Cervical cancer remains a significant global health concern, but advancements in vaccination have provided a powerful tool in its prevention. The human papillomavirus (HPV) vaccine, targeting the primary cause of cervical cancer, has been widely recognized for its efficacy in reducing the incidence of the disease. Studies indicate that HPV vaccination can prevent a substantial percentage of cervical cancer cases, with estimates suggesting it can avert up to 90% of cancers caused by the most common HPV types. This remarkable impact underscores the importance of widespread vaccination efforts in combating cervical cancer and highlights its role as a cornerstone of preventive healthcare.
| Characteristics | Values |
|---|---|
| Vaccine Types Covered | HPV vaccines (e.g., Gardasil 9, Cervarix) |
| HPV Types Prevented | High-risk types: HPV 16, 18, 31, 33, 45, 52, 58 (varies by vaccine) |
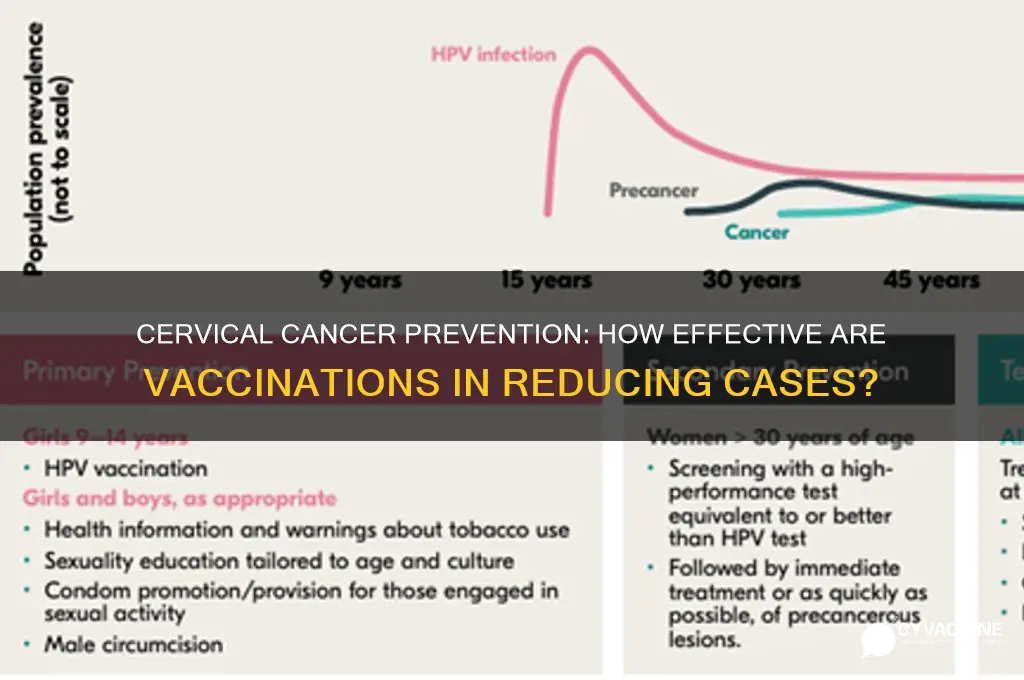
| Percent of Cervical Cancer Prevented | Up to 90% (when vaccinated before HPV exposure) |
| Efficacy Against Precancerous Lesions | Nearly 100% against cervical precancerous lesions caused by targeted HPV types |
| Population Coverage | Females and males (as HPV vaccination prevents other HPV-related cancers) |
| Age Recommendation | Ideally 9–14 years (catch-up through 26 years for females, 21 for males) |
| Duration of Protection | At least 10+ years (ongoing studies suggest long-term immunity) |
| Global Impact | Significant reduction in cervical cancer incidence in vaccinated populations |
| Limitations | Does not protect against all HPV types; does not treat existing infections |
| Source of Data | WHO, CDC, clinical trials, and meta-analyses (data as of 2023) |
Explore related products






What You'll Learn
![]()
HPV Vaccine Effectiveness Against Cervical Cancer
The HPV vaccine has been a game-changer in the fight against cervical cancer, significantly reducing the incidence of this disease worldwide. Studies show that the vaccine prevents 90% of cervical cancers when administered to girls and women aged 9 to 26 before HPV exposure. This remarkable effectiveness is attributed to its ability to target the high-risk HPV types 16 and 18, which are responsible for approximately 70% of all cervical cancer cases globally. By blocking these strains, the vaccine not only prevents cancer but also reduces the need for invasive procedures like colposcopies and biopsies.
To maximize the vaccine’s effectiveness, timing is crucial. The Centers for Disease Control and Prevention (CDC) recommends a two-dose schedule for individuals starting the series before their 15th birthday, with doses administered 6 to 12 months apart. For those who begin vaccination at ages 15 to 26, a three-dose schedule is advised, with the second dose given 1 to 2 months after the first and the third dose administered 6 months after the initial shot. Adhering to these schedules ensures optimal protection, as partial vaccination may not provide the full preventive benefits.
While the HPV vaccine is highly effective, it’s not a standalone solution. Regular cervical cancer screenings, such as Pap tests, remain essential even for vaccinated individuals. This is because the vaccine doesn’t protect against all cancer-causing HPV types, and screenings can detect precancerous changes early. Combining vaccination with routine screenings creates a robust defense against cervical cancer, reducing mortality rates by up to 70% in some populations.
A common misconception is that the HPV vaccine is only for women. In reality, it’s equally important for boys and men, as HPV can cause cancers of the penis, anus, and throat, in addition to genital warts. Vaccinating both genders not only protects individuals but also reduces the overall transmission of HPV, creating herd immunity. This dual approach underscores the vaccine’s role as a public health tool, not just a personal preventive measure.
Despite its proven effectiveness, HPV vaccination rates remain suboptimal in many regions due to misinformation and access barriers. Addressing these challenges requires education campaigns that highlight the vaccine’s safety and long-term benefits, as well as policies that improve affordability and availability. By increasing vaccination coverage, we can move closer to the World Health Organization’s goal of eliminating cervical cancer as a public health problem within the next century.
Gavin Newsom's Stance on Mandatory Vaccines: What You Need to Know
You may want to see also
Explore related products






![]()
HPV Types Covered by Vaccines
Cervical cancer is predominantly caused by persistent infections with high-risk human papillomavirus (HPV) types, primarily HPV 16 and 18, which together account for approximately 70% of cases globally. HPV vaccines, however, offer protection against a broader range of types, significantly reducing the risk of cervical cancer and other HPV-related diseases. Understanding which HPV types are covered by these vaccines is crucial for appreciating their preventive potential.
The first-generation HPV vaccines, such as Gardasil (quadrivalent) and Cervarix (bivalent), target HPV 16 and 18, the most carcinogenic types. Gardasil also protects against HPV 6 and 11, which cause 90% of genital warts but are low-risk for cancer. These vaccines have been shown to prevent nearly 100% of precancerous cervical lesions caused by the targeted types when administered before HPV exposure, typically recommended for adolescents aged 9–14 with a two-dose schedule. For those aged 15–26, a three-dose regimen is advised due to a less robust immune response in older individuals.
The second-generation vaccine, Gardasil 9, represents a significant advancement, covering nine HPV types: 6, 11, 16, 18, 31, 33, 45, 52, and 58. These additional types are responsible for another 15–20% of cervical cancers, bringing the total preventive potential to approximately 90% of cervical cancer cases. Gardasil 9 is administered in two doses for those under 15 and three doses for older individuals, offering broader protection and simplifying vaccination schedules by replacing earlier versions.
While HPV vaccines are highly effective against the types they cover, they do not protect against all high-risk HPV strains. Persistent infections with non-vaccine types (e.g., HPV 51 or 59) still pose a risk, albeit smaller. Therefore, regular cervical cancer screening remains essential, even for vaccinated individuals. Additionally, the vaccines are prophylactic, not therapeutic, meaning they prevent infection but do not treat existing HPV-related conditions.
In practice, maximizing the impact of HPV vaccination requires strategic implementation. Vaccinating before sexual debut ensures optimal efficacy, as HPV is primarily transmitted sexually. Public health efforts should focus on integrating vaccination into routine adolescent immunizations and addressing barriers such as cost, awareness, and hesitancy. For example, school-based programs have successfully increased uptake in countries like Australia and Rwanda, demonstrating the feasibility of high coverage rates.
In summary, HPV vaccines cover the most carcinogenic types responsible for the majority of cervical cancers, with Gardasil 9 offering protection against nine strains. While they significantly reduce cancer risk, ongoing screening and global vaccination efforts are vital to fully leverage their preventive potential. By targeting the right HPV types and ensuring widespread access, these vaccines can play a transformative role in eliminating cervical cancer as a public health threat.
Puerto Rico's Vaccine Triumph: How the Island Led America
You may want to see also
Explore related products






![]()
Global Cervical Cancer Prevention Rates
Cervical cancer remains a significant global health burden, with an estimated 604,000 new cases and 342,000 deaths annually. However, the introduction of HPV vaccines has revolutionized prevention efforts. Current data indicates that HPV vaccination can prevent 70-90% of cervical cancers, depending on vaccine coverage and the number of doses administered. This staggering figure underscores the vaccine’s potential to drastically reduce disease incidence, particularly in regions with high vaccination rates. For instance, countries like Australia and the UK have reported substantial declines in HPV infections and precancerous lesions among vaccinated populations, setting a benchmark for global prevention strategies.
To maximize the vaccine’s impact, adherence to recommended dosing schedules is critical. The World Health Organization (WHO) advises a two-dose regimen for girls aged 9–14, with doses administered 6–12 months apart. For individuals aged 15 and older, a three-dose schedule is recommended, spaced over 6 months. These guidelines are tailored to optimize immune response while ensuring accessibility, especially in low-resource settings. Notably, studies show that even a single dose can provide substantial protection, though two doses remain the gold standard for long-term efficacy.
Despite the vaccine’s proven effectiveness, global prevention rates vary widely due to disparities in access and awareness. High-income countries like the United States and Canada achieve vaccination coverage rates exceeding 70%, while many low-income nations struggle to reach 20%. This gap highlights the urgent need for equitable distribution and targeted public health campaigns. Initiatives like Gavi, the Vaccine Alliance, have made strides in subsidizing vaccine costs for developing countries, but sustained investment and infrastructure support are essential to bridge this divide.
A comparative analysis reveals that countries integrating HPV vaccination into national immunization programs and school-based delivery systems achieve higher coverage rates. For example, Rwanda’s successful campaign, which vaccinated over 93% of eligible girls, demonstrates the power of political commitment and community engagement. Conversely, regions with fragmented healthcare systems or cultural hesitancy face significant challenges. Addressing these barriers requires not only logistical solutions but also culturally sensitive education to dispel myths and build trust.
In conclusion, while HPV vaccination holds the key to preventing the majority of cervical cancers, its global impact hinges on universal access and strategic implementation. By prioritizing dose optimization, equitable distribution, and community-driven approaches, the world can move closer to eliminating cervical cancer as a public health threat. Practical steps include advocating for policy reforms, leveraging technology for outreach, and fostering partnerships between governments, NGOs, and healthcare providers. The data is clear: vaccination works, but its success depends on collective action.
Vaccines vs Infections: Which Offers Superior Immunity?
You may want to see also
Explore related products






![]()
Vaccine Impact on Precancerous Lesions
Cervical cancer begins with precancerous lesions, often caused by persistent human papillomavirus (HPV) infections. Vaccines targeting HPV types 16 and 18, responsible for approximately 70% of cervical cancers, have demonstrated profound effects on these lesions. Clinical trials show that HPV vaccination reduces the incidence of high-grade precancerous lesions by up to 93% in individuals without prior exposure to the virus. This statistic underscores the vaccine’s role in interrupting the progression from infection to cancer, making it a cornerstone of cervical cancer prevention.
Consider the mechanism: HPV vaccines stimulate the production of antibodies that neutralize the virus before it infects cervical cells. For optimal efficacy, the vaccine is administered in two or three doses, depending on the recipient’s age. Adolescents aged 9–14 receive two doses six months apart, while those 15 and older require three doses over six months. Early vaccination is critical, as it ensures protection before potential HPV exposure, thereby preventing the initial infection that leads to precancerous changes.
A comparative analysis reveals the vaccine’s impact across populations. In countries with high vaccination coverage, such as Australia and the UK, rates of precancerous lesions have plummeted. For instance, Australia’s national HPV vaccination program, introduced in 2007, led to a 90% reduction in high-grade cervical abnormalities among young women within a decade. Conversely, regions with lower vaccination rates continue to report higher lesion incidence, highlighting the direct correlation between vaccine uptake and disease prevention.
Despite its success, challenges remain. Vaccine hesitancy, misinformation, and access disparities limit its full potential. Public health initiatives must address these barriers through education, affordable access, and targeted outreach. For individuals, staying informed about vaccination schedules and adhering to them is crucial. Parents and caregivers should prioritize vaccinating children before they become sexually active, as this maximizes protection against HPV-related precancerous lesions.
In conclusion, the impact of HPV vaccination on precancerous lesions is transformative, offering a clear pathway to cervical cancer prevention. By understanding its mechanisms, adhering to dosing guidelines, and learning from global successes, societies can further reduce the burden of this disease. The vaccine’s ability to prevent up to 93% of high-grade lesions reinforces its status as a vital tool in public health, but its full potential depends on widespread adoption and informed action.
Vaccines and Autism: Debunking Myths About Donald Trump's Son
You may want to see also
Explore related products

$14.95





![]()
Long-Term Protection Duration Post-Vaccination
The HPV vaccine's long-term protection duration is a critical factor in its effectiveness against cervical cancer. Studies show that the vaccine provides robust immunity for at least 10 years post-vaccination, with some research suggesting protection could extend beyond 15 years. This extended duration is particularly significant because it covers the period when individuals are most at risk of HPV exposure, typically during their late teens and early twenties. For maximum efficacy, the CDC recommends a two-dose schedule for individuals aged 9 to 14, with doses administered 6 to 12 months apart. Those vaccinated at 15 or older require a three-dose series, spaced over 6 months, to ensure a comparable immune response.
Analyzing the data, the vaccine's longevity is attributed to its ability to induce high levels of neutralizing antibodies against HPV types 16 and 18, which cause approximately 70% of cervical cancer cases. A 2020 study published in *The Lancet* found that vaccinated individuals maintained antibody levels well above the protective threshold for over a decade. This sustained immunity is further supported by herd immunity effects, as widespread vaccination reduces the prevalence of HPV in the population. However, ongoing monitoring is essential to confirm whether booster doses will be necessary in the future, especially for those vaccinated in adolescence.
From a practical standpoint, ensuring long-term protection requires adherence to the recommended vaccination schedule and age-specific dosing. Parents and healthcare providers should prioritize vaccinating preteens at the earliest opportunity, ideally before potential HPV exposure. For young adults who missed early vaccination, completing the three-dose series is crucial. Additionally, maintaining a healthy lifestyle, including regular cervical cancer screenings, complements vaccine protection. While the vaccine significantly reduces cervical cancer risk, it does not cover all HPV types, so screenings remain vital for early detection.
Comparatively, the HPV vaccine's long-term protection outpaces that of many other vaccines, such as the flu shot, which requires annual administration. This durability underscores its role as a cornerstone of cervical cancer prevention. However, disparities in access and awareness persist, particularly in low-income regions, where vaccination rates lag. Addressing these gaps through education and policy initiatives is essential to maximize the vaccine's global impact. By combining widespread vaccination with continued research, we can move closer to eliminating cervical cancer as a public health threat.
Vaccine Economics: How Drug Companies Profit from Immunizations
You may want to see also
Frequently asked questions
The HPV vaccination prevents approximately 70-90% of cervical cancers, as it targets the most common high-risk HPV types (16 and 18) responsible for about 70% of cases.
No, the HPV vaccine protects against the high-risk HPV types that cause most cervical cancers, but not all. It prevents about 70-90% of cases, depending on the vaccine type and coverage.
Studies show the HPV vaccine is highly effective, reducing the risk of cervical cancer by 70-90% in those vaccinated before HPV exposure.
The HPV vaccine is most effective before HPV exposure. It does not treat existing infections but can still protect against other high-risk HPV types not yet acquired.
Yes, regular cervical cancer screenings (Pap tests or HPV tests) are crucial for early detection and prevention, even for vaccinated individuals.