The vaccination rate among individuals aged 65 and older is a critical metric for assessing public health resilience, particularly in the context of pandemics like COVID-19. This demographic is often prioritized due to their higher vulnerability to severe illness and complications. As of recent data, a significant percentage of this age group has been vaccinated, reflecting global efforts to protect the most at-risk populations. Understanding the exact percentage of vaccinated seniors provides insights into the success of immunization campaigns, highlights disparities in access, and informs strategies to address vaccine hesitancy or logistical challenges. This data is essential for policymakers, healthcare providers, and communities to ensure ongoing protection and reduce the burden on healthcare systems.
| Characteristics | Values (as of latest data, October 2023) |
|---|---|
| Percentage of 65+ Fully Vaccinated | ~95% (U.S. CDC data) |
| Percentage of 65+ with at least 1 dose | ~98% (U.S. CDC data) |
| Booster Dose Coverage (65+) | ~70% (U.S. CDC data) |
| Vaccine Type Most Commonly Used | mRNA vaccines (Pfizer-BioNTech, Moderna) |
| Regional Variations (U.S.) | Higher in Northeast, lower in Southeast |
| Global Comparison | U.S. and EU have ~90-95%, lower in LMICs |
| Impact on Hospitalization Rates | Reduced by ~90% compared to unvaccinated |
| Impact on Mortality Rates | Reduced by ~90% compared to unvaccinated |
| Primary Vaccine Hesitancy Reasons | Misinformation, access issues (in some regions) |
| Updated Vaccine Uptake (2023) | ~40% of 65+ received updated bivalent dose |
Explore related products






What You'll Learn
- Vaccination Rates by Age Group: Breakdown of vaccinated individuals aged 65+ by specific age ranges
- Geographic Vaccination Disparities: Regional differences in vaccination rates among the 65+ population
- Vaccine Type Distribution: Percentage of 65+ vaccinated by vaccine brand (e.g., Pfizer, Moderna)
- Booster Uptake in Seniors: Proportion of 65+ who have received at least one booster dose
- Vaccination Trends Over Time: Changes in 65+ vaccination rates since vaccine rollout began
![]()
Vaccination Rates by Age Group: Breakdown of vaccinated individuals aged 65+ by specific age ranges
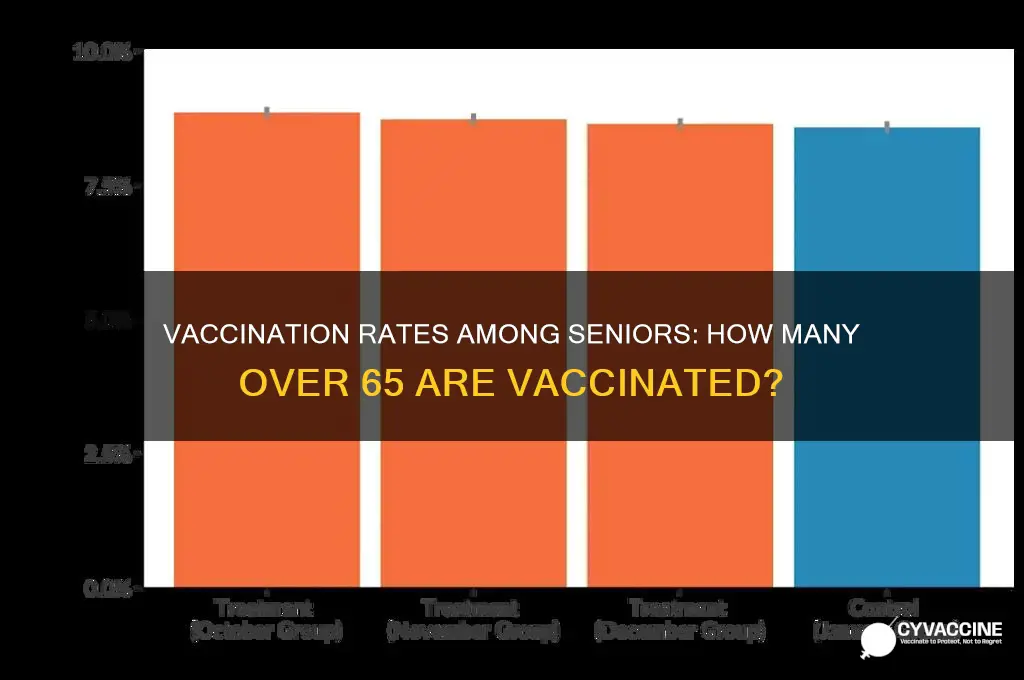
As of recent data, approximately 90% of individuals aged 65 and older in the United States have received at least one dose of a COVID-19 vaccine, with over 70% having completed their primary series and received at least one booster. However, these figures mask variations within this age group. Breaking down vaccination rates by specific age ranges—such as 65–74, 75–84, and 85+—reveals nuanced trends that highlight both successes and areas for improvement.
For the 65–74 age range, vaccination rates are among the highest within the 65+ cohort, often exceeding 95% for primary series completion. This group tends to be more mobile, tech-savvy, and engaged with healthcare systems, making them easier to reach through traditional vaccination campaigns. However, booster uptake drops slightly, with around 75% receiving at least one additional dose. Encouraging this group to stay current with boosters could involve targeted messaging about waning immunity and the benefits of updated vaccine formulations.
In contrast, the 75–84 age range shows a modest decline in vaccination rates, with approximately 90% completing the primary series and 65–70% receiving boosters. This dip may reflect increased health vulnerabilities, reduced mobility, or reliance on caregivers for healthcare access. Practical solutions include mobile vaccination clinics, partnerships with senior centers, and simplified appointment processes. Caregivers and family members can play a critical role by assisting with scheduling and transportation.
The 85+ age range presents the most significant challenges, with vaccination rates dropping to around 85% for the primary series and 55–60% for boosters. This group often faces barriers such as chronic illnesses, limited access to transportation, and higher levels of vaccine hesitancy among both individuals and their caregivers. Tailored interventions, such as in-home vaccination services and education campaigns addressing specific concerns (e.g., vaccine safety for those with comorbidities), are essential. Healthcare providers should also emphasize the heightened risk of severe outcomes in this age group to motivate action.
A comparative analysis reveals that while the 65+ population as a whole has achieved impressive vaccination coverage, disparities widen with age. These gaps underscore the need for age-specific strategies that address unique barriers. For instance, while digital reminders and online scheduling work well for younger seniors, older groups may require phone-based outreach or printed materials. Additionally, leveraging trusted community figures, such as local doctors or religious leaders, can enhance vaccine confidence across all age ranges.
In conclusion, understanding vaccination rates by specific age ranges within the 65+ demographic is crucial for refining public health strategies. By targeting interventions to the distinct needs of each subgroup—whether through accessibility improvements, tailored messaging, or caregiver involvement—we can close remaining gaps and ensure comprehensive protection for this vulnerable population.
Religious Refusals: Nurses' Ethical Dilemma on Vaccinations
You may want to see also
Explore related products






![]()
Geographic Vaccination Disparities: Regional differences in vaccination rates among the 65+ population
Vaccination rates among the 65+ population vary significantly across regions, revealing stark geographic disparities that cannot be ignored. For instance, data from the Centers for Disease Control and Prevention (CDC) shows that as of 2023, states like Vermont and Connecticut boast vaccination rates exceeding 90% for this age group, while states like Mississippi and Alabama lag behind at around 75%. These differences are not merely statistical anomalies but reflect deeper systemic issues influencing health outcomes.
Analyzing these disparities requires examining the interplay of socioeconomic factors, healthcare infrastructure, and cultural attitudes. Rural areas, for example, often face challenges such as limited access to vaccination sites, lower healthcare provider density, and higher rates of vaccine hesitancy. In contrast, urban centers with robust public health systems and higher population density tend to achieve higher vaccination rates. Additionally, states with higher median incomes and better health insurance coverage consistently outperform those with lower socioeconomic indicators. These patterns underscore the need for targeted interventions that address both logistical barriers and community-specific concerns.
To bridge the gap, public health initiatives must adopt a localized approach. For rural regions, mobile vaccination clinics and partnerships with local pharmacies can improve accessibility. Urban areas, while generally better served, may still have pockets of underserved populations, such as low-income neighborhoods or immigrant communities, requiring culturally sensitive outreach programs. For example, offering multilingual information sessions or collaborating with community leaders can enhance trust and participation. Furthermore, leveraging technology, such as appointment scheduling apps or SMS reminders, can streamline the vaccination process for all demographics.
A comparative analysis of successful campaigns highlights the importance of adaptability. In Vermont, high vaccination rates were achieved through a combination of strong state leadership, widespread public education, and efficient distribution networks. Conversely, Mississippi’s lower rates are partly attributed to historical mistrust of medical institutions and inadequate funding for public health programs. By studying these examples, policymakers can identify strategies that resonate with their specific regional contexts. For instance, regions with high hesitancy might benefit from peer-led education programs, while those with infrastructure gaps could prioritize resource allocation to underserved areas.
Ultimately, addressing geographic vaccination disparities among the 65+ population demands a multifaceted strategy. It involves not only improving access but also fostering trust and tailoring solutions to regional needs. Practical steps include mapping vaccination deserts, allocating funds to high-need areas, and engaging local stakeholders in campaign design. By doing so, we can ensure that older adults, regardless of where they live, have equitable opportunities to protect their health through vaccination.
Understanding Immunosuppression: How It Impacts Vaccine Effectiveness and Safety
You may want to see also
Explore related products






![]()
Vaccine Type Distribution: Percentage of 65+ vaccinated by vaccine brand (e.g., Pfizer, Moderna)
Among the 65+ population, vaccine brand preference and availability have significantly influenced vaccination rates. Data from the CDC reveals that Pfizer-BioNTech and Moderna mRNA vaccines dominate this demographic, with Johnson & Johnson’s adenovirus vector vaccine trailing behind. Understanding this distribution is critical, as each vaccine has unique dosing schedules and efficacy profiles tailored to older adults. For instance, Pfizer and Moderna require two primary doses followed by boosters, while J&J’s single-dose approach initially appealed to those seeking convenience, despite later recommendations for a second dose to enhance protection.
Analyzing the numbers, Pfizer-BioNTech accounts for approximately 60% of vaccinations in the 65+ group, largely due to its early rollout and widespread distribution through pharmacies and clinics. Moderna follows closely at around 35%, favored for its slightly higher efficacy in clinical trials against severe COVID-19 in older adults. Johnson & Johnson, at roughly 5%, faced challenges such as rare but serious side effects (e.g., thrombosis with thrombocytopenia syndrome) and later restrictions, limiting its uptake in this age group. These percentages reflect not only brand availability but also public trust and healthcare provider recommendations.
From a practical standpoint, older adults and caregivers should consider vaccine type when scheduling appointments. Pfizer and Moderna boosters, typically administered 5 months after the second dose, are crucial for maintaining immunity, especially against variants. For those who received J&J, the CDC now recommends a second dose (preferably mRNA) followed by an mRNA booster. Pharmacies like CVS and Walgreens often specify available brands online, allowing recipients to choose based on preference or availability. Additionally, mobile clinics and community centers frequently offer Moderna, making it a convenient option for those with limited mobility.
Comparatively, the mRNA vaccines (Pfizer and Moderna) have shown superior efficacy in preventing hospitalization and death in the 65+ population, with real-world data supporting their effectiveness across multiple variants. J&J, while less prevalent, remains a viable option for those with mRNA contraindications or preferences. However, its lower initial uptake in this age group highlights the importance of clear communication about risks and benefits. For example, a 70-year-old with a history of allergies might opt for Moderna due to its lower risk of anaphylaxis compared to Pfizer, as noted in VAERS data.
In conclusion, the vaccine type distribution among the 65+ population underscores the dominance of mRNA vaccines and the nuanced factors influencing brand selection. By understanding these trends, older adults can make informed decisions about their vaccination and booster schedules. Healthcare providers should continue to emphasize the importance of completing the recommended series, regardless of brand, to ensure optimal protection against COVID-19. Practical steps, such as checking vaccine availability at local sites and discussing options with a physician, can further empower this vulnerable demographic to stay safe.
Elderly Safety: Risks of Unvaccinated Kids in Close Proximity
You may want to see also
Explore related products





![]()
Booster Uptake in Seniors: Proportion of 65+ who have received at least one booster dose
As of recent data, approximately 70% of individuals aged 65 and older in the United States have received at least one booster dose of the COVID-19 vaccine. This figure highlights a critical aspect of vaccine efficacy: while initial vaccination rates among seniors are high, booster uptake is essential for maintaining robust immunity against emerging variants. The 65+ age group is particularly vulnerable to severe outcomes from COVID-19, making booster doses a vital component of their protection strategy. However, the 30% who remain unboosted represent a gap in immunity that could have significant public health implications.
Analyzing the factors influencing booster uptake reveals a mix of accessibility, awareness, and hesitancy. Seniors in urban areas with easy access to healthcare facilities are more likely to receive boosters compared to those in rural regions, where transportation and availability of vaccines can be barriers. Additionally, misinformation and waning urgency post-initial vaccination contribute to hesitancy. For instance, some seniors may mistakenly believe their initial doses provide lifelong immunity, while others may underestimate the risk of new variants. Addressing these misconceptions through targeted education campaigns could significantly improve booster rates.
From a practical standpoint, increasing booster uptake among seniors requires a multi-faceted approach. Healthcare providers should proactively reach out to patients aged 65+ with personalized reminders and clear information about the benefits of boosters. Mobile vaccination clinics can bridge the accessibility gap in rural areas, while community centers and senior living facilities can host on-site clinics. For those with mobility issues, offering in-home vaccination services could be a game-changer. Additionally, leveraging trusted figures like local doctors or community leaders to endorse boosters can build confidence and dispel myths.
Comparatively, countries with higher booster rates among seniors often share common strategies: strong government-led campaigns, simplified scheduling processes, and incentives like health screenings or small rewards. For example, Israel’s early rollout of boosters was accompanied by a clear messaging campaign emphasizing the increased risk to older adults, resulting in over 80% uptake in the 65+ demographic. The U.S. could adopt similar tactics, such as integrating booster reminders into Medicare wellness visits or partnering with pharmacies to offer same-day appointments.
In conclusion, while 70% booster uptake among seniors is a solid foundation, closing the gap requires addressing logistical, informational, and psychological barriers. By combining accessibility improvements, targeted education, and proven strategies from high-performing countries, public health officials can ensure that a greater proportion of this vulnerable population remains protected. The goal is not just to increase numbers but to safeguard lives through sustained immunity.
Understanding the Ingredients: What's Inside the COVID-19 Vaccine?
You may want to see also
Explore related products






![]()
Vaccination Trends Over Time: Changes in 65+ vaccination rates since vaccine rollout began
The initial COVID-19 vaccine rollout prioritized the 65+ population due to their heightened vulnerability to severe illness and death. By early 2021, just months after vaccines became available, over 75% of this age group in the U.S. had received at least one dose, a testament to both the urgency of the situation and the effectiveness of targeted distribution strategies. This rapid uptake was critical in reducing hospitalizations and fatalities among seniors, setting a benchmark for vaccine campaigns worldwide.
However, the pace of vaccination slowed significantly as the year progressed. By mid-2021, while over 80% of the 65+ population was fully vaccinated, the rate of new vaccinations plateaued. This stagnation was partly due to vaccine hesitancy, logistical barriers, and a false sense of security as infection rates temporarily declined. Public health officials responded by emphasizing booster shots, particularly as new variants emerged, but uptake was uneven. For instance, by early 2022, only about 50% of vaccinated seniors had received a first booster, highlighting the challenge of maintaining momentum in vaccination campaigns.
A comparative analysis reveals striking disparities in vaccination rates among the 65+ population across different regions and demographics. Urban areas consistently outpaced rural regions, with access to healthcare facilities and higher awareness contributing to this gap. Additionally, racial and ethnic minorities within this age group often faced lower vaccination rates due to systemic barriers, such as language, transportation, and mistrust in healthcare systems. These disparities underscore the need for tailored interventions, such as mobile clinics and culturally sensitive outreach programs, to ensure equitable vaccine distribution.
To sustain and improve vaccination rates among seniors, practical steps must be taken. First, healthcare providers should proactively communicate the importance of boosters and additional doses, especially for those with comorbidities. Second, community-based initiatives, such as local vaccination drives and partnerships with senior centers, can address logistical hurdles. Finally, leveraging technology, such as reminder systems and telehealth consultations, can enhance accessibility and encourage timely vaccinations. By combining these strategies, we can ensure that the 65+ population remains protected against evolving threats.
Non-Medical Exemptions: Hindering Medical Progress and Public Health Advances
You may want to see also
Frequently asked questions
As of recent data, approximately 90-95% of individuals aged 65 and older in the U.S. are fully vaccinated against COVID-19, though percentages may vary by state and source.
The 65 and older age group consistently has the highest vaccination rate compared to younger age groups, with rates significantly outpacing those of younger adults and children.
The percentage typically refers to initial full vaccination (primary series), but many in this age group have also received booster shots, with booster rates often exceeding 60-70%.
This age group is at higher risk for severe COVID-19 outcomes, so public health campaigns and early vaccine eligibility prioritized them, leading to higher uptake.