Childhood vaccines are a cornerstone of public health, preventing millions of illnesses and deaths annually. A critical aspect of their effectiveness is the percentage of time they successfully produce immunity. Most childhood vaccines, such as those for measles, mumps, rubella, and polio, confer immunity in 90-99% of recipients after the recommended series of doses. This high rate of protection not only safeguards vaccinated individuals but also contributes to herd immunity, reducing disease transmission in communities. However, factors like vaccine type, individual immune response, and adherence to vaccination schedules can influence immunity levels. Understanding these percentages is essential for addressing vaccine hesitancy and ensuring widespread protection against preventable diseases.
Explore related products






What You'll Learn
- Vaccine Efficacy Rates: Percentage of children achieving immunity post-vaccination for common childhood diseases
- Immunity Duration: How long vaccine-induced immunity typically lasts in children after full doses
- Factors Affecting Immunity: Role of age, health, and vaccine type in immunity success rates
- Herd Immunity Impact: How childhood vaccination rates contribute to community-wide disease protection
- Breakthrough Infections: Frequency of vaccine-preventable diseases occurring despite immunization in children
![]()
Vaccine Efficacy Rates: Percentage of children achieving immunity post-vaccination for common childhood diseases
Childhood vaccines are a cornerstone of public health, but their efficacy rates—the percentage of children who achieve immunity post-vaccination—vary depending on the disease and vaccine type. For instance, the measles, mumps, and rubella (MMR) vaccine is a standout performer, with two doses conferring immunity to measles in 97% of children, mumps in 88%, and rubella in over 95%. These high rates underscore the vaccine’s role in nearly eradicating measles in many regions. In contrast, the influenza vaccine’s efficacy fluctuates annually, typically ranging from 40% to 60% in children, due to the virus’s rapid mutation and the need for seasonal updates. Understanding these differences is crucial for parents and healthcare providers to set realistic expectations and emphasize the importance of timely vaccination.
Consider the varicella (chickenpox) vaccine, which demonstrates how efficacy can improve with additional doses. A single dose provides immunity in about 85% of children, but a second dose boosts this rate to over 98%. This two-dose regimen, recommended for children aged 12–15 months and 4–6 years, not only reduces the risk of chickenpox but also prevents severe complications like bacterial infections and pneumonia. Practical tip: ensure your child receives both doses on schedule, as spacing them 3 months apart can optimize immune response. This example highlights how vaccine design and administration protocols directly influence immunity outcomes.
The diphtheria, tetanus, and pertussis (DTaP) vaccine illustrates another dimension of efficacy: duration of immunity. While 80–90% of children achieve protection after the full five-dose series (starting at 2 months and ending at 4–6 years), immunity to pertussis wanes over time, with effectiveness dropping to 70% after 1 year and 40% after 3 years. This explains why breakthrough infections occur despite vaccination. To mitigate this, adolescents and adults are advised to receive booster shots (Tdap) to maintain immunity and reduce transmission, especially to vulnerable infants. This underscores the importance of lifelong vaccination strategies for sustained protection.
Efficacy rates also depend on factors beyond the vaccine itself, such as age, underlying health conditions, and geographic location. For example, the rotavirus vaccine, which prevents severe diarrhea in infants, has an efficacy of 90% in developed countries but drops to 50–60% in low-income regions with higher disease prevalence. This disparity highlights the interplay between vaccine biology and environmental factors. Parents in high-risk areas should prioritize early vaccination (starting at 6 weeks) and ensure the full series (2 or 3 doses, depending on the brand) is completed by 8 months. Such tailored approaches maximize individual and community-level immunity.
Finally, the human papillomavirus (HPV) vaccine exemplifies how high efficacy rates translate into long-term disease prevention. Administered in two doses to children aged 9–14 (or three doses for older teens), it provides nearly 100% protection against the HPV types responsible for most cervical cancers. This vaccine’s success lies in its ability to induce robust, long-lasting immune responses before potential exposure. Persuasive takeaway: by vaccinating preteens, parents can virtually eliminate their child’s risk of HPV-related cancers later in life. This proactive approach is a testament to the power of vaccination in shaping healthier futures.
Pharmacists: Skilled Vaccine Administrators?
You may want to see also
Explore related products


$27.74 $32.99




![]()
Immunity Duration: How long vaccine-induced immunity typically lasts in children after full doses
Childhood vaccines are designed to provide robust immunity, but the duration of this protection varies widely depending on the vaccine and the pathogen it targets. For instance, the measles, mumps, and rubella (MMR) vaccine typically confers lifelong immunity after two doses, administered at 12–15 months and 4–6 years. In contrast, the diphtheria, tetanus, and pertussis (DTaP) vaccine requires booster shots every 10 years to maintain immunity, as protection wanes over time. Understanding these differences is crucial for parents and healthcare providers to ensure children remain protected throughout their developmental years.
Consider the influenza vaccine, which presents a unique challenge due to the virus’s rapid mutation. Children aged 6 months and older need annual vaccination because the vaccine’s effectiveness lasts only about 6–12 months. This highlights the importance of timely, repeated doses to align with seasonal flu strains. Conversely, the hepatitis B vaccine, given in three doses starting at birth, provides immunity for at least 20 years, often a lifetime, without the need for boosters. These examples illustrate how vaccine design and pathogen behavior dictate immunity duration.
Age plays a critical role in how long vaccine-induced immunity lasts. Infants and young children, for example, may require additional doses of certain vaccines to build sufficient immunity. The Haemophilus influenzae type b (Hib) vaccine is administered in a series of 3–4 doses starting at 2 months, with immunity lasting into adulthood. Adolescents, on the other hand, may need booster shots for vaccines like Tdap (tetanus, diphtheria, and pertussis) around age 11–12 to reinforce waning immunity. Tailoring vaccination schedules to age-specific immune responses ensures optimal protection.
Practical tips can help parents and caregivers maximize the benefits of childhood vaccines. Keep a detailed record of vaccination dates and doses, as some vaccines require precise timing between doses to achieve full immunity. For example, the varicella (chickenpox) vaccine is given in two doses, with the second dose administered 3 months after the first. Stay informed about recommended booster shots, especially for vaccines like HPV (human papillomavirus), which requires a series of 2–3 doses for adolescents aged 11–14. Finally, consult healthcare providers regularly to address any concerns and ensure children are up to date on their immunizations.
In summary, vaccine-induced immunity in children is not one-size-fits-all. It depends on the vaccine, the pathogen, the child’s age, and the vaccination schedule. While some vaccines provide lifelong protection, others require boosters to sustain immunity. By understanding these nuances and following recommended guidelines, parents and healthcare providers can ensure children remain shielded from preventable diseases throughout their critical developmental years.
Vaccine Rules: DC's Proof-of-Vaccination Requirements
You may want to see also
Explore related products






![]()
Factors Affecting Immunity: Role of age, health, and vaccine type in immunity success rates
Childhood vaccines are a cornerstone of public health, but their effectiveness isn’t uniform. Immunity success rates vary widely, influenced by factors like age, underlying health, and vaccine type. For instance, the measles vaccine confers immunity in 93% of recipients after one dose and 97% after two, while the influenza vaccine’s efficacy fluctuates annually, ranging from 40% to 60% due to viral strain mismatches. Understanding these variables is critical for optimizing vaccine strategies and ensuring protection.
Age plays a pivotal role in vaccine-induced immunity. Infants, with immature immune systems, often require multiple doses to build robust immunity. For example, the diphtheria-tetanus-pertussis (DTaP) vaccine is administered in a series of five doses starting at 2 months, with each dose incrementally boosting immune response. Conversely, adolescents and adults may respond more vigorously to vaccines due to fully developed immune systems, but aging can reverse this advantage. In older adults, immune senescence reduces vaccine efficacy, as seen with the shingles vaccine, which is 97% effective in those over 50 but less so in older cohorts.
Underlying health conditions significantly impact immunity success rates. Immunocompromised individuals, such as those with HIV or undergoing chemotherapy, often mount weaker responses to vaccines. For instance, the pneumococcal vaccine’s efficacy drops to 50-70% in HIV-positive individuals compared to 60-80% in healthy adults. Chronic illnesses like diabetes or asthma can also impair immune responses, necessitating tailored vaccination schedules or adjuvanted formulations. Pregnant individuals, while generally responsive to vaccines like Tdap, may require specific timing to maximize maternal and fetal protection.
Vaccine type and formulation are equally critical determinants of immunity. Live-attenuated vaccines, such as MMR (measles, mumps, rubella), typically induce stronger, longer-lasting immunity but are contraindicated in immunocompromised individuals. Inactivated or subunit vaccines, like the hepatitis B vaccine, often require booster doses to maintain immunity. Adjuvants, such as aluminum salts in the HPV vaccine, enhance immune responses but can increase local reactions. mRNA vaccines, a recent innovation, have shown remarkable efficacy, with Pfizer’s COVID-19 vaccine achieving 95% protection in clinical trials, though real-world effectiveness varies with emerging variants.
Practical strategies can mitigate these factors and improve immunity outcomes. For age-related challenges, adhering to recommended vaccination schedules is essential. Health providers should screen for underlying conditions and adjust vaccine choices accordingly—for example, using high-dose influenza vaccines for older adults. Public health campaigns must emphasize the importance of boosters, particularly for vaccines with waning immunity like tetanus (requiring a booster every 10 years). Finally, ongoing research into personalized vaccine regimens and next-generation formulations promises to address current limitations, ensuring broader and more durable protection across diverse populations.
Can Dogs Be Vaccinated Against Poisonous Snake Bites? Exploring the Facts
You may want to see also
Explore related products





![]()
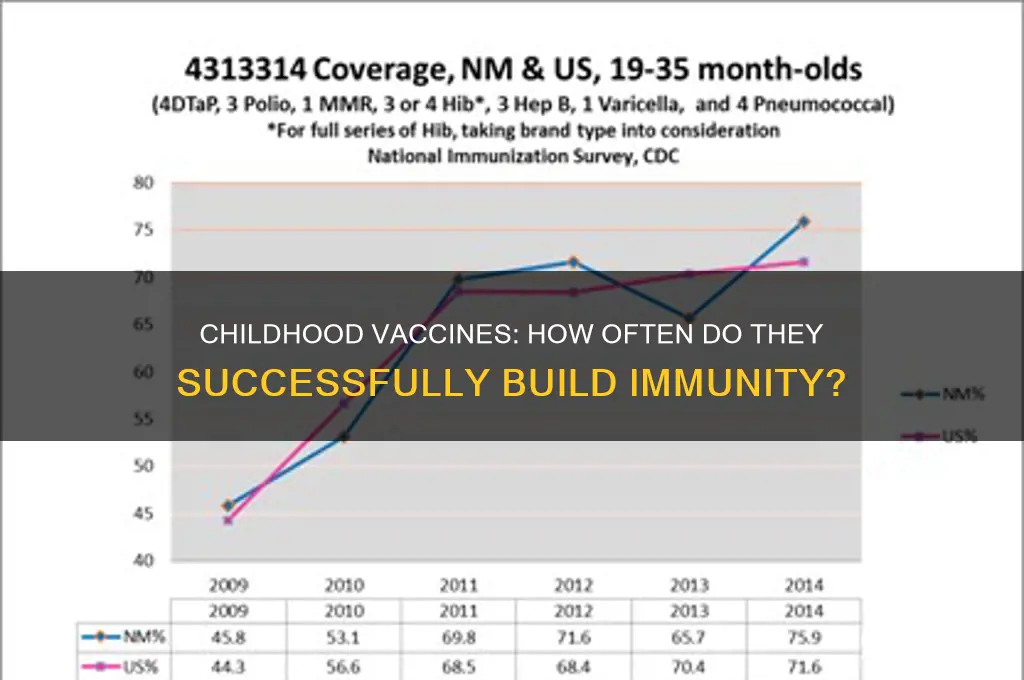
Herd Immunity Impact: How childhood vaccination rates contribute to community-wide disease protection
Childhood vaccines are remarkably effective, typically producing immunity in 85-95% of recipients after a complete series. This high success rate is critical for individual protection, but its true power lies in herd immunity—a community-wide shield against disease. When vaccination rates reach a certain threshold, usually 90-95% for highly contagious diseases like measles, the spread of pathogens is significantly hindered, protecting even those who cannot be vaccinated due to medical reasons. This collective defense mechanism is why childhood vaccination rates are not just personal health decisions but a cornerstone of public health.
Consider measles, a highly contagious virus with a basic reproduction number (R0) of 12-18, meaning one infected person can spread it to 12-18 others in an unvaccinated population. The measles vaccine, administered in two doses (first at 12-15 months, second at 4-6 years), achieves 97% immunity after the full series. When 95% of a community is vaccinated, the virus struggles to find susceptible hosts, effectively halting outbreaks. However, when vaccination rates drop below this threshold, as seen in recent anti-vaccine movements, outbreaks reemerge. For instance, the 2019 U.S. measles outbreak, with over 1,200 cases, was linked to communities with vaccination rates as low as 70%.
Achieving herd immunity requires strategic vaccination efforts, particularly for diseases like pertussis (whooping cough), where the vaccine’s efficacy wanes over time. The DTaP vaccine series (diphtheria, tetanus, pertussis), given at 2, 4, 6, and 15-18 months, followed by boosters at 4-6 years and 11-12 years, provides initial protection but diminishes after 3-5 years. This makes cocooning—vaccinating close contacts of infants too young for vaccination—essential. For example, pregnant women receiving the Tdap vaccine during each pregnancy passes antibodies to newborns, offering critical early protection until they can receive their first dose at 2 months.
Critics often question vaccine safety, but the benefits of herd immunity far outweigh rare risks. Adverse reactions are exceedingly rare: severe allergic reactions to the MMR vaccine occur in about 1 in a million doses. Compare this to the 1 in 500 risk of hospitalization from measles complications. Public health campaigns must emphasize these statistics while addressing misinformation. For instance, the debunked link between the MMR vaccine and autism has persisted despite overwhelming evidence to the contrary, highlighting the need for clear, science-based communication.
In practice, maintaining herd immunity requires vigilance. Schools and healthcare providers play a pivotal role by enforcing vaccination mandates and offering catch-up schedules for missed doses. Parents can contribute by adhering to the CDC’s recommended immunization schedule and staying informed about local disease trends. For example, during a mumps outbreak, ensuring adolescents receive the recommended two doses of the MMR vaccine (first at 12-15 months, second at 4-6 years) can curb transmission. Ultimately, herd immunity is a shared responsibility, where each vaccinated child strengthens the community’s defense, proving that the impact of childhood vaccination extends far beyond the individual.
Is the Polio Vaccine FDA-Approved? Facts and Safety Explained
You may want to see also
Explore related products






![]()
Breakthrough Infections: Frequency of vaccine-preventable diseases occurring despite immunization in children
Childhood vaccines are remarkably effective, typically conferring immunity in 85% to 99% of recipients, depending on the disease. For instance, two doses of the measles, mumps, and rubella (MMR) vaccine are 97% effective in preventing measles, while the diphtheria, tetanus, and pertussis (DTaP) vaccine achieves 80-90% efficacy against pertussis. However, even within these high success rates, a small percentage of vaccinated children remain susceptible to breakthrough infections—cases where a vaccine-preventable disease occurs despite immunization. Understanding the frequency and factors contributing to these events is critical for public health strategies and parental confidence in vaccination programs.
Breakthrough infections are not a sign of vaccine failure but rather a reflection of biological variability and vaccine limitations. For example, the influenza vaccine’s efficacy ranges from 40% to 60% annually due to viral mutations and individual immune responses. Similarly, while the chickenpox (varicella) vaccine is 98% effective in preventing severe disease, it may still allow mild breakthrough cases in 2-4% of vaccinated children. Age, underlying health conditions, and time since vaccination also play roles; immunity can wane over time, increasing susceptibility. For instance, tetanus and diphtheria immunity may decline 5-10 years after the last booster, necessitating timely follow-up doses.
To minimize breakthrough infections, adherence to recommended vaccine schedules is essential. The Centers for Disease Control and Prevention (CDC) advises completing the full series of doses for optimal protection. For example, the MMR vaccine requires two doses, with the first at 12-15 months and the second at 4-6 years. Delayed or skipped doses reduce efficacy, increasing breakthrough risk. Additionally, herd immunity plays a vital role; when vaccination rates drop below 90-95%, as seen in recent measles outbreaks, even fully vaccinated individuals face higher risk due to increased disease circulation.
Practical steps can further reduce breakthrough infection risk. Parents should ensure children receive all recommended vaccines on time, including boosters. For travel to areas with higher disease prevalence, consulting a healthcare provider for additional precautions is advisable. Monitoring for symptoms and prompt medical attention if a breakthrough infection is suspected can prevent complications. Finally, staying informed about vaccine updates, such as reformulated influenza vaccines or new COVID-19 variants, ensures ongoing protection. Breakthrough infections, while rare, underscore the importance of maintaining high vaccination rates and individual vigilance to safeguard children’s health.
Could a Vaccine Be the Solution to Lyme Disease?
You may want to see also
Frequently asked questions
Most childhood vaccines produce immunity in 85-99% of recipients, depending on the specific vaccine and individual factors.
Yes, some vaccines, like the influenza vaccine, may have lower efficacy rates (around 40-60%) due to the virus's frequent mutations, but most routine childhood vaccines have higher success rates.
Vaccine efficacy can vary due to factors like individual immune system differences, underlying health conditions, or improper vaccine storage/administration, making 100% immunity unattainable.