As of recent data, a significant portion of the U.S. population has received at least one dose of the COVID-19 vaccine, with vaccination rates varying by state and demographic group. According to the Centers for Disease Control and Prevention (CDC), approximately 68% of the total U.S. population has been fully vaccinated, while over 77% have received at least one dose. These figures reflect ongoing efforts to combat the pandemic, though disparities in access and hesitancy persist, particularly in certain regions and communities. Understanding these percentages is crucial for assessing the nation’s progress in achieving herd immunity and reducing the spread of the virus.
Explore related products






What You'll Learn
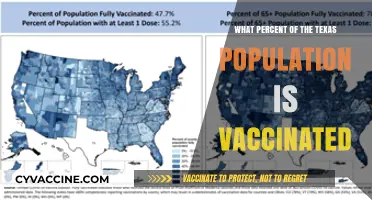
- Vaccination Rates by State: Compare vaccine distribution and uptake across different U.S. states
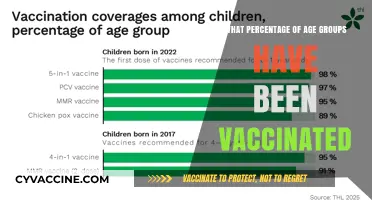
- Age Group Vaccination: Analyze vaccination percentages among various age demographics in the U.S
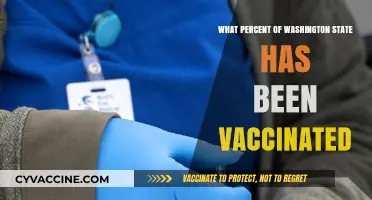
- Urban vs. Rural Areas: Examine vaccine coverage differences between urban and rural populations
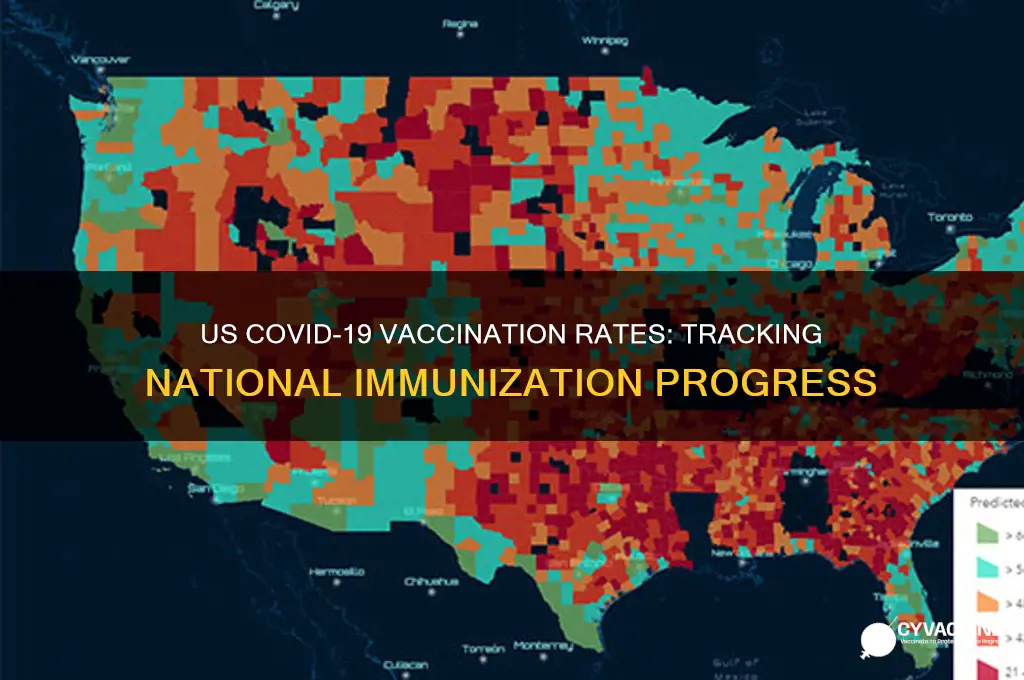
- Vaccine Hesitancy Trends: Explore factors contributing to vaccine hesitancy and its impact on percentages
- Booster Shot Uptake: Assess the percentage of the U.S. population receiving COVID-19 booster doses
![]()
Vaccination Rates by State: Compare vaccine distribution and uptake across different U.S. states
As of the latest data, vaccination rates across the U.S. vary significantly by state, reflecting differences in distribution strategies, public health messaging, and local attitudes toward vaccines. For instance, states like Vermont and Massachusetts lead with over 75% of their populations fully vaccinated, while others, such as Mississippi and Alabama, lag behind with rates below 50%. This disparity highlights the complex interplay of socioeconomic factors, political climates, and access to healthcare resources. Understanding these variations is crucial for identifying regions at higher risk of outbreaks and tailoring interventions to improve vaccine uptake.
Analyzing the data reveals that states with higher vaccination rates often share common traits: robust public health infrastructure, proactive outreach campaigns, and strong partnerships with local communities. For example, California’s "Vaccinate All 58" initiative targeted underserved counties through mobile clinics and multilingual resources, contributing to its 70% vaccination rate. In contrast, states with lower rates frequently face challenges like vaccine hesitancy, limited healthcare access, and political polarization. A comparative study of these strategies can provide actionable insights for states struggling to boost their numbers.
To compare vaccine distribution and uptake effectively, consider these steps: first, examine state-level data on doses administered per capita, broken down by age groups (e.g., 12–17, 18–64, 65+). Second, assess the availability of vaccines in rural versus urban areas, as disparities often widen in less populated regions. Third, analyze the role of incentives—such as Ohio’s vaccine lottery or New York’s free MetroCards—in driving participation. By dissecting these elements, policymakers and advocates can identify gaps and replicate successful models.
Persuasively, it’s clear that addressing vaccine disparities requires more than just increasing supply. States with lower rates must tackle misinformation head-on through trusted messengers like local doctors or faith leaders. For example, West Virginia’s partnership with community pharmacies helped overcome hesitancy in rural areas. Additionally, offering flexible vaccination sites—such as pop-up clinics at schools or workplaces—can remove barriers for busy individuals. Practical tips for residents include checking state health department websites for nearby clinics and verifying insurance coverage for booster shots.
Descriptively, the landscape of vaccination rates by state paints a picture of both progress and persistent challenges. While some states celebrate milestones like 80% of eligible residents receiving at least one dose, others grapple with stagnant numbers despite ample supply. This patchwork of protection leaves pockets of vulnerability across the nation, underscoring the need for continued efforts. By learning from high-performing states and adapting strategies to local contexts, the U.S. can move closer to achieving herd immunity and safeguarding public health.
Morgan Wallen Concerts: Vaccination Requirements and Rules
You may want to see also
Explore related products






![]()
Age Group Vaccination: Analyze vaccination percentages among various age demographics in the U.S
As of recent data, vaccination rates in the U.S. vary significantly across age groups, reflecting both access disparities and generational attitudes toward health interventions. Adults aged 65 and older lead with over 90% having received at least one dose, driven by heightened vulnerability to severe COVID-19 outcomes. Conversely, adolescents aged 12–17 lag behind, with approximately 60% initiating vaccination, despite eligibility since mid-2021. This gap underscores the influence of parental hesitancy and misinformation on younger demographics.
Analyzing these trends reveals a clear correlation between age and vaccination uptake. Middle-aged adults (40–64) show moderate rates around 75%, balancing awareness of risk with varying levels of trust in medical systems. Young adults (18–39), however, exhibit lower compliance at roughly 65%, often attributed to perceptions of lower personal risk and competing priorities. Public health campaigns must address these age-specific barriers, emphasizing tailored messaging—such as school-based drives for teens or workplace incentives for young professionals—to bridge these divides.
A comparative lens highlights the success of senior vaccination efforts, which leveraged targeted outreach through Medicare networks and community partnerships. Such strategies could be adapted for younger groups by integrating vaccine access into routine pediatric visits or college health services. For instance, offering doses during sports physicals or orientation events could normalize vaccination for adolescents. Similarly, pop-up clinics at workplaces or social venues might resonate with young adults, removing logistical hurdles while fostering peer encouragement.
Persuasively, the data demands a shift from broad campaigns to age-segmented strategies. While older adults responded to risk-focused narratives, younger populations require messaging centered on collective responsibility and long-term health. For parents of teens, addressing safety concerns through pediatrician testimonials or debunking myths via trusted influencers could alleviate hesitancy. Practical tips include leveraging reminder systems for second doses and ensuring multilingual materials for diverse communities.
In conclusion, closing age-based vaccination gaps requires understanding each demographic’s unique motivations and challenges. By refining approaches—whether through policy adjustments, creative outreach, or localized solutions—the U.S. can achieve more equitable protection across generations. The lessons from senior vaccination success offer a blueprint, but adaptation is key to meeting younger cohorts where they are, both physically and psychologically.
Why Vaccinate? Key Reasons to Protect Your Health and Community
You may want to see also
Explore related products






![]()
Urban vs. Rural Areas: Examine vaccine coverage differences between urban and rural populations
As of recent data, urban areas in the U.S. consistently report higher COVID-19 vaccination rates compared to rural regions. For instance, metropolitan counties often exceed 70% full vaccination coverage, while many rural counties struggle to reach 50%. This disparity isn’t isolated to COVID-19 vaccines; it mirrors trends in flu vaccination and other preventive health measures. The gap highlights systemic challenges in rural healthcare access, from fewer pharmacies to limited public health infrastructure. Understanding these differences is critical for tailoring strategies to improve vaccine equity across geographic divides.
One major factor driving this urban-rural divide is the availability of vaccination sites. Urban centers typically host multiple hospitals, clinics, and pop-up vaccination hubs, often within walking distance or a short drive. In contrast, rural residents may face hour-long trips to the nearest vaccine provider, a barrier exacerbated by limited public transportation. For example, a study found that rural Americans are three times more likely to cite travel distance as a reason for vaccine hesitancy. Addressing this requires innovative solutions, such as mobile clinics or partnerships with local businesses to host vaccination events.
Beyond logistics, socioeconomic and cultural factors play a significant role. Rural populations often have higher rates of poverty and lower educational attainment, which correlate with vaccine hesitancy. Misinformation spreads more easily in tight-knit communities, where word-of-mouth can outweigh public health messaging. Urban areas, with their diverse populations and greater exposure to mainstream media, tend to have more robust health literacy. Bridging this gap demands localized, culturally sensitive campaigns that engage trusted community leaders, such as pastors or farmers, to advocate for vaccination.
Practical steps can help narrow the urban-rural vaccine gap. For rural areas, consider extending clinic hours to accommodate agricultural workers’ schedules or offering incentives like gift cards for local stores. Schools and churches can serve as vaccination sites, leveraging their central role in rural life. Urban strategies should focus on reaching underserved neighborhoods, such as deploying multilingual health workers in immigrant communities. By adapting approaches to the unique needs of each region, public health efforts can move closer to achieving equitable vaccine coverage nationwide.
Sipuleucel-T: Unveiling Its Unique Vaccine-Like Mechanism and Functionality
You may want to see also
Explore related products






![]()
Vaccine Hesitancy Trends: Explore factors contributing to vaccine hesitancy and its impact on percentages
As of recent data, approximately 67% of the U.S. population has received at least one dose of a COVID-19 vaccine, with about 60% fully vaccinated. These numbers, while significant, reveal a persistent gap in vaccination rates, largely driven by vaccine hesitancy. This reluctance isn’t uniform; it varies by region, age, and socioeconomic factors, creating pockets of vulnerability where outbreaks can thrive. Understanding these trends is critical to addressing the root causes and improving vaccination rates.
Analyzing the Factors Behind Hesitancy
Vaccine hesitancy stems from a complex interplay of misinformation, historical mistrust, and systemic barriers. For instance, surveys show that 40% of unvaccinated adults cite concerns about side effects, while 30% doubt the vaccine’s efficacy. Social media amplifies misinformation, with false claims about fertility, microchips, or long-term health risks spreading rapidly. Historically marginalized communities, such as African Americans, often point to past medical abuses (e.g., the Tuskegee Syphilis Study) as a reason for distrust. Additionally, logistical hurdles—like lack of transportation or paid time off for vaccination—disproportionately affect low-income populations, further widening disparities.
Regional Disparities and Their Consequences
Vaccination rates in the U.S. vary dramatically by state, with Vermont boasting a 78% fully vaccinated rate compared to Alabama’s 49%. These differences correlate with political leanings, education levels, and access to healthcare. In rural areas, where 20% of Americans live, vaccine access remains a challenge due to fewer clinics and pharmacies. The impact? Counties with lower vaccination rates have seen 3–5 times higher hospitalization rates during COVID-19 surges, straining local healthcare systems and prolonging the pandemic’s economic toll.
Strategies to Combat Hesitancy
To bridge the gap, tailored approaches are essential. For younger adults (ages 18–29), who have the lowest vaccination rates among eligible groups, peer-to-peer messaging and social media campaigns debunking myths can be effective. In communities of color, partnering with trusted local leaders—like clergy or community health workers—has shown promise. For example, pop-up clinics at churches or schools increased vaccination rates by 15% in pilot programs. Employers can also play a role by offering incentives like paid time off or gift cards for employees who get vaccinated.
The Long-Term Impact of Hesitancy
If current trends persist, vaccine hesitancy could hinder herd immunity, estimated to require 70–85% vaccination coverage. This leaves the door open for new variants to emerge, potentially requiring additional booster doses. For parents, hesitancy extends to childhood vaccines, with measles outbreaks already rising in states with lower vaccination rates. Addressing hesitancy isn’t just about COVID-19—it’s about rebuilding trust in public health systems to prevent future crises.
By dissecting these trends and implementing targeted solutions, we can move closer to protecting not just individuals, but entire communities.
Post-Vaccination Care: Soothing Your Baby After 2-Month Shots
You may want to see also
Explore related products






![]()
Booster Shot Uptake: Assess the percentage of the U.S. population receiving COVID-19 booster doses
As of recent data, approximately 70% of the U.S. population has received at least one dose of a COVID-19 vaccine, yet the uptake of booster shots paints a different picture. Only about 50% of fully vaccinated individuals have received a booster dose, leaving a significant portion of the population with waning immunity. This disparity raises concerns about ongoing protection against severe illness, hospitalization, and death, particularly among vulnerable populations.
Analyzing the booster shot uptake reveals stark differences across age groups. Among adults aged 65 and older, booster coverage hovers around 70%, reflecting a higher awareness of risk and adherence to health recommendations. In contrast, only about 40% of adults aged 18–49 have received a booster, despite this group comprising a substantial portion of the workforce and social interactions. Pediatric booster rates are even lower, with less than 30% of eligible adolescents aged 12–17 having received an additional dose. These variations underscore the need for targeted outreach and education tailored to specific demographics.
To improve booster shot uptake, public health strategies must address barriers such as misinformation, access issues, and complacency. For instance, mobile vaccination clinics in underserved communities and workplace vaccination drives can enhance accessibility. Clear messaging about the benefits of boosters, including reduced risk of severe outcomes from variants like Omicron, is essential. Additionally, integrating booster reminders into routine healthcare visits and leveraging trusted community leaders can encourage hesitant individuals to act.
A comparative look at global booster rates highlights the U.S.’s middling performance. Countries like Canada and the U.K. have achieved higher booster coverage through aggressive campaigns and streamlined distribution systems. The U.S. could adopt similar tactics, such as offering incentives (e.g., gift cards or paid time off) and simplifying appointment scheduling. Learning from international successes could help close the booster gap domestically.
Practically, individuals can take proactive steps to ensure they and their families are up to date on boosters. The CDC recommends a second booster for adults over 50 and certain immunocompromised individuals, while others should receive at least one booster five months after their initial series. Checking local pharmacies, clinics, or the Vaccines.gov website for availability is straightforward. For parents, discussing booster benefits with pediatricians and scheduling appointments during routine check-ups can ease concerns and streamline the process.
In conclusion, while primary COVID-19 vaccination rates in the U.S. are relatively high, booster shot uptake remains suboptimal, particularly among younger adults and adolescents. Addressing this gap requires a multi-faceted approach combining accessibility, education, and tailored outreach. By learning from global successes and empowering individuals with practical tools, the U.S. can bolster population-level immunity and better prepare for future waves of the virus.
Influenza Vaccine: Single Dose or Multiple Shots Explained
You may want to see also
Frequently asked questions
As of 2023, approximately 80-85% of the U.S. population has received at least one dose of the COVID-19 vaccine, though exact numbers may vary by source and date.
Around 68-72% of the U.S. population is considered fully vaccinated, depending on the definition of "fully vaccinated" and the latest data.
Vaccination rates are highest among older adults, with over 90% of individuals aged 65 and older fully vaccinated, while rates are lower among younger age groups, particularly children under 12.
Approximately 30-40% of the U.S. population has received at least one booster dose, with rates varying significantly by age, region, and other demographic factors.