temperature). |
| Administration | Typically given intramuscularly (e.g., Pfizer-BioNTech, Moderna). | Intramuscular or subcutaneous injection (e.g., Novavax). |
| Dose Frequency | Usually requires 2 doses (3 weeks to 1 month apart) for full efficacy. | Typically requires 2 doses (3-4 weeks apart) for full efficacy. |
| Booster Shots | Boosters recommended due to waning immunity over time. | Boosters may be needed but generally less frequently than mRNA vaccines. |
| Technology | Newer technology, first approved for widespread use during the COVID-19 pandemic. | Older, well-established technology (e.g., hepatitis B, HPV vaccines). |
| Side Effects | Common side effects include pain at injection site, fatigue, headache, muscle pain, and fever. | Similar side effects but generally milder; may include injection site pain and fatigue. |
| Efficacy | High efficacy (90-95% against symptomatic COVID-19 for Pfizer and Moderna). | High efficacy (e.g., Novavax reported ~90% efficacy against COVID-19). |
| Allergies | Rare cases of severe allergic reactions (anaphylaxis) reported. | Lower risk of severe allergic reactions compared to mRNA vaccines. |
| Cost | Generally higher production and storage costs due to mRNA technology. | Lower production and storage costs; more cost-effective in some cases. |
| Global Accessibility | Limited accessibility in low-resource settings due to storage requirements. | Easier to distribute globally due to simpler storage and handling requirements. |
| Examples | Pfizer-BioNTech, Moderna COVID-19 vaccines. | Novavax COVID-19 vaccine, hepatitis B vaccine, HPV vaccine. |
Explore related products






What You'll Learn
- mRNA Mechanism: Delivers genetic instructions to cells to produce specific proteins, triggering immune response
- Protein Mechanism: Contains pre-made proteins to directly stimulate the immune system without genetic material
- Storage Requirements: mRNA vaccines need ultra-cold storage; protein vaccines are more stable at standard refrigeration
- Immune Response: mRNA elicits broader immune reactions; protein vaccines focus on specific antigens
- Development Speed: mRNA vaccines are faster to produce; protein vaccines require more complex manufacturing
![]()
mRNA Mechanism: Delivers genetic instructions to cells to produce specific proteins, triggering immune response
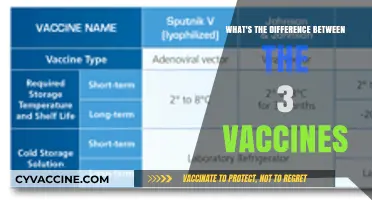
The mRNA vaccine mechanism is a marvel of precision engineering, delivering a set of genetic instructions to cells that act as a blueprint for producing specific proteins. Unlike traditional vaccines that introduce a weakened or inactivated pathogen, mRNA vaccines provide only the information needed to create a harmless piece of the virus, typically the spike protein found on the surface of SARS-CoV-2. Once injected, lipid nanoparticles protect the fragile mRNA as it enters cells, primarily in the deltoid muscle at the injection site. Inside the cell, the mRNA hijacks the ribosomes, the cell’s protein factories, to synthesize the viral protein. This process mimics a natural infection, but without the risk of causing disease, as the mRNA does not enter the cell’s nucleus or alter DNA. For instance, the Pfizer-BioNTech COVID-19 vaccine delivers 30 micrograms of mRNA in a two-dose regimen, spaced 3–4 weeks apart for individuals aged 12 and older, triggering a robust immune response.
Consider the immune system’s reaction to this process: as cells produce the viral protein, they display it on their surface, flagging it as foreign. Antigen-presenting cells (APCs) then engulf these proteins and transport them to lymph nodes, where they activate T cells and B cells. B cells, in particular, differentiate into plasma cells that secrete antibodies specifically tailored to neutralize the viral protein. This targeted response is both efficient and effective, as the body learns to recognize and combat the pathogen without being exposed to it directly. Studies show that mRNA vaccines like Moderna’s, which uses a 100-microgram dose for the first injection and a 50-microgram booster, can elicit antibody levels significantly higher than those observed in recovered COVID-19 patients, offering superior protection.
One of the key advantages of mRNA vaccines is their adaptability. The technology can be rapidly redesigned to target new variants or entirely different pathogens by simply updating the mRNA sequence. For example, when the Omicron variant emerged, Pfizer and Moderna were able to develop updated boosters within months, a process that would have taken years with traditional vaccine platforms. This flexibility is particularly valuable in the face of evolving viruses or emerging infectious diseases. However, it’s crucial to store mRNA vaccines properly—Pfizer’s vaccine requires ultra-cold storage at -90°C to -60°C, while Moderna’s can be stored at standard freezer temperatures (-25°C to -15°C)—to ensure the mRNA remains stable and effective.
Despite their effectiveness, mRNA vaccines are not without challenges. Some individuals may experience side effects such as fatigue, headache, or pain at the injection site, which are generally mild and resolve within a few days. These symptoms are a sign that the immune system is responding as intended. For optimal results, recipients should stay hydrated, rest, and avoid strenuous activity immediately after vaccination. Additionally, while mRNA vaccines are safe for most age groups, ongoing research is refining their use in younger children and immunocompromised populations. For instance, the Pfizer vaccine was initially approved for adults before being tested and approved for adolescents and, later, children as young as 5 years old, with adjusted dosages to balance efficacy and safety.
In conclusion, the mRNA mechanism represents a groundbreaking approach to vaccination, combining molecular precision with immunological ingenuity. By teaching cells to produce specific proteins, these vaccines harness the body’s own machinery to mount a targeted immune response. Their rapid development, high efficacy, and adaptability make them a powerful tool in combating infectious diseases. As the technology evolves, it holds promise not only for pandemics but also for cancers, genetic disorders, and other conditions where protein production plays a critical role. For now, following vaccination guidelines—such as completing the full dose series and staying informed about booster recommendations—ensures maximum protection for individuals and communities alike.
Essential Baby Vaccines: The Bare Minimum for Infant Health
You may want to see also
Explore related products

$11.93 $21.99





![]()
Protein Mechanism: Contains pre-made proteins to directly stimulate the immune system without genetic material
Protein-based vaccines operate on a straightforward principle: they deliver pre-made proteins directly to the immune system, bypassing the need for genetic material. Unlike mRNA vaccines, which instruct cells to produce a specific protein, protein vaccines provide the antigen itself, ready for immune recognition. This approach is exemplified by the Novavax COVID-19 vaccine, which uses a recombinant spike protein to trigger an immune response. The absence of genetic material eliminates concerns about integration into the host genome, offering a safety profile that appeals to those wary of newer mRNA technology.
Consider the administration process: protein vaccines typically require a two-dose regimen, with doses spaced 3–4 weeks apart. For instance, the Novavax vaccine is administered intramuscularly, with each dose containing 5 micrograms of the spike protein. This dosing schedule is designed to prime the immune system effectively, producing antibodies and memory cells for long-term protection. Notably, protein vaccines often incorporate adjuvants, such as Matrix-M in Novavax, to enhance the immune response, ensuring robust protection even with smaller protein quantities.
One of the key advantages of protein vaccines lies in their stability and storage requirements. Unlike mRNA vaccines, which demand ultra-cold storage, protein vaccines can be stored at standard refrigerator temperatures (2–8°C). This makes them more accessible in regions with limited cold-chain infrastructure, particularly in low- and middle-income countries. For healthcare providers, this translates to simpler logistics and reduced risk of vaccine spoilage during distribution.
However, protein vaccines are not without limitations. Their production process is often more complex and time-consuming compared to mRNA vaccines, as it involves culturing cells to express and purify the target protein. This can delay vaccine development during emerging pandemics, where rapid response is critical. Additionally, while protein vaccines are generally well-tolerated, side effects such as injection site pain, fatigue, and headache are common, though typically mild and short-lived.
In practice, protein vaccines are particularly suited for specific populations, such as individuals with mRNA contraindications or those hesitant about genetic-based technologies. For example, the Novavax vaccine has been approved for adults aged 18 and older, offering an alternative for those who cannot or prefer not to receive mRNA vaccines. When considering protein vaccines, it’s essential to weigh their benefits—such as established safety and ease of storage—against their drawbacks, like slower production timelines. This balanced perspective ensures informed decision-making in vaccine selection.
Concentra's Hepatitis B Vaccine Cost: What to Expect
You may want to see also
Explore related products






![]()
Storage Requirements: mRNA vaccines need ultra-cold storage; protein vaccines are more stable at standard refrigeration
One of the most significant logistical challenges in vaccine distribution is the storage requirement, which varies dramatically between mRNA and protein vaccines. mRNA vaccines, such as Pfizer-BioNTech and Moderna, require ultra-cold storage temperatures, typically between -60°C and -80°C (-76°F to -112°F), to maintain their stability and efficacy. This is because mRNA molecules are fragile and can degrade quickly at higher temperatures. In contrast, protein vaccines, like Novavax, are more robust and can be stored at standard refrigeration temperatures of 2°C to 8°C (36°F to 46°F), similar to many traditional vaccines. This difference has profound implications for global vaccine accessibility, particularly in regions with limited infrastructure.
Consider the practical implications for healthcare providers and distributors. mRNA vaccines often require specialized freezers and meticulous handling to ensure they remain viable from manufacturing to administration. For instance, Pfizer’s vaccine must be used within 5 days once stored at standard refrigeration after being thawed from ultra-cold conditions. Protein vaccines, on the other hand, can be stored in standard refrigerators for months, simplifying the supply chain and reducing the risk of spoilage. This stability makes protein vaccines more feasible for rural or low-resource settings, where ultra-cold storage is impractical or cost-prohibitive.
From a persuasive standpoint, the storage requirements of mRNA vaccines highlight both their innovation and their limitations. While mRNA technology represents a groundbreaking advancement in vaccine development, its logistical demands underscore the need for complementary solutions like protein vaccines. For example, Novavax’s protein-based vaccine, which uses recombinant nanoparticle technology, offers a more logistically friendly alternative without compromising efficacy. This duality—innovation versus practicality—is a critical consideration for policymakers aiming to balance cutting-edge science with equitable distribution.
A comparative analysis reveals the trade-offs between these vaccine types. mRNA vaccines, despite their storage challenges, offer rapid scalability and adaptability, as demonstrated during the COVID-19 pandemic. Protein vaccines, while easier to store, rely on more traditional manufacturing processes that may take longer to scale up. However, their stability at standard refrigeration temperatures makes them a more reliable option for sustained immunization campaigns, particularly in developing countries. For instance, a protein-based vaccine could be stored in a rural clinic’s refrigerator for months, ensuring consistent availability for patients of all age categories, from children to the elderly.
In conclusion, the storage requirements of mRNA and protein vaccines are not just technical details but pivotal factors shaping their global impact. While mRNA vaccines push the boundaries of scientific innovation, protein vaccines offer a practical, stable solution for widespread distribution. Understanding these differences empowers healthcare systems to make informed decisions, ensuring vaccines reach those who need them most, regardless of geographic or infrastructural barriers.
Vaccines Save Lives: Simplifying the Science for Skeptics
You may want to see also
Explore related products






![]()
Immune Response: mRNA elicits broader immune reactions; protein vaccines focus on specific antigens
The immune system's response to a vaccine is a delicate dance, and the choreography differs significantly between mRNA and protein-based vaccines. mRNA vaccines, such as the Pfizer-BioNTech and Moderna COVID-19 vaccines, introduce a novel approach by delivering genetic instructions to our cells, prompting them to produce a specific viral protein, often the spike protein. This process mimics a natural infection, triggering a robust immune reaction. In contrast, protein vaccines, like the Novavax COVID-19 vaccine, directly inject a harmless piece of the virus, typically the same spike protein, into the body.
The Breadth of Immune Activation: mRNA vaccines excel in eliciting a broad immune response. Once the mRNA enters our cells, it instructs them to manufacture the viral protein, which then gets displayed on the cell surface. This presentation activates multiple arms of the immune system. It stimulates the production of antibodies, particularly neutralizing antibodies that can prevent the virus from entering cells. Simultaneously, it engages T cells, including helper T cells that coordinate the immune response and killer T cells that eliminate infected cells. This comprehensive activation is akin to a full-scale military operation, targeting the invader from multiple angles.
Protein vaccines, on the other hand, take a more precision-focused approach. They introduce a specific viral protein, often in a highly purified form, directly into the body. This protein is typically accompanied by adjuvants, substances that enhance the immune response. The immune system recognizes the foreign protein, prompting the production of antibodies specifically tailored to that antigen. While this response is potent, it is more akin to a sniper's precision shot, targeting a single aspect of the virus. For instance, the Novavax vaccine uses a recombinant nanoparticle technology to display the spike protein, inducing a strong antibody response against this critical viral component.
Practical Implications and Considerations: The choice between these vaccine types has practical implications, especially for different populations. mRNA vaccines, with their broader immune activation, may be particularly beneficial for individuals with compromised immune systems, as they stimulate multiple immune pathways. However, this broad response can also lead to more systemic side effects, such as fever and fatigue, which are generally mild and short-lived. Protein vaccines, with their focused approach, might be preferred for those who have experienced severe reactions to other vaccine types or for specific age groups. For example, some protein-based vaccines are approved for use in adolescents and younger children, offering a targeted immune boost without the potential side effects of a broader response.
In the context of COVID-19 vaccination, the mRNA vaccines have been widely used for primary series and boosters, providing excellent protection against severe disease. Protein vaccines, with their unique advantages, offer an alternative for those who may not be suitable candidates for mRNA technology. This diversity in vaccine types ensures a more inclusive approach to immunization, catering to various immune profiles and preferences. Understanding these differences empowers individuals to make informed decisions about their healthcare, especially in an era where vaccine options are expanding.
Breeding Viruses for Vaccines: The Science Behind Lab Cultivation
You may want to see also
Explore related products






![]()
Development Speed: mRNA vaccines are faster to produce; protein vaccines require more complex manufacturing
The speed at which a vaccine can be developed and manufactured is a critical factor in responding to emerging infectious diseases. mRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna for COVID-19, have a distinct advantage in this area. Once the genetic sequence of a pathogen is known, mRNA vaccines can be designed and ready for testing within weeks. This rapid development timeline is due to the modular nature of mRNA technology, where the same production process can be adapted to target different diseases simply by changing the mRNA sequence. For instance, the COVID-19 mRNA vaccines were developed and authorized for emergency use within a year of the virus’s genetic sequence being published, a feat unprecedented in vaccine history.
In contrast, protein vaccines, like Novavax’s COVID-19 vaccine, require a more intricate manufacturing process. These vaccines use a specific protein from the pathogen, often the spike protein, which must be produced in large quantities, purified, and sometimes combined with adjuvants to enhance the immune response. This process involves cultivating cells in bioreactors, extracting the protein, and ensuring its stability—steps that are time-consuming and resource-intensive. For example, Novavax’s vaccine took approximately 18 months to reach authorization, partly due to these manufacturing complexities. While protein vaccines have a proven track record (e.g., the HPV and hepatitis B vaccines), their production timeline is inherently longer than that of mRNA vaccines.
From a practical standpoint, the faster development of mRNA vaccines offers a strategic advantage during pandemics or outbreaks. For instance, if a new variant of a virus emerges, mRNA vaccines can be quickly updated to match the variant’s genetic sequence. This agility was demonstrated during the Omicron wave, when Pfizer and Moderna began developing variant-specific boosters within weeks. Protein vaccines, however, would require additional time to re-engineer and scale up production, potentially delaying their availability. This difference in speed underscores the role of mRNA vaccines as a first line of defense in rapidly evolving public health crises.
Despite their slower development, protein vaccines have unique strengths that make them valuable in certain contexts. Their reliance on well-established manufacturing techniques and the stability of protein-based formulations can make them more accessible in regions with limited cold-chain infrastructure. For example, Novavax’s vaccine can be stored at standard refrigerator temperatures (2°C to 8°C), whereas mRNA vaccines require ultra-cold storage (-70°C for Pfizer’s vaccine, though later formulations allowed for -20°C). This makes protein vaccines a practical choice for low-resource settings or areas with unreliable electricity. Thus, while mRNA vaccines excel in speed, protein vaccines offer durability and logistical advantages that complement their slower production timeline.
In summary, the development speed of mRNA vaccines positions them as a rapid-response tool in the fight against infectious diseases, while protein vaccines, though slower to produce, provide a reliable and logistically feasible alternative. Understanding these differences allows public health officials to strategically deploy vaccines based on the specific needs of a situation—whether prioritizing speed during an outbreak or ensuring accessibility in resource-constrained regions. Both technologies have their place in the vaccine landscape, each addressing unique challenges in global health.
Vaccines for Children Program: Benefits, Eligibility, and Services Offered
You may want to see also
Frequently asked questions
mRNA vaccines deliver genetic instructions (mRNA) to cells to produce a specific protein (antigen), triggering an immune response. Protein vaccines, on the other hand, directly deliver the pre-made antigen protein to the immune system, bypassing the need for cells to produce it.
Protein vaccines have been used longer in humans, with examples like the hepatitis B and HPV vaccines. mRNA vaccines, such as the Pfizer-BioNTech and Moderna COVID-19 vaccines, are newer and represent a more recent advancement in vaccine technology.
Effectiveness depends on the specific disease and vaccine design. mRNA vaccines often elicit strong immune responses due to their ability to mimic viral infection, but protein vaccines can also be highly effective, especially when combined with adjuvants to boost immunity. Both types have proven successful in preventing diseases.