Vaccines and antibodies are both crucial components of the immune system, but they serve distinct roles in protecting the body against diseases. A vaccine is a biological preparation that stimulates the immune system to recognize and combat specific pathogens, such as viruses or bacteria, by introducing a harmless form of the pathogen or its components. This process triggers the production of memory cells, enabling the body to mount a rapid and effective response if exposed to the actual pathogen in the future. In contrast, antibodies are proteins produced by the immune system in response to the presence of foreign substances, known as antigens. They act as a direct defense mechanism by binding to and neutralizing pathogens, preventing them from causing infection. While vaccines proactively train the immune system to respond to future threats, antibodies are the immediate soldiers deployed to fight off active infections. Understanding the difference between these two is essential for grasping how the body defends itself against diseases.
| Characteristics | Values |
|---|---|
| Definition | Vaccine: A biological preparation that provides active acquired immunity to a particular infectious disease. Antibody: A protein produced by the immune system to neutralize or destroy pathogens like viruses or bacteria. |
| Purpose | Vaccine: Prevents infection by training the immune system to recognize and fight a pathogen. Antibody: Directly neutralizes or destroys pathogens after infection or exposure. |
| Administration | Vaccine: Typically administered via injection, orally, or nasally before exposure to a pathogen. Antibody: Administered via injection (e.g., monoclonal antibodies) after exposure or infection. |
| Immunity Type | Vaccine: Induces active immunity, where the body produces its own immune response. Antibody: Provides passive immunity, as the antibodies are externally supplied. |
| Duration of Protection | Vaccine: Long-term protection, often years, with potential need for boosters. Antibody: Short-term protection, typically weeks to months. |
| Mechanism | Vaccine: Stimulates the immune system to produce memory cells and antibodies. Antibody: Directly binds to and neutralizes pathogens without involving the immune system's memory. |
| Examples | Vaccine: COVID-19 vaccines (Pfizer, Moderna), flu vaccine, MMR vaccine. Antibody: Monoclonal antibodies (e.g., Casirivimab/Imdevimab for COVID-19), convalescent plasma. |
| Development Time | Vaccine: Typically takes years to develop and test. Antibody: Can be developed more quickly, especially monoclonal antibodies. |
| Side Effects | Vaccine: Mild to moderate side effects (e.g., soreness, fever). Antibody: Potential allergic reactions or infusion-related side effects. |
| Use in Treatment | Vaccine: Primarily used for prevention, not treatment. Antibody: Used for both prevention (e.g., post-exposure prophylaxis) and treatment of active infections. |
| Cost | Vaccine: Generally more cost-effective for large-scale prevention. Antibody: Often more expensive, especially for monoclonal antibody treatments. |
Explore related products






What You'll Learn
- Vaccines vs. Antibodies: Purpose - Vaccines prevent; antibodies fight existing infections, both crucial for immune defense
- How Vaccines Work - Stimulate immune system to produce antibodies against specific pathogens?
- How Antibodies Work - Proteins that tag or neutralize pathogens for immune system destruction?
- Active vs. Passive Immunity - Vaccines provide active immunity; antibodies offer passive, short-term protection
- Sources of Antibodies - Naturally produced or administered via treatments like monoclonal antibodies
![]()
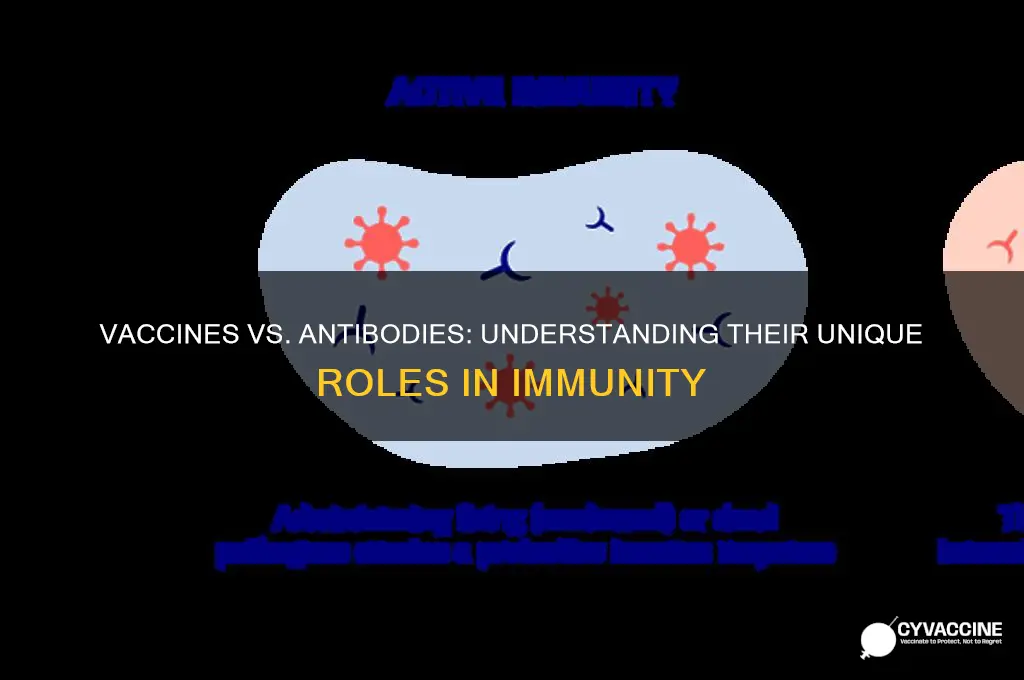
Vaccines vs. Antibodies: Purpose - Vaccines prevent; antibodies fight existing infections, both crucial for immune defense
Vaccines and antibodies are both cornerstones of immune defense, yet they serve distinct roles in safeguarding health. Vaccines act as proactive guardians, priming the immune system to recognize and neutralize pathogens before they cause illness. For instance, the COVID-19 mRNA vaccines, administered in two doses spaced 3–4 weeks apart, teach the body to produce spike proteins, triggering an immune response that prevents severe disease. This preventive approach is particularly vital for vulnerable populations, such as the elderly or immunocompromised, who may face higher risks from infections.
In contrast, antibodies are the immune system’s rapid response team, deployed to combat existing infections. These Y-shaped proteins bind to pathogens, neutralizing them or marking them for destruction by other immune cells. Monoclonal antibody treatments, like those used for COVID-19, provide immediate protection by delivering lab-created antibodies directly into the bloodstream. Unlike vaccines, which require weeks to build immunity, antibody treatments offer instant defense but are short-lived, typically effective for only a few weeks. This makes them a complementary tool, not a replacement for vaccination.
The interplay between vaccines and antibodies highlights their shared yet unique importance. Vaccines reduce the likelihood of infection, while antibodies mitigate damage when infections occur. For example, a child vaccinated against measles develops memory cells that swiftly produce antibodies upon exposure, preventing the virus from spreading. Conversely, an unvaccinated child relies solely on their innate immune response, which may be slower and less effective, increasing the risk of complications. This underscores why both prevention and treatment strategies are essential for public health.
Practical considerations further distinguish their use. Vaccines are typically administered via injection or nasal spray, with schedules tailored to age and health status—infants receive their first doses at 2 months, while adults may need boosters every 5–10 years. Antibody treatments, often given intravenously, are reserved for high-risk individuals or those with active infections. For instance, a 65-year-old with COVID-19 symptoms might receive a monoclonal antibody infusion within 10 days of symptom onset to prevent hospitalization. Understanding these differences empowers individuals to make informed decisions about their health.
Ultimately, vaccines and antibodies are not rivals but allies in the fight against disease. Vaccines fortify the immune system’s memory, while antibodies provide immediate relief during active infections. Together, they form a comprehensive defense strategy, illustrating the elegance of the immune system’s dual approach to protection. Whether through a flu shot or an antibody infusion, both tools are indispensable in maintaining individual and collective health.
Hepatitis Vaccine: Help or Hindrance for Existing Infections?
You may want to see also
Explore related products


$109 $119.99




![]()
How Vaccines Work - Stimulate immune system to produce antibodies against specific pathogens
Vaccines are not antibodies; they are the architects that train your immune system to recognize and combat specific pathogens. When you receive a vaccine, it introduces a harmless piece of a virus or bacterium, or a weakened/inactivated form of the pathogen, into your body. This triggers your immune system to produce antibodies—proteins designed to neutralize the invader. For example, the Pfizer-BioNTech COVID-19 vaccine delivers mRNA instructions to your cells to produce a harmless spike protein found on the SARS-CoV-2 virus, prompting your immune system to generate antibodies against it. This process mimics a natural infection but without the risk of severe illness.
The immune response to a vaccine unfolds in stages. First, antigen-presenting cells (APCs) engulf the vaccine’s components and present them to T cells, which activate B cells. These B cells then differentiate into plasma cells, the antibody factories of your immune system. A single B cell can produce up to 2,000 antibodies per second, ensuring a robust defense. Over time, some B cells become memory cells, which persist for years or even decades, ready to mount a rapid response if the actual pathogen is encountered. This is why vaccines often require multiple doses: the first primes the immune system, and subsequent doses boost antibody levels and memory cell formation. For instance, the HPV vaccine is administered in two or three doses over 6–12 months, depending on the recipient’s age.
While antibodies are the stars of this process, vaccines also stimulate cellular immunity, involving T cells that directly attack infected cells. This dual-pronged approach ensures a comprehensive defense. However, not all vaccines work the same way. Live-attenuated vaccines, like the MMR (measles, mumps, rubella) vaccine, use weakened pathogens to provoke a strong immune response, while subunit vaccines, like the hepatitis B vaccine, contain only specific pieces of the pathogen. Understanding these mechanisms helps explain why some vaccines provide lifelong immunity (e.g., yellow fever) while others require periodic boosters (e.g., tetanus).
Practical considerations are key to maximizing vaccine efficacy. Timing matters: spacing doses correctly allows the immune system to mature its response. For example, the influenza vaccine is reformulated annually to match circulating strains, and it’s best administered in early fall for optimal protection during peak flu season. Age also plays a role; infants receive vaccines in a staggered schedule to build immunity without overwhelming their developing immune systems. Adults, particularly those over 65, may need higher doses or adjuvants (substances that enhance immune response) due to age-related immune decline.
In summary, vaccines are not antibodies but the catalysts that drive antibody production and immune memory. By mimicking infection safely, they prepare your body to fight off real threats. Understanding this process empowers individuals to make informed decisions about vaccination, ensuring they receive the right vaccine at the right time and in the right dose. Whether it’s a childhood immunization or a travel vaccine, the principle remains the same: stimulate the immune system to protect against specific pathogens, one antibody at a time.
Essential Questions to Ask Before Administering Vaccines: A Comprehensive Guide
You may want to see also
Explore related products






![]()
How Antibodies Work - Proteins that tag or neutralize pathogens for immune system destruction
Antibodies, also known as immunoglobulins, are Y-shaped proteins produced by the immune system to identify and neutralize foreign objects like bacteria and viruses. These proteins are the body’s precision tools, designed to tag or directly neutralize pathogens, marking them for destruction by other immune cells. Unlike vaccines, which train the immune system to recognize and combat future threats, antibodies are the immediate responders, circulating in the bloodstream and lymphatic system, ready to bind to specific antigens on pathogens. This binding action either blocks the pathogen’s ability to infect cells or signals immune cells to engulf and destroy the invader. For instance, during a COVID-19 infection, antibodies target the virus’s spike protein, preventing it from entering human cells.
The process of antibody production begins when the immune system encounters a pathogen. B cells, a type of white blood cell, recognize the pathogen’s antigens and differentiate into plasma cells, which secrete antibodies tailored to that specific threat. This specificity is crucial—each antibody is uniquely shaped to fit a particular antigen, much like a key fits a lock. Monoclonal antibodies, a medical innovation, are lab-created proteins designed to mimic this natural process. They are used in treatments for conditions like cancer, autoimmune diseases, and infectious diseases, often administered intravenously in doses ranging from 500 mg to 1,000 mg, depending on the condition and patient age. For example, in COVID-19 treatment, monoclonal antibodies are given to high-risk individuals within 10 days of symptom onset to reduce disease severity.
Neutralization is one of the primary functions of antibodies. By binding to pathogens, they can block critical sites needed for infection, effectively disarming the threat. For instance, influenza antibodies attach to the virus’s hemagglutinin protein, preventing it from attaching to host cells. Tagging, another key function, involves coating the pathogen with antibodies, making it easier for phagocytic cells to identify and consume the invader. This dual action ensures that pathogens are either rendered harmless or swiftly eliminated. However, antibodies are not infallible; their effectiveness depends on the pathogen’s ability to mutate. For example, the flu vaccine is updated annually because the virus evolves, requiring new antibodies to match emerging strains.
Understanding how antibodies work highlights their role as both immediate defenders and long-term protectors. While vaccines stimulate the production of memory cells that can rapidly generate antibodies upon future exposure, antibodies themselves provide real-time protection. Passive antibody therapy, such as convalescent plasma or monoclonal antibody treatments, offers immediate immunity without the need for vaccination, making it particularly useful for immunocompromised individuals or during outbreaks. However, this protection is temporary, lasting weeks to months, whereas vaccine-induced immunity can persist for years. For practical application, individuals should consult healthcare providers to determine if antibody therapy is appropriate, especially for those over 65 or with underlying conditions, as they are at higher risk for severe infections.
In summary, antibodies are the immune system’s targeted weapons, working to neutralize or tag pathogens for destruction. Their specificity and dual functionality make them indispensable in fighting infections. While vaccines prepare the body for future threats, antibodies provide immediate defense, whether naturally produced or administered as treatment. Recognizing their distinct roles and limitations helps in making informed decisions about health interventions, ensuring both prevention and treatment strategies are optimized for maximum efficacy.
Vaccinated and Masked: Understanding the Ongoing Need for Face Coverings
You may want to see also
Explore related products





![]()
Active vs. Passive Immunity - Vaccines provide active immunity; antibodies offer passive, short-term protection
Vaccines and antibodies both combat disease, but they operate through fundamentally different mechanisms, conferring distinct types of immunity. Vaccines stimulate active immunity, a process where the body’s immune system is trained to recognize and fight a pathogen. For example, the mRNA COVID-19 vaccines (e.g., Pfizer-BioNTech, Moderna) deliver genetic instructions to cells, prompting them to produce a harmless piece of the virus’s spike protein. This triggers the immune system to generate antibodies and memory cells, offering long-term protection—often years—against the virus. In contrast, antibodies provide passive immunity, a short-term defense where pre-made antibodies are directly introduced into the body. For instance, monoclonal antibody treatments like casirivimab-imdevimab are administered to high-risk COVID-19 patients, offering immediate but temporary protection (typically weeks) without engaging the immune system’s memory.
Consider the analogy of a security system: vaccines are like training a guard dog to recognize and attack intruders, while antibodies are akin to hiring a temporary security guard who leaves after a few weeks. Active immunity is resource-intensive upfront—vaccines often require multiple doses (e.g., the COVID-19 series involves two primary doses and boosters) and time for the immune system to respond—but it builds lasting resilience. Passive immunity, however, is immediate but fleeting. For example, infants receive maternal antibodies via the placenta and breast milk, protecting them from infections like measles for the first 6–12 months of life until their own immune systems mature.
Practical applications highlight these differences. Vaccines are ideal for preventing diseases in healthy individuals, such as the annual flu shot or childhood immunizations like the MMR vaccine. Antibodies, however, are critical for vulnerable populations—immunocompromised patients, the elderly, or those exposed to a disease without prior immunity. For instance, rabies immunoglobulin is administered alongside the rabies vaccine to individuals bitten by a potentially rabid animal, providing instant protection while the vaccine induces active immunity.
A key caution: passive immunity’s short duration means it’s not a substitute for vaccination. Relying solely on antibody treatments leaves individuals unprotected once the antibodies degrade. Conversely, vaccines may not offer immediate protection—the COVID-19 mRNA vaccines take about two weeks to build significant immunity—making them less effective in emergency scenarios. Understanding these distinctions helps tailor interventions: vaccines for long-term prevention, antibodies for immediate, short-term defense.
In summary, the choice between vaccines and antibodies hinges on the context—prevention versus urgent protection, long-term versus short-term needs. Vaccines empower the body to defend itself, while antibodies provide a temporary shield. Both are vital tools in modern medicine, but their roles are complementary, not interchangeable. For optimal health, prioritize vaccination where possible, and reserve antibody treatments for specific, high-risk situations.
Where to Sign Up for the Vaccine: Official Website Guide
You may want to see also
Explore related products






![]()
Sources of Antibodies - Naturally produced or administered via treatments like monoclonal antibodies
Antibodies, the body's specialized proteins designed to neutralize pathogens, originate from two primary sources: natural production within the immune system or direct administration through medical treatments. When exposed to a pathogen, the body’s B cells activate, proliferate, and differentiate into plasma cells, which secrete antibodies tailored to the invading threat. This natural process, though robust, requires time—typically days to weeks—to mount an effective response. For instance, after a COVID-19 infection, detectable levels of IgG antibodies emerge around 10–14 days post-symptom onset, peaking at 2–3 weeks. In contrast, monoclonal antibody treatments, such as those used for severe COVID-19 cases (e.g., casirivimab/imdevimab), provide immediate, high-concentration antibodies via intravenous infusion, bypassing the need for the body to generate its own.
Administering monoclonal antibodies is a precise, targeted intervention, often reserved for high-risk individuals or those with compromised immune systems. For example, the FDA-approved dosage of sotrovimab for COVID-19 treatment is a single 500 mg intravenous infusion over 30 minutes, with monitoring for potential infusion-related reactions. This approach is particularly critical for patients over 65 or those with conditions like diabetes or heart disease, who face higher risks of severe illness. However, monoclonal antibodies are not a substitute for vaccination; they offer temporary protection (lasting weeks to months) and do not stimulate long-term immune memory.
Natural antibody production, while slower, confers lasting immunity through memory B cells, which can rapidly reactivate upon re-exposure to a pathogen. Vaccines exploit this mechanism by introducing a harmless antigen (e.g., mRNA, viral vector, or protein subunit) to trigger B cell activation without causing disease. For instance, the Pfizer-BioNTech COVID-19 vaccine induces a robust antibody response within 2–3 weeks of the second dose, with studies showing 95% efficacy in preventing symptomatic infection. Booster doses further enhance antibody titers, addressing waning immunity over time.
A key distinction lies in the duration and scope of protection. Naturally produced antibodies from infection may wane after 6–12 months, depending on the pathogen, while vaccine-induced immunity often lasts longer due to the controlled, optimized antigen presentation. Monoclonal antibodies, however, are short-lived and do not confer memory immunity, making them a reactive rather than preventive tool. For example, while monoclonal antibodies reduce hospitalization risk in early-stage COVID-19 by 70–85%, their protective window is limited to the treatment period.
In practice, combining these sources strategically maximizes protection. Vaccination remains the cornerstone of preventive care, while monoclonal antibodies serve as a critical therapeutic option for vulnerable populations. For instance, a 70-year-old with leukemia, ineligible for vaccination due to immunosuppression, might receive monoclonal antibodies prophylactically during a community outbreak. Conversely, a healthy 30-year-old should prioritize vaccination, relying on natural immunity for future exposures. Understanding these sources empowers individuals and healthcare providers to tailor interventions effectively, balancing prevention and treatment in the fight against infectious diseases.
Vaccines: Stopping Viruses in Their Tracks?
You may want to see also
Frequently asked questions
A vaccine is a biological preparation that provides active, acquired immunity to a particular infectious disease. It typically contains a weakened or inactivated form of the disease-causing pathogen (such as a virus or bacterium) or parts of it, which stimulates the immune system to recognize and fight the pathogen without causing the disease.
An antibody, also known as an immunoglobulin, is a protein produced by the immune system in response to the presence of a foreign substance, such as a virus or bacterium. Antibodies help the immune system identify and neutralize pathogens by binding to specific antigens on their surfaces, marking them for destruction by other immune cells.
A vaccine works proactively by training the immune system to recognize and combat a pathogen before an infection occurs, providing long-term immunity. Antibodies, on the other hand, are part of the immune system’s response to an existing infection or exposure, either naturally produced by the body or administered as a treatment (e.g., monoclonal antibodies) to help fight off the pathogen immediately.