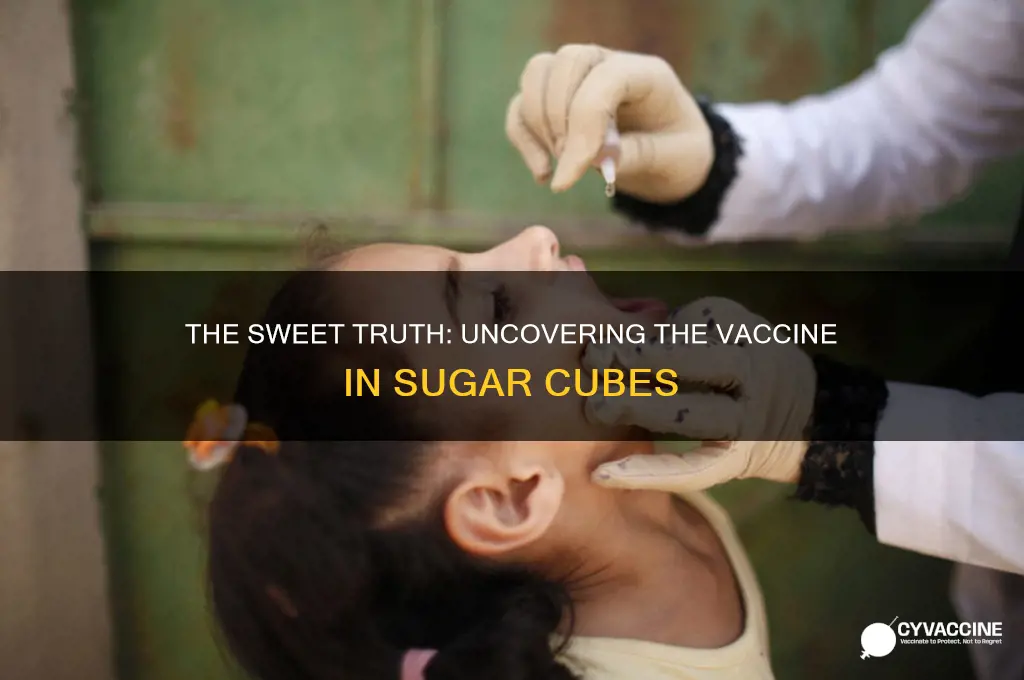
The sugar cube vaccine, a symbol of a bygone era in public health, was a key player in the global effort to eradicate polio. Introduced in the late 1950s and early 1960s, these sugar cubes were infused with the Sabin oral polio vaccine (OPV), developed by Dr. Albert Sabin. Unlike the injectable inactivated polio vaccine (IPV) created by Dr. Jonas Salk, the OPV was a live, attenuated vaccine administered orally, making it easier to distribute and more accessible, especially for mass immunization campaigns. The sugar cubes not only masked the taste of the vaccine but also made the process more appealing, particularly to children, contributing significantly to the widespread adoption of polio vaccination and the eventual decline of the disease worldwide.
| Characteristics | Values |
|---|---|
| Vaccine Type | Oral Polio Vaccine (OPV) |
| Specific Strain | Sabin strains (types 1, 2, and 3) |
| Administration Method | Oral, often delivered on a sugar cube |
| Developer | Albert Sabin |
| Introduction Year | 1961 (widely adopted) |
| Purpose | Prevention of poliomyelitis (polio) |
| Formulation | Live attenuated virus |
| Storage Requirement | Refrigerated (2-8°C) |
| Dosage | Typically 2 drops (for modern OPV, equivalent to sugar cube dose) |
| Immunity Type | Mucosal and humoral immunity |
| Effectiveness | High (over 95% after multiple doses) |
| Side Effects | Rarely, vaccine-associated paralytic polio (VAPP) |
| Current Use | Phased out in many countries in favor of Inactivated Polio Vaccine (IPV) due to VAPP risk |
| Historical Significance | Key tool in global polio eradication efforts |
Explore related products






What You'll Learn
- Polio Vaccine Type: The sugar cubes contained the oral polio vaccine (OPV), a live attenuated virus
- Sabin vs. Salk: OPV (Sabin) was in cubes, unlike the injected inactivated vaccine (Salk)
- Mass Immunization: Sugar cubes made OPV administration easy for large-scale campaigns in the 1960s
- Stability in Cubes: The vaccine remained stable in sugar cubes, ensuring effective delivery
- Global Eradication: Sugar cube vaccines played a key role in reducing polio cases worldwide
![]()
Polio Vaccine Type: The sugar cubes contained the oral polio vaccine (OPV), a live attenuated virus
The sugar cubes that became a symbol of polio eradication in the mid-20th century contained the oral polio vaccine (OPV), a groundbreaking innovation in disease prevention. Unlike injectable vaccines, OPV uses a live attenuated virus, meaning the virus is weakened but still alive, allowing it to stimulate a robust immune response without causing the disease. This method was particularly effective because it mimicked natural infection, providing both mucosal and systemic immunity. The vaccine was administered in a single dose of 0.1 mL, typically given to children aged 6 weeks and older, often in public health campaigns that reached millions.
One of the key advantages of OPV was its ease of administration. The vaccine was mixed with sugar cubes to make it palatable and child-friendly, a strategy that significantly boosted compliance. Parents were instructed to ensure their children consumed the entire cube without chewing, as this could reduce the vaccine’s effectiveness. The simplicity of this approach allowed for mass immunization campaigns, particularly in developing countries where access to healthcare infrastructure was limited. However, it’s important to note that OPV required proper storage at 2–8°C to maintain its potency, a logistical challenge in regions with unreliable refrigeration.
While OPV played a pivotal role in reducing polio cases by 99% globally, it is not without drawbacks. The live attenuated virus in OPV can, in rare cases, revert to a virulent form, causing vaccine-associated paralytic polio (VAPP) at a rate of about 1 in 2.7 million doses. Additionally, the vaccine can shed in stool, potentially spreading the weakened virus to unvaccinated individuals. These risks have led to the phased replacement of OPV with the inactivated polio vaccine (IPV) in many countries, though OPV remains essential in regions where polio is still endemic due to its ability to interrupt person-to-person transmission.
For those administering OPV today, practical tips include ensuring the vaccine is administered on an empty stomach for optimal absorption and avoiding concurrent antibiotics, which can interfere with the vaccine’s efficacy. Health workers should also educate caregivers about the importance of completing the full vaccination series, typically three doses spaced 4–8 weeks apart, followed by a booster. Despite its limitations, OPV’s role in the sugar cube campaigns remains a testament to its effectiveness in combating a once-devastating disease, offering valuable lessons for future public health initiatives.
Childhood MMR Vaccine: Essential Precautions for Safe Immunization
You may want to see also
Explore related products





![]()
Sabin vs. Salk: OPV (Sabin) was in cubes, unlike the injected inactivated vaccine (Salk)
The sugar cubes that became iconic in the fight against polio contained the Sabin vaccine, a live, attenuated oral polio vaccine (OPV). This method of delivery was revolutionary, transforming vaccination into a simple, even pleasant, experience, especially for children. Unlike the Salk vaccine, which required injection and used an inactivated form of the virus, the Sabin vaccine was administered orally, often on a small, sweet cube. This approach not only increased compliance but also provided a practical solution for mass immunization campaigns. The sugar cube method became a symbol of hope during the mid-20th century, as it promised to eradicate a disease that had paralyzed millions.
From a logistical standpoint, the Sabin vaccine’s oral delivery was a game-changer. The sugar cubes were easy to distribute, required no needles, and could be administered by minimally trained personnel. Each cube contained a precise dose of the vaccine, typically around 0.1 mL of the live, attenuated virus. This simplicity made it ideal for large-scale campaigns, particularly in developing countries where access to medical infrastructure was limited. In contrast, the Salk vaccine’s injection method demanded sterile conditions and trained healthcare workers, making it less feasible for widespread use in remote or resource-poor areas.
The choice between Sabin’s OPV and Salk’s inactivated vaccine (IPV) was not just about delivery method but also about immunity. Sabin’s vaccine induced both humoral and mucosal immunity, providing better protection against the spread of the virus in the community. This was crucial for achieving herd immunity and interrupting polio transmission. However, the live virus in OPV carried a rare but serious risk: vaccine-derived poliovirus (VDPV), which could cause paralysis in immunocompromised individuals or in under-vaccinated populations. Salk’s IPV, while safer in this regard, offered primarily humoral immunity and required multiple doses to be effective.
For parents and caregivers, understanding the differences between these vaccines is essential. The Sabin vaccine, with its sugar cube delivery, was often the first choice for mass campaigns due to its ease of administration and ability to confer gut immunity. However, it was typically given to children over 2 months old, as younger infants might still have maternal antibodies that could interfere with the vaccine’s effectiveness. Salk’s IPV, on the other hand, was often used in combination with OPV in regions where polio remained endemic, providing a dual layer of protection. Today, many countries use a combination of both vaccines to maximize safety and efficacy, though the sugar cube method remains a nostalgic reminder of Sabin’s innovative approach.
In practical terms, the Sabin vaccine’s sugar cube delivery taught us valuable lessons about vaccine accessibility and public acceptance. Its success highlighted the importance of designing vaccines with the end-user in mind, particularly in global health contexts. While the sugar cubes are no longer widely used, their legacy lives on in modern oral vaccines and the ongoing pursuit of painless, convenient immunization methods. For those interested in historical vaccination campaigns, the Sabin vaccine’s story underscores the power of innovation in overcoming public health challenges.
Navigating Vaccine Exemption Applications: A Step-by-Step Guide for Eligibility
You may want to see also
Explore related products






![]()
Mass Immunization: Sugar cubes made OPV administration easy for large-scale campaigns in the 1960s
The sugar cubes of the 1960s were not just a sweet treat but a revolutionary tool in the fight against polio. These unassuming cubes contained the Oral Polio Vaccine (OPV), a live-attenuated vaccine that could prevent the debilitating disease. This innovative delivery method played a pivotal role in mass immunization campaigns, particularly in the United States, where it became a symbol of public health success.
A Sweet Solution for Mass Immunization
In the 1960s, the OPV was administered to millions of children through a simple sugar cube, making it one of the most accessible and widely accepted vaccines in history. The vaccine, developed by Albert Sabin, was a game-changer due to its ease of administration and effectiveness. Unlike injections, which could be painful and required trained medical personnel, the sugar cube method allowed for rapid distribution in schools, community centers, and even door-to-door campaigns. This approach was particularly crucial for reaching large populations quickly, a key strategy in eradicating polio.
Practical Implementation and Dosage
The process was straightforward: each sugar cube was impregnated with a specific dose of the OPV, typically 0.1 mL, containing Type 1, 2, and 3 polioviruses. Children, usually between the ages of 2 and 5, would receive one cube, placed on their tongue to dissolve. This method ensured accurate dosing and was far less intimidating than a needle, making it ideal for young children. The vaccine's stability at room temperature further facilitated its distribution, even in areas with limited refrigeration.
Impact and Legacy
The sugar cube campaigns were a logistical triumph, immunizing millions within a short period. For instance, in 1962, over 3 million children in New York City received the vaccine in a single day, a remarkable feat of organization. This approach not only reduced the incidence of polio but also demonstrated the power of creative solutions in public health. The success of these campaigns contributed to a significant decline in polio cases, paving the way for global eradication efforts.
Lessons for Modern Immunization Strategies
The sugar cube OPV administration offers valuable insights for contemporary vaccination programs. Its success highlights the importance of considering cultural acceptance, ease of delivery, and community engagement. Modern vaccines could benefit from similar innovative delivery systems, especially in regions with limited healthcare infrastructure. By learning from this historical example, public health officials can design more effective and accessible immunization strategies, ensuring vaccines reach those who need them most.
In summary, the sugar cubes containing OPV were a brilliant solution for mass immunization, combining medical science with practical innovation. This approach not only saved countless lives but also set a precedent for creative vaccine distribution, leaving a lasting impact on global health initiatives.
US Vaccines: Made in China?
You may want to see also
Explore related products




![]()
Stability in Cubes: The vaccine remained stable in sugar cubes, ensuring effective delivery
The polio vaccine, specifically the oral Sabin vaccine, was the primary vaccine delivered via sugar cubes during the mid-20th century. This method was chosen not only for its ease of administration but also because the sugar helped stabilize the live attenuated virus, ensuring it remained effective from production to consumption. The vaccine’s stability in sugar cubes was critical, as it allowed for mass immunization campaigns to reach millions of children globally, particularly in areas with limited access to refrigeration or medical infrastructure.
One of the key factors in the vaccine’s stability was the protective environment provided by the sugar cube itself. The sucrose in the cube acted as a desiccant, reducing moisture and preventing the virus from degrading. Additionally, the sugar’s crystalline structure shielded the vaccine from temperature fluctuations, which could otherwise render it ineffective. For instance, the Sabin vaccine, when embedded in sugar cubes, retained its potency for up to 48 hours at room temperature, making it ideal for door-to-door distribution campaigns. This stability was particularly crucial in developing countries, where maintaining a cold chain was often impractical.
Administering the vaccine via sugar cubes also simplified dosage and delivery. Each cube was standardized to contain one dose of the vaccine, typically around 0.1 mL of the live attenuated virus. This eliminated the need for trained medical personnel to measure and administer the vaccine, as the sugar cube itself served as both the delivery mechanism and the preservative. Parents were instructed to give the cube to their children, who would consume it like a treat, ensuring high compliance rates among children aged 6 months to 5 years, the primary target group for polio vaccination.
Comparatively, other vaccine delivery methods at the time, such as injections, faced challenges in stability and administration. Injectable vaccines required refrigeration and trained personnel, limiting their reach in rural or resource-constrained areas. The sugar cube method, however, bypassed these hurdles, enabling mass vaccination drives that drastically reduced polio cases worldwide. For example, during the 1960s, the World Health Organization (WHO) distributed Sabin vaccine-infused sugar cubes to over 100 million children annually, contributing to a 99% reduction in polio cases globally by the late 20th century.
To replicate this method today for other vaccines, several practical considerations must be taken into account. First, the vaccine must be compatible with the sugar matrix, as not all vaccines can withstand the desiccating effects of sucrose. Second, the sugar cubes must be produced under sterile conditions to prevent contamination. Finally, public education campaigns are essential to ensure proper handling and consumption. While the sugar cube method may not be universally applicable, its success with the polio vaccine underscores the importance of innovative delivery systems in achieving global health goals.
Add Your Vaccine Passport to iPhone Wallet: A Simple Guide
You may want to see also
Explore related products






![]()
Global Eradication: Sugar cube vaccines played a key role in reducing polio cases worldwide
The sugar cubes that became a symbol of hope in the fight against polio contained the Sabin oral polio vaccine (OPV), a live-attenuated vaccine developed by Dr. Albert Sabin in the late 1950s. Unlike the injectable inactivated polio vaccine (IPV) created by Dr. Jonas Salk, OPV was administered orally, making it easier to distribute on a global scale. This innovation was pivotal in the World Health Assembly’s 1988 resolution to eradicate polio worldwide. The sugar cubes, each infused with a single dose of the vaccine, were not only palatable to children but also eliminated the need for medical expertise in administration, enabling mass immunization campaigns in remote and resource-limited areas.
One of the most striking examples of the sugar cube vaccine’s impact was the 1961–1962 campaign in the United States, where over 20 million children received the vaccine in school-based programs. The simplicity of distribution—children were given a sugar cube to eat, no needles required—led to rapid uptake. Globally, this approach was replicated in countries like India, Brazil, and Egypt, where door-to-door campaigns and community health drives reached millions. The vaccine’s efficacy was remarkable: a single dose provided 50% immunity, while three doses, spaced 4–6 weeks apart, achieved up to 95% protection in children under 5, the most vulnerable age group.
The logistical advantages of the sugar cube vaccine cannot be overstated. In regions with limited healthcare infrastructure, the vaccine’s stability at room temperature for short periods and its ease of transport made it a game-changer. For instance, in rural Africa and Southeast Asia, where refrigeration was scarce, health workers could carry thousands of doses in simple containers, ensuring accessibility. However, the sugar cube method was eventually phased out in favor of liquid OPV drops due to cost-effectiveness and ease of production. Despite this, the sugar cube campaigns laid the groundwork for modern mass immunization strategies, demonstrating that creative delivery methods could overcome barriers to global health initiatives.
Critics initially questioned the vaccine’s safety and efficacy, particularly in regions with poor sanitation, where the live virus could, in rare cases, revert to a virulent form. Yet, the benefits far outweighed the risks. By 1994, the Americas were declared polio-free, and global cases plummeted from 350,000 in 1988 to fewer than 1,000 by 2000. The sugar cube vaccine’s role in this achievement underscores the power of innovation in public health. Today, as we edge closer to complete eradication, the lessons from this campaign remain relevant: simplicity, accessibility, and community engagement are key to tackling global health challenges.
For those involved in modern immunization efforts, the sugar cube vaccine offers a blueprint for success. Practical tips include leveraging local leaders to build trust, using culturally appropriate delivery methods, and ensuring consistent follow-up doses. While the sugar cube itself is no longer in use, its legacy lives on in the oral vaccine drops that continue to protect millions. The story of the sugar cube vaccine is not just a historical footnote but a testament to human ingenuity and the relentless pursuit of a polio-free world.
Kissinger's Vaccination Agenda: Herd Acceptance
You may want to see also
Frequently asked questions
The sugar cubes contained the oral polio vaccine (OPV), developed by Dr. Albert Sabin.
The sugar cubes were used as a palatable and convenient way to administer the oral polio vaccine, making it easier for children to take.
Sugar cubes were widely used in the 1960s during mass vaccination campaigns, particularly in the United States, to eradicate polio.
No, the use of sugar cubes for the polio vaccine has been discontinued. Today, OPV is typically administered as liquid drops directly into the mouth.


![Eighty-three Years a Servant, or, The Life of Rev. Alvah Sabin [microform]](https://m.media-amazon.com/images/I/51EiGEIbt2L._AC_UL320_.jpg)