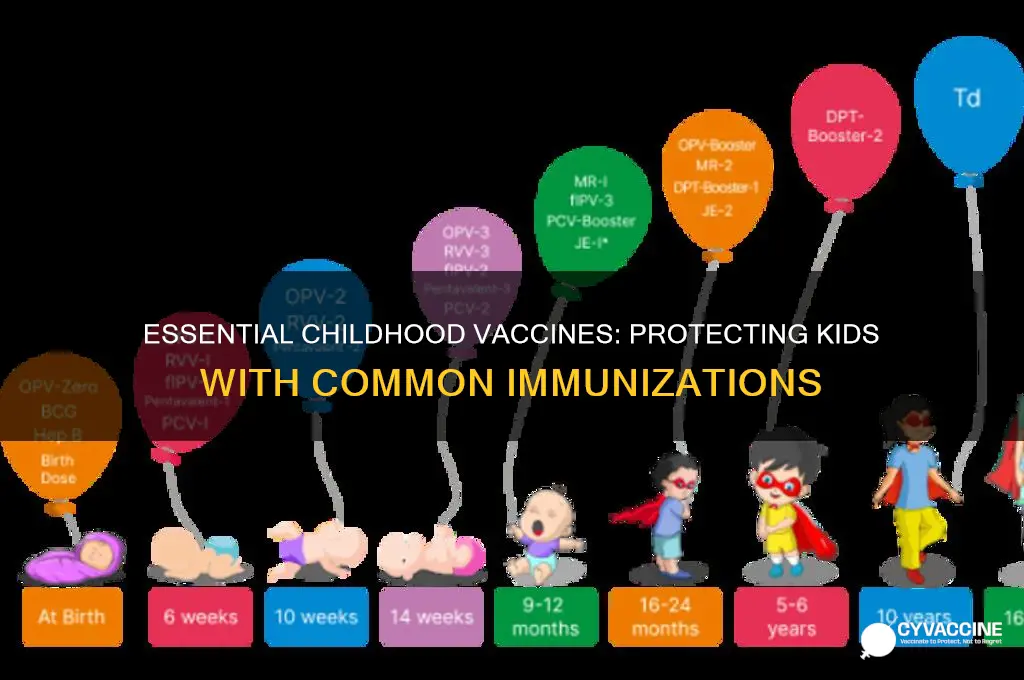
Childhood vaccinations are a cornerstone of public health, protecting children from serious and potentially life-threatening diseases. Common vaccines recommended for children include the MMR vaccine (measles, mumps, and rubella), DTaP (diphtheria, tetanus, and pertussis), IPV (inactivated poliovirus), Hib (Haemophilus influenzae type b), PCV (pneumococcal conjugate), Rotavirus, Hepatitis A and B, Varicella (chickenpox), and Influenza (flu). These vaccines are typically administered in a scheduled series starting from infancy to ensure immunity during critical developmental stages. Each vaccine is rigorously tested for safety and efficacy, and their widespread use has led to the near-elimination of many once-common childhood diseases. Following the recommended immunization schedule is crucial to safeguarding children’s health and preventing outbreaks in communities.
| Characteristics | Values |
|---|---|
| Vaccine Types | DTaP (Diphtheria, Tetanus, Pertussis), MMR (Measles, Mumps, Rubella), IPV (Inactivated Polio Vaccine), Hib (Haemophilus influenzae type b), Hepatitis A, Hepatitis B, Varicella (Chickenpox), PCV (Pneumococcal Conjugate Vaccine), Rotavirus, Influenza (Flu), Meningococcal, HPV (Human Papillomavirus) |
| Age Range | Birth to 18 years, with specific schedules for each vaccine |
| Dosage Schedule | Varies by vaccine; e.g., DTaP: 5 doses (2, 4, 6, 15-18 months, 4-6 years) |
| Administration Method | Primarily intramuscular (IM) or subcutaneous (SC) injection |
| Common Side Effects | Mild fever, soreness at injection site, fussiness, fatigue |
| Protection Duration | Varies; some require boosters (e.g., Tdap for teens), others lifelong |
| Global Recommendations | Endorsed by WHO, CDC, and national health authorities |
| Purpose | Prevent infectious diseases, reduce morbidity and mortality |
| Safety Profile | Rigorously tested and monitored for safety and efficacy |
| Availability | Widely available in most countries, often subsidized or free |
| Combination Vaccines | Available (e.g., MMRV, DTaP-IPV-Hib) to reduce number of shots |
| Storage Requirements | Typically refrigerated (2-8°C) to maintain potency |
| Contraindications | Severe allergic reaction to a previous dose, specific medical conditions |
Explore related products



$27.74 $32.99



What You'll Learn
- Routine childhood immunizations: MMR, DTaP, IPV, Hib, PCV, and flu vaccines
- Hepatitis A and B vaccines for liver protection in early childhood
- Varicella vaccine to prevent chickenpox and its complications in kids
- Rotavirus vaccine to reduce severe diarrhea and dehydration in infants
- Meningococcal vaccine for protection against bacterial meningitis in older children
![]()
Routine childhood immunizations: MMR, DTaP, IPV, Hib, PCV, and flu vaccines
Childhood immunizations are a cornerstone of public health, protecting young lives from preventable diseases. Among the most critical are the MMR (Measles, Mumps, Rubella), DTaP (Diphtheria, Tetanus, Pertussis), IPV (Inactivated Polio Vaccine), Hib (Haemophilus influenzae type b), PCV (Pneumococcal Conjunctive Vaccine), and flu vaccines. These vaccines are administered according to a standardized schedule, typically beginning at birth and continuing through adolescence, to ensure maximum efficacy and protection.
The MMR vaccine is a prime example of a combination vaccine, shielding children from three highly contagious diseases. Administered in two doses, the first at 12-15 months and the second at 4-6 years, it boasts a 97% effectiveness rate against measles after both doses. Measles, a once-common childhood illness, can lead to severe complications like pneumonia and encephalitis. Mumps and rubella, though less severe, can still cause significant health issues, including deafness and congenital rubella syndrome. Parents should be aware that mild side effects, such as fever or rash, may occur but are far outweighed by the vaccine's benefits.
In contrast, the DTaP vaccine targets three bacterial infections with a single shot. Given in a series of five doses starting at 2 months, with boosters at 4-6 years and 11-12 years, it provides robust protection against diphtheria, tetanus, and pertussis. Pertussis, or whooping cough, is particularly dangerous for infants, who may experience severe coughing fits leading to breathing difficulties. Tetanus, caused by a toxin-producing bacterium, can result in painful muscle stiffness and lockjaw. Diphtheria, though rare in the U.S., can cause a thick coating in the throat, leading to breathing problems. Ensuring timely vaccination is crucial, as delays can leave children vulnerable during critical developmental stages.
IPV, Hib, and PCV vaccines address specific yet significant threats. The IPV vaccine, administered in four doses starting at 2 months, protects against poliovirus, which can cause paralysis. Hib vaccine, given in three or four doses depending on the brand, prevents infections like meningitis and pneumonia caused by Haemophilus influenzae type b. PCV, typically given in four doses, safeguards against pneumococcal bacteria, a leading cause of ear infections, pneumonia, and bloodstream infections in children. These vaccines are often combined with others to streamline the immunization process, reducing the number of shots required while maintaining high efficacy.
Lastly, the annual flu vaccine is a vital component of childhood immunizations, recommended for all children aged 6 months and older. Influenza viruses evolve rapidly, necessitating yearly updates to the vaccine. While its effectiveness varies by season, it remains the best defense against flu-related complications, such as pneumonia and hospitalization. Parents can opt for the traditional shot or the nasal spray vaccine, depending on their child’s age and health status. Scheduling the flu vaccine early in the season ensures protection during peak flu months, typically between December and February.
Practical tips for parents include keeping a detailed record of vaccinations, scheduling appointments well in advance, and discussing any concerns with healthcare providers. Mild side effects like soreness at the injection site or low-grade fever are common and manageable with over-the-counter remedies. By adhering to the recommended immunization schedule, parents can provide their children with a strong foundation for lifelong health, reducing the risk of severe illnesses and contributing to community-wide immunity.
Exploring the Latest Advances in HIV Vaccine Development and Names
You may want to see also
Explore related products






![]()
Hepatitis A and B vaccines for liver protection in early childhood
Hepatitis A and B are viral infections that can cause severe liver damage, but they are largely preventable through vaccination. These vaccines are cornerstone components of childhood immunization schedules worldwide, offering robust protection during the early years when the liver is particularly vulnerable. The Hepatitis A vaccine is typically administered in two doses, starting at 12 months of age, with a minimum interval of 6 months between doses. For Hepatitis B, the vaccination series begins at birth, with three doses given at 0, 1–2 months, and 6–18 months of age. This early intervention is critical, as children infected with Hepatitis B are more likely to develop chronic liver disease, including cirrhosis and liver cancer, later in life.
The rationale behind vaccinating children against Hepatitis A and B is both preventive and pragmatic. Hepatitis A is primarily spread through contaminated food or water, while Hepatitis B is transmitted through bodily fluids, often from mother to child during birth or through close contact. By vaccinating children early, public health systems aim to create herd immunity and reduce the overall disease burden. For instance, countries with high vaccination rates for Hepatitis B have seen a dramatic decline in childhood liver disease cases. Parents should ensure their children receive these vaccines on schedule, as delays can leave them susceptible during critical developmental stages.
A comparative analysis of these vaccines reveals their unique benefits and shared goals. While both protect the liver, the Hepatitis A vaccine is often combined with other vaccines, such as for Hepatitis B or diphtheria, tetanus, and pertussis (DTaP), to streamline administration. The Hepatitis B vaccine, however, is frequently given as a standalone shot, especially in newborns. Both vaccines have proven safe and effective, with mild side effects like soreness at the injection site or low-grade fever. Notably, the Hepatitis B vaccine is one of the first given to newborns, underscoring its importance in preventing vertical transmission from infected mothers.
Practical tips for parents include scheduling vaccinations during well-child visits to ensure consistency and discussing combination vaccines with healthcare providers to minimize the number of shots. For families traveling to regions with high Hepatitis A prevalence, accelerating the vaccine schedule may be advisable, but this should be done under medical guidance. Additionally, maintaining a record of vaccination dates is essential, as some schools and childcare facilities require proof of immunization. By prioritizing these vaccines, parents can safeguard their children’s liver health and contribute to broader public health goals.
In conclusion, the Hepatitis A and B vaccines are indispensable tools in early childhood liver protection. Their inclusion in routine immunization schedules reflects their proven efficacy and the severe consequences of the diseases they prevent. Parents and caregivers play a vital role in ensuring timely vaccination, while healthcare providers must continue educating families about the long-term benefits of these vaccines. Together, these efforts can reduce the global burden of hepatitis and secure healthier futures for children worldwide.
Childhood Vaccination Schedule in 1963: A Comprehensive Overview
You may want to see also
Explore related products






![]()
Varicella vaccine to prevent chickenpox and its complications in kids
Chickenpox, a highly contagious disease caused by the varicella-zoster virus, was once a common childhood illness, often dismissed as a mild rite of passage. However, complications such as bacterial infections, pneumonia, and encephalitis can arise, particularly in infants, adolescents, and those with weakened immune systems. The varicella vaccine, introduced in the mid-1990s, has dramatically reduced the incidence of chickenpox and its associated risks. Administered in two doses—the first at 12–15 months and the second at 4–6 years—this live-attenuated vaccine provides robust immunity in over 90% of recipients. Its effectiveness extends beyond individual protection, contributing to herd immunity and minimizing outbreaks in communities.
From a practical standpoint, parents should be aware of the vaccine’s safety profile and potential side effects. Mild reactions, such as soreness at the injection site, fever, or a temporary rash, are common but rarely cause concern. The vaccine is contraindicated for children with severe allergies to neomycin or gelatin, as well as those with compromised immune systems. For families planning international travel, ensuring children are vaccinated is crucial, as chickenpox remains prevalent in regions with lower immunization rates. Adhering to the recommended schedule is key, as delaying doses can leave children vulnerable during peak exposure ages.
A comparative analysis highlights the varicella vaccine’s impact versus historical management of chickenpox. Before its introduction, annual cases in the U.S. exceeded 4 million, with 10,000 hospitalizations and 100 deaths. Post-vaccination, these numbers have plummeted by over 90%, demonstrating the vaccine’s efficacy. Unlike natural infection, which confers lifelong immunity but carries risks, the vaccine offers a safer alternative with minimal adverse effects. While breakthrough cases can occur, they are typically milder, underscoring the vaccine’s role in disease mitigation rather than complete eradication.
Persuasively, the varicella vaccine is a cornerstone of pediatric preventive care, aligning with broader public health goals. Its inclusion in routine immunization schedules reflects global consensus on its benefits. Parents play a pivotal role in ensuring uptake, as hesitancy or misinformation can hinder progress. By protecting children from chickenpox, the vaccine also prevents shingles later in life, as the virus can reactivate as the immune system ages. This dual benefit reinforces its value, making it a non-negotiable component of childhood health.
Instructively, caregivers should monitor children post-vaccination for rare but serious reactions, such as severe allergic responses or persistent crying. Keeping a record of vaccination dates and sharing it with healthcare providers ensures continuity of care. For children who miss doses, catch-up schedules are available, though timely adherence is ideal. Schools and daycare centers often require proof of vaccination, emphasizing its societal importance. By prioritizing the varicella vaccine, parents safeguard not only their children but also contribute to a healthier, more resilient community.
Vaccination Status: Polite Ways to Inquire Guests' COVID-19 Vaccination
You may want to see also
Explore related products






![]()
Rotavirus vaccine to reduce severe diarrhea and dehydration in infants
Rotavirus is a leading cause of severe diarrhea and dehydration in infants and young children worldwide, particularly in developing countries. Before the introduction of the rotavirus vaccine, this highly contagious virus was responsible for millions of hospitalizations and hundreds of thousands of deaths annually in children under five. The development and widespread adoption of the rotavirus vaccine have significantly reduced the global burden of this disease, making it a cornerstone of pediatric immunization programs.
The rotavirus vaccine is administered orally, typically in a liquid form, and is given in a series of doses to ensure robust immunity. In most countries, the first dose is recommended at 6 weeks of age, followed by additional doses at 2-month intervals, with the final dose administered by 6 months of age. This schedule may vary slightly depending on the specific vaccine brand and regional guidelines. For example, the RotaTeq vaccine is given in three doses, while the Rotarix vaccine requires only two doses. Adhering to the recommended schedule is crucial, as it ensures optimal protection during the period when infants are most vulnerable to severe rotavirus infections.
One of the key advantages of the rotavirus vaccine is its safety and efficacy profile. Clinical trials have demonstrated that the vaccine reduces the risk of severe rotavirus gastroenteritis by 85–98%, depending on the setting. Even in cases where vaccinated children still contract the virus, the symptoms are typically milder, with a lower risk of dehydration and hospitalization. This not only alleviates the suffering of the child but also reduces the economic and emotional burden on families and healthcare systems. Parents should be reassured that the vaccine is well-tolerated, with mild side effects such as irritability or temporary diarrhea being rare.
Despite its proven benefits, rotavirus vaccine coverage remains uneven globally, particularly in low-income regionsRotavirus is a leading cause of severe diarrhea and dehydration in infants and young children worldwide, particularly in developing countries. Before the introduction of the rotavirus vaccine, this highly contagious virus was responsible for millionsRotavirus is a leading cause of severe diarrhea and dehydration in infants and young children worldwide, particularly in developing countries. Before the introduction of the rotavirus vaccine, this highly contagious virus was responsible for millions of hospitalizations and hundreds of thousands of deaths annually in children under five. The vaccine, administered orally, has proven to be a game-changer in pediatric health, significantly reducing the incidence of severe rotavirus infections and their complications. Its impact is so profound that the World Health Organization (WHO) recommends its inclusion in all national immunization programs.
The rotavirus vaccine is typically given in a series of doses, starting as early as 6 weeks of age, depending on the specific vaccine brand and regional guidelines. For example, the RotaTeq vaccine is administered in three doses at 2, 4, and 6 months, while the Rotarix vaccine requires only two doses, usually at 2 and 4 months. The oral delivery method is not only child-friendly but also ensures the vaccine targets the intestinal tract, where rotavirus primarily replicates. Parents should be aware that mild side effects, such as temporary diarrhea or fussiness, may occur, but these are far outweighed by the vaccine’s benefits.
One of the most compelling aspects of the rotavirus vaccine is its herd immunity potential. As vaccination rates increase, the virus circulates less in communities, protecting even unvaccinated individuals, including those too young to receive the vaccine. This collective benefit underscores the importance of adhering to the recommended immunization schedule. However, it’s crucial to note that the vaccine does not provide 100% protection against rotavirus infection, but it dramatically reduces the severity of symptoms, preventing life-threatening dehydration and hospitalizations.
Practical tips for parents include ensuring the vaccine is administered on time and avoiding feeding infants immediately before or after vaccination, as this could reduce the vaccine’s effectiveness. Additionally, maintaining good hygiene practices, such as frequent handwashing, complements vaccination efforts by reducing the spread of the virus. For families in resource-limited settings, where access to medical care may be challenging, the rotavirus vaccine is a critical tool in preventing severe illness and the economic burden associated with treatment.
In conclusion, the rotavirus vaccine stands as a cornerstone in pediatric preventive care, offering a simple yet powerful solution to a once-devastating illness. Its oral administration, early dosing schedule, and proven efficacy make it an essential component of childhood immunization. By protecting infants from severe diarrhea and dehydration, this vaccine not only saves lives but also contributes to healthier, more resilient communities. Parents and healthcare providers alike play a vital role in ensuring widespread adoption and adherence to this life-saving intervention.
Upload Your Vaccine Certificate to PeduliLindungi App: A Quick Guide
You may want to see also
Explore related products






![]()
Meningococcal vaccine for protection against bacterial meningitis in older children
Bacterial meningitis is a rare but potentially life-threatening infection that can cause severe complications, including brain damage, hearing loss, and even death. Older children and adolescents are particularly vulnerable to meningococcal disease, which is why the meningococcal vaccine is a crucial component of their immunization schedule. This vaccine protects against Neisseria meningitidis, the bacterium responsible for meningococcal meningitis and sepsis.
Understanding the Vaccine
The meningococcal vaccine comes in two primary forms: MenACWY and MenB. MenACWY covers four serogroups (A, C, W, and Y) and is recommended for preteens and teens, typically administered at age 11 or 12, with a booster dose at age 16. MenB, which protects against serogroup B, is given in a series of two or three doses, depending on the brand, and is often recommended for high-risk individuals or as an option for broader protection. Both vaccines are highly effective in preventing meningococcal disease, though they do not provide lifelong immunity, hence the need for boosters.
Administration and Timing
The Centers for Disease Control and Prevention (CDC) advises that the MenACWY vaccine be given during the preteen years, with the booster dose following four to five years later. This timing ensures optimal protection during adolescence, when the risk of infection is highest. MenB vaccination, if elected, should begin at age 16–18 or earlier for those at increased risk, such as individuals with complement deficiencies or asplenia. Healthcare providers will determine the appropriate schedule based on individual risk factors and vaccine availability.
Practical Tips for Parents
Parents should ensure their children receive the meningococcal vaccine as part of their routine immunizations. Scheduling appointments during back-to-school checkups can help integrate the vaccine into existing healthcare routines. It’s also important to monitor for mild side effects, such as soreness at the injection site, headache, or fatigue, which are common and typically resolve within a few days. Keeping a record of vaccination dates and sharing this information with school health services can aid in maintaining compliance with local immunization requirements.
The Broader Impact
Beyond individual protection, widespread meningococcal vaccination contributes to herd immunity, reducing the overall prevalence of the disease in communities. This is particularly critical in settings like college dormitories, where close living conditions can facilitate the spread of bacteria. By vaccinating older children, parents not only safeguard their own families but also play a role in protecting vulnerable populations, such as infants too young to receive the vaccine. In this way, the meningococcal vaccine is both a personal and public health imperative.
Sore Throat After Booster Vaccine: Common Side Effect or Concern?
You may want to see also
Frequently asked questions
Common vaccines for infants in their first year include the Hepatitis B (HepB) vaccine, Rotavirus (RV) vaccine, Diphtheria, Tetanus, and Pertussis (DTaP) vaccine, Haemophilus influenzae type b (Hib) vaccine, Pneumococcal conjugate (PCV) vaccine, and Inactivated Poliovirus (IPV) vaccine.
The MMR vaccine is typically given in two doses, with the first dose administered between 12 and 15 months of age and the second dose between 4 and 6 years old.
Yes, the Flu vaccine is recommended annually for children aged 6 months and older to protect against seasonal influenza.
The Varicella vaccine protects against chickenpox. It is typically given in two doses, with the first dose administered between 12 and 15 months and the second dose between 4 and 6 years old.
Yes, common vaccines for preteens and teenagers include the Human Papillomavirus (HPV) vaccine, Tetanus, Diphtheria, and Pertussis (Tdap) booster, and Meningococcal conjugate (MenACWY) vaccine.