Developing a vaccine is a complex and multifaceted process that involves rigorous scientific research, clinical trials, regulatory approvals, and manufacturing scalability. On average, it takes about 10 to 15 years to bring a vaccine from the initial research phase to market availability. However, this timeline can vary significantly depending on factors such as the type of pathogen, the urgency of the need, funding availability, and technological advancements. For instance, the COVID-19 pandemic accelerated vaccine development to an unprecedented 12-18 months due to global collaboration, emergency funding, and streamlined regulatory processes. Despite such exceptions, the traditional timeline underscores the challenges of ensuring safety, efficacy, and mass production, highlighting why vaccine development remains a lengthy and resource-intensive endeavor.
| Characteristics | Values |
|---|---|
| Average Time to Develop a Vaccine | Historically, 10-15 years, but accelerated to 1-2 years during COVID-19 |
| Preclinical Stage | 3-6 years (lab research and animal testing) |
| Clinical Trials (Phase 1-3) | 6-8 years (human testing for safety, efficacy, and dosage) |
| Regulatory Review and Approval | 6 months to 2 years |
| Manufacturing and Distribution | 6-12 months |
| Fastest Vaccine Development | Pfizer-BioNTech COVID-19 vaccine (11 months from development to approval) |
| Key Factors Affecting Timeline | Funding, technology, regulatory processes, and disease complexity |
| Recent Technological Advances | mRNA and viral vector platforms significantly reduced development time |
| Emergency Use Authorization (EUA) | Allows expedited approval during public health emergencies |
Explore related products



$8.41 $30



What You'll Learn
![]()
Historical vaccine development timelines
Vaccine development has historically been a marathon, not a sprint, with timelines stretching from a few years to several decades. The smallpox vaccine, developed in 1796 by Edward Jenner, stands as one of the earliest successes, taking roughly 20 years from initial observation to widespread use. This timeline, however, was atypical for its era, as most vaccines prior to the 20th century relied on trial-and-error methods, often with limited scientific understanding. For instance, the rabies vaccine, introduced by Louis Pasteur in 1885, required over a decade of experimentation, including direct human testing, which would be ethically unthinkable today. These early efforts highlight the painstaking nature of vaccine development before modern scientific tools and regulatory frameworks existed.
The 20th century brought significant advancements, reducing development times but still requiring considerable effort. The polio vaccine, developed by Jonas Salk in 1955, took nearly 20 years from initial research to approval, involving large-scale clinical trials and public health campaigns. In contrast, the measles vaccine, introduced in 1963, took just over a decade, benefiting from improved virology techniques and a clearer understanding of the virus. These examples illustrate how scientific progress and infrastructure began to compress timelines, though they remained lengthy by modern standards. Each vaccine also required multiple doses—for polio, the inactivated vaccine (IPV) typically involves 3–4 doses, while the measles vaccine is often administered as part of the MMR (measles, mumps, rubella) combination, with 2 doses recommended for full immunity.
The late 20th and early 21st centuries saw further acceleration, driven by technological breakthroughs and global collaboration. The mumps vaccine, developed in 1967, took less than a decade, while the hepatitis B vaccine, approved in 1981, benefited from recombinant DNA technology, reducing development time to around 15 years. However, exceptions like the human papillomavirus (HPV) vaccine, approved in 2006 after nearly 20 years of research, remind us that complexity and safety concerns can still extend timelines. The HPV vaccine, for instance, required extensive testing across diverse age groups, with recommendations now targeting adolescents aged 11–12 for optimal efficacy, often involving a 2- or 3-dose regimen depending on age at initial vaccination.
The COVID-19 pandemic marked an unprecedented shift, with vaccines developed in under a year, a feat made possible by decades of research on related coronaviruses, massive funding, and global cooperation. However, this timeline is an outlier, not a new norm. Historically, vaccines like the Ebola vaccine, approved in 2019 after nearly 5 years of accelerated development, demonstrate that even in emergencies, safety and efficacy remain non-negotiable. Practical takeaways from history include the importance of sustained investment in research, flexible regulatory processes, and public trust. For individuals, understanding vaccine schedules—such as the 2-dose regimen for COVID-19 vaccines or the annual flu shot—ensures maximum protection. History teaches us that while timelines can vary, the foundation of successful vaccine development lies in science, patience, and preparedness.
MMR Vaccine Dosage: Understanding the Standard Oz Measurement
You may want to see also
Explore related products






![]()
Factors influencing vaccine development speed
Developing a vaccine typically takes 10 to 15 years, but the COVID-19 pandemic slashed this timeline to under one year. This unprecedented speed wasn’t magic—it was the result of specific factors aligning to accelerate the process. Understanding these factors reveals how vaccine development timelines can be shortened without compromising safety or efficacy.
Funding and Resource Allocation: The Fuel for Speed
Massive financial investment acts as a catalyst for rapid vaccine development. During the COVID-19 pandemic, governments and private sectors poured billions into research, manufacturing, and distribution. For instance, Operation Warp Speed in the U.S. allocated $18 billion, enabling parallel testing of multiple vaccine candidates. Without such funding, traditional sequential testing would have added years to the timeline. To replicate this speed, stakeholders must prioritize upfront investment, ensuring labs have access to cutting-edge technology, large-scale clinical trial sites, and manufacturing facilities ready to produce doses at scale.
Regulatory Flexibility: Balancing Speed and Safety
Regulatory agencies like the FDA played a pivotal role in expediting COVID-19 vaccines by streamlining processes without lowering safety standards. Rolling reviews allowed data from clinical trials to be assessed in real-time, shaving months off approval timelines. Emergency Use Authorizations (EUAs) further accelerated access. However, this approach requires meticulous monitoring of side effects post-approval. For future pandemics, maintaining this balance between speed and safety will hinge on transparent communication and robust post-market surveillance systems.
Scientific Advancements: Building on Past Innovations
The rapid development of mRNA vaccines (e.g., Pfizer and Moderna) was possible because the technology had been in development for decades. Researchers had already established the platform’s safety and efficacy for diseases like Zika and influenza. COVID-19 merely provided the urgency to scale it up. Similarly, platforms like viral vectors (used in Johnson & Johnson’s vaccine) were adapted from existing research. Investing in foundational science today—such as next-generation adjuvants or self-amplifying RNA—could unlock even faster responses tomorrow.
Global Collaboration: A Multiplied Effort
The pandemic fostered unprecedented collaboration among scientists, governments, and industries worldwide. Data sharing, open-access research, and cross-border clinical trials eliminated redundancies and accelerated problem-solving. For example, the Oxford-AstraZeneca vaccine was developed through a partnership between a university and a pharmaceutical giant, with manufacturing agreements spanning multiple continents. Sustaining this collaborative spirit requires dismantling intellectual property barriers and fostering trust among nations. Without such unity, future vaccine development risks reverting to slower, siloed processes.
Public Health Urgency: A Double-Edged Sword
The sheer scale of COVID-19’s impact created an environment where rapid vaccine development was not just desirable but essential. This urgency mobilized resources and streamlined decision-making. However, it also heightened the risk of public skepticism and misinformation. Ensuring public trust requires clear messaging about vaccine safety and efficacy, coupled with transparent reporting of trial results. For instance, explaining that mRNA vaccines do not alter DNA or that rare side effects (e.g., myocarditis in young males, occurring at rates of 1 in 10,000) are closely monitored can alleviate concerns.
By dissecting these factors, it becomes clear that rapid vaccine development is achievable but requires a delicate interplay of resources, innovation, collaboration, and trust. Each factor serves as a lever that, when pulled effectively, can shorten timelines without sacrificing safety. The challenge lies in sustaining these conditions beyond crises, ensuring humanity remains prepared for the next threat.
Hepatitis B Vaccine: How Does It Work?
You may want to see also
Explore related products






![]()
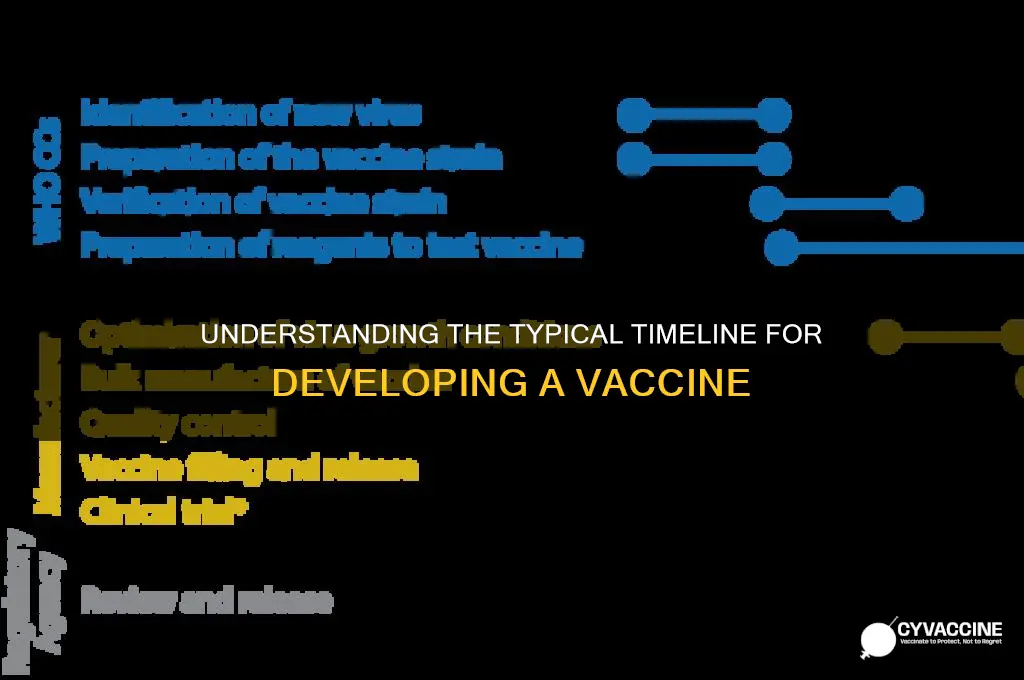
Role of technology in accelerating development
Historically, vaccine development has been a marathon, not a sprint, often taking 10 to 15 years from initial research to market availability. The COVID-19 pandemic, however, shattered this timeline, with several vaccines authorized for emergency use within a year. This unprecedented speed wasn't magic; it was technology.
Consider the mRNA platform, a cornerstone of COVID-19 vaccines like Pfizer-BioNTech and Moderna. Unlike traditional methods that rely on weakened viruses or viral proteins, mRNA vaccines deliver genetic instructions, allowing our cells to produce a harmless piece of the virus, triggering an immune response. This modular approach, akin to swapping out software code, enabled rapid adaptation to the SARS-CoV-2 genome sequence, shared publicly in January 2020.
Technology also streamlined clinical trials. Digital platforms facilitated remote monitoring of participants, while advanced analytics accelerated data analysis. For instance, adaptive trial designs allowed researchers to modify dosage levels (e.g., 30 µg for Pfizer’s vaccine) or group sizes mid-study based on real-time data, optimizing efficiency without compromising safety.
Manufacturing, once a bottleneck, benefited from innovations like single-use bioreactors and automated fill-finish systems. These reduced cross-contamination risks and increased production scalability, ensuring millions of doses could be manufactured concurrently. For context, Pfizer’s Kalamazoo facility produced up to 1 billion doses in 2021, a feat unimaginable without such advancements.
The takeaway? Technology doesn’t just accelerate vaccine development; it redefines its boundaries. From design to delivery, each stage now leverages tools that were science fiction a decade ago. While challenges like equitable distribution persist, the role of technology in compressing timelines from decades to months is undeniable—a blueprint for future pandemics and beyond.
Essential Puppy Vaccinations: What Your 15-Week-Old Pup Needs Now
You may want to see also
Explore related products






![]()
Regulatory approval process duration
The regulatory approval process is a critical phase in vaccine development, often spanning 5 to 10 years under normal circumstances. This timeline, however, is not set in stone. For instance, the COVID-19 vaccines received emergency use authorization in under a year, showcasing how urgency and global collaboration can accelerate this stage. Such exceptions highlight the flexibility of regulatory frameworks when public health demands it.
Consider the steps involved: preclinical testing, three phases of clinical trials, and rigorous review by agencies like the FDA or EMA. Each phase is designed to ensure safety and efficacy, but it’s the regulatory review that often becomes the bottleneck. Agencies scrutinize data on dosage levels (e.g., 30 µg of mRNA in Pfizer’s vaccine), side effects, and long-term outcomes. For pediatric vaccines, additional trials are required to adjust dosages for age categories, such as half-doses for children aged 5–11, further extending the timeline.
A persuasive argument for streamlining this process lies in its inefficiencies. While safety cannot be compromised, redundant paperwork and siloed global reviews delay approvals unnecessarily. Harmonizing regulatory standards across countries could shave years off this phase. For example, mutual recognition agreements between the FDA and EMA could allow simultaneous reviews, reducing duplication of effort.
Practically, developers can expedite approval by engaging regulators early. Pre-submission meetings clarify expectations, while rolling reviews—where data is assessed as it becomes available—can cut months off the timeline. Manufacturers should also prepare for post-approval monitoring, such as tracking adverse events in real-world settings, to maintain public trust and regulatory compliance.
In conclusion, while the regulatory approval process is inherently lengthy, it is neither inflexible nor immutable. Strategic planning, global cooperation, and adaptive frameworks can significantly reduce its duration without sacrificing safety. The COVID-19 pandemic proved that when stakes are high, this phase can be expedited—a lesson worth applying to future vaccine development.
Vaccines and Abortion: The Fetal Cell Myth
You may want to see also
Explore related products






![]()
Funding and resource impact on timelines
The average time to develop a vaccine typically spans 10 to 15 years, but funding and resource allocation can dramatically compress or extend this timeline. During the COVID-19 pandemic, unprecedented financial investment and global collaboration slashed development to under one year, proving that money and coordination are critical accelerants. Conversely, vaccines for diseases primarily affecting low-income regions, like malaria, have languished for decades due to insufficient funding. This disparity highlights how resource availability dictates speed, innovation, and ultimately, public health outcomes.
Consider the logistical hurdles: clinical trials for a vaccine require thousands of participants, specialized equipment, and stringent safety protocols. A well-funded project can run multiple trial phases concurrently, hire top researchers, and secure priority access to manufacturing facilities. For instance, Operation Warp Speed allocated $18 billion to COVID-19 vaccine efforts, enabling companies like Pfizer and Moderna to produce 95% effective mRNA vaccines in record time. Without such funding, these trials would have staggered over years, not months. Practical tip: Governments and organizations must prioritize early-stage funding to avoid bottlenecks in research and production.
However, funding alone isn’t enough; resource distribution matters equally. During the Ebola outbreak in 2014, limited infrastructure in affected African countries delayed vaccine deployment despite available funding. Cold chain requirements, transportation networks, and trained healthcare workers are essential for delivering doses effectively. For example, the Pfizer COVID-19 vaccine requires storage at -70°C, a challenge in regions lacking advanced refrigeration. Comparative analysis shows that regions with robust healthcare systems and pre-existing manufacturing capabilities can distribute vaccines 3–5 times faster than those without.
Persuasive argument: Investing in global health infrastructure isn’t just altruistic—it’s self-preserving. The longer a disease circulates in under-resourced regions, the higher the risk of mutations that render existing vaccines ineffective. For instance, the polio vaccine faced setbacks due to vaccine hesitancy and inadequate distribution in parts of Africa and Asia, allowing the virus to persist. By allocating resources equitably, we not only save lives but also prevent future pandemics. Step one: Establish regional manufacturing hubs in low-income countries. Step two: Train local healthcare workers to administer vaccines efficiently.
Descriptive example: Imagine a vaccine development pipeline as a highway. Funding acts as the number of lanes—more lanes mean faster progress. Resources, like fuel and vehicle maintenance, ensure the journey isn’t interrupted. During the H1N1 pandemic in 2009, the U.S. invested $1.5 billion in vaccine production, but delays occurred due to reliance on egg-based manufacturing, a slow and outdated method. In contrast, mRNA technology, backed by substantial funding, bypassed these limitations in 2020. Takeaway: Modernizing production methods and ensuring resource flexibility are as vital as financial investment in shortening timelines.
Booster Shots for J&J Vaccine: What You Need to Know
You may want to see also
Frequently asked questions
Traditionally, vaccine development takes 10 to 15 years, including research, clinical trials, and regulatory approval.
Yes, with accelerated processes, funding, and global collaboration, vaccine development can be shortened to 1 to 2 years, as seen with COVID-19 vaccines.
Clinical trials (Phase 1, 2, and 3) and regulatory review are the most time-consuming stages, often taking several years.
It involves rigorous testing for safety, efficacy, and manufacturing quality, ensuring the vaccine is both effective and safe for widespread use.