Poliomyelitis, commonly known as polio, is a highly contagious viral disease that can lead to paralysis and even death, particularly in young children. The development of vaccines has been pivotal in the global effort to eradicate this debilitating illness. The vaccine for poliomyelitis, introduced in the 1950s, comes in two primary forms: the inactivated poliovirus vaccine (IPV), which is administered through injection, and the oral poliovirus vaccine (OPV), delivered as drops. These vaccines have significantly reduced the incidence of polio worldwide, with many countries now declared polio-free. The success of vaccination campaigns underscores the importance of widespread immunization in preventing the spread of this once-devastating disease.
Explore related products






What You'll Learn
- Vaccine Types: Inactivated Polio Vaccine (IPV) and Oral Polio Vaccine (OPV) are the two main types
- Effectiveness: Both vaccines provide high immunity, preventing poliovirus infection and paralysis effectively
- Administration: IPV is injected, while OPV is given orally, making it easier to distribute
- Global Eradication: Vaccination campaigns have reduced polio cases by over 99% worldwide since 1988
- Side Effects: Mild side effects include soreness at the injection site or mild fever, rarely serious
![]()
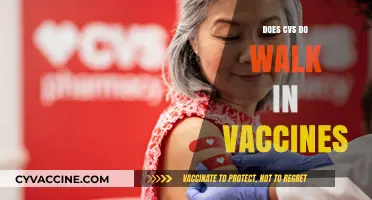
Vaccine Types: Inactivated Polio Vaccine (IPV) and Oral Polio Vaccine (OPV) are the two main types
Poliomyelitis, a once-feared disease causing paralysis and even death, has been largely eradicated thanks to effective vaccination programs. At the heart of this success are two primary vaccine types: the Inactivated Polio Vaccine (IPV) and the Oral Polio Vaccine (OPV). Each has distinct characteristics, administration methods, and roles in global polio prevention. Understanding these differences is crucial for healthcare providers, policymakers, and parents alike.
Analytical Perspective:
IPV, introduced in 1955, is an injectable vaccine containing inactivated (killed) poliovirus. It stimulates the body to produce antibodies against all three poliovirus types (1, 2, and 3) without introducing live virus. This makes IPV safer for individuals with weakened immune systems, as it cannot cause vaccine-associated paralytic polio (VAPP), a rare but serious risk associated with OPV. However, IPV primarily induces humoral immunity (blood-based antibodies), offering limited protection against viral transmission in the gut. This means vaccinated individuals can still carry and spread the virus, though they are protected from paralysis. IPV is typically administered in multiple doses, starting at 2 months of age, with boosters recommended for long-term immunity.
Instructive Approach:
OPV, developed by Albert Sabin in the 1960s, is an oral vaccine containing weakened (attenuated) live poliovirus. Its key advantage is its ability to induce both humoral and mucosal immunity, effectively blocking viral replication in the gut and preventing transmission. This makes OPV a powerful tool for interrupting polio outbreaks in communities. However, the live virus in OPV can, in rare cases (1 in 2.7 million doses), revert to a virulent form and cause VAPP. For this reason, OPV is being phased out in countries where polio has been eliminated, replaced by IPV to eliminate the risk of vaccine-derived poliovirus (VDPV). OPV is administered as drops, making it easier to deliver in mass campaigns, especially in low-resource settings.
Comparative Analysis:
The choice between IPV and OPV depends on the epidemiological context. In polio-endemic regions, OPV remains the vaccine of choice due to its ability to halt transmission and provide herd immunity. However, in polio-free countries, IPV is preferred to eliminate the risk of VAPP and VDPV. A hybrid approach, using both vaccines, has been adopted in some regions to maximize immunity while minimizing risks. For instance, the World Health Organization recommends a "sequential schedule" where OPV is given first to induce mucosal immunity, followed by IPV to boost antibody levels and ensure long-term protection.
Practical Tips:
For parents and caregivers, understanding the vaccine schedule is essential. In many countries, infants receive a combination of IPV and OPV doses, tailored to local polio risk. For example, in the U.S., the CDC recommends four doses of IPV at 2 months, 4 months, 6–18 months, and 4–6 years. In polio-endemic areas, OPV may be given at birth, followed by multiple doses in the first year. Travelers to polio-affected regions should ensure they are up to date on their polio vaccines and may require a booster dose. Always consult healthcare providers for personalized advice, especially for individuals with immunodeficiencies or specific health conditions.
Persuasive Takeaway:
The IPV and OPV vaccines are not just medical tools but symbols of humanity’s triumph over a devastating disease. While their differences in administration, immunity, and risk profiles require careful consideration, their combined use has brought polio to the brink of eradication. Choosing the right vaccine is not just a clinical decision but a strategic one, balancing individual safety with community protection. As we approach a polio-free world, staying informed and vaccinated remains our best defense against this preventable disease.
Vaccination: Weighing Lifesaving Benefits Against Potential Risks and Concerns
You may want to see also
Explore related products






![]()
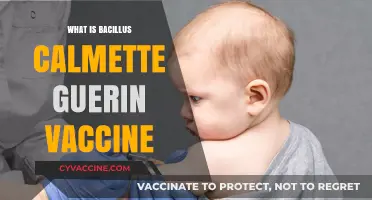
Effectiveness: Both vaccines provide high immunity, preventing poliovirus infection and paralysis effectively
The two primary vaccines for poliomyelitis—the inactivated poliovirus vaccine (IPV) and the oral poliovirus vaccine (OPV)—are remarkably effective in preventing both poliovirus infection and the devastating paralysis it can cause. Clinical trials and real-world data consistently show that IPV, administered through injection, provides over 90% immunity after two doses and nearly 100% protection after three doses. OPV, delivered orally, is equally potent, inducing robust intestinal immunity that blocks viral replication and transmission. This dual-pronged effectiveness has been pivotal in reducing global polio cases by 99% since 1988, highlighting the vaccines' role in near-eradication efforts.
For optimal protection, the World Health Organization (WHO) recommends a tailored vaccination schedule based on age and risk factors. Infants typically receive their first dose of IPV at 2 months, followed by additional doses at 4 months and 6–18 months, ensuring long-term immunity. In regions with active polio transmission, OPV is often used in mass vaccination campaigns, as its ease of administration and ability to confer mucosal immunity make it ideal for rapid community protection. However, due to rare cases of vaccine-derived poliovirus, IPV is increasingly favored in polio-free countries, offering a safer alternative without compromising efficacy.
A critical aspect of these vaccines' effectiveness lies in their ability to prevent paralytic polio, the most severe manifestation of the disease. Studies show that even in individuals who contract the virus after vaccination, the risk of paralysis is reduced by over 70%. This underscores the vaccines' role not only in preventing infection but also in mitigating the disease's most debilitating effects. For travelers to polio-endemic areas, a booster dose of IPV is recommended, ensuring continued protection against imported cases and maintaining global eradication progress.
Despite their proven efficacy, maximizing the vaccines' impact requires addressing logistical and behavioral challenges. Cold chain maintenance is essential for IPV, as it must be stored between 2°C and 8°C to remain viable. OPV, while more heat-stable, requires careful handling to avoid contamination. Public health campaigns emphasizing the importance of completing the full vaccine series are equally vital, as partial immunity can leave individuals vulnerable. By combining scientific rigor with practical strategies, these vaccines continue to serve as a cornerstone of polio prevention, bringing the world closer to a polio-free future.
Parvo Vaccine Safety: Handwashing After Administration – Essential or Optional?
You may want to see also
Explore related products






![]()
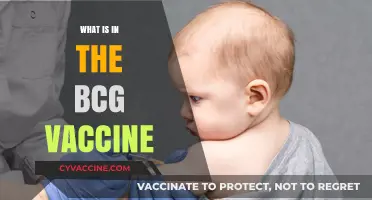
Administration: IPV is injected, while OPV is given orally, making it easier to distribute
The route of administration is a critical factor in the delivery of poliomyelitis vaccines, with inactivated poliovirus vaccine (IPV) and oral poliovirus vaccine (OPV) offering distinct advantages and challenges. IPV, administered through injection, typically requires a trained healthcare professional to deliver the vaccine intramuscularly or subcutaneously, often in the deltoid muscle for adults or the vastus lateralis muscle for infants and young children. The standard dosage for IPV is 0.5 mL, with a recommended schedule of 4 doses at 2, 4, 6-18 months, and 4-6 years of age. This method ensures a high level of safety, as the inactivated virus cannot revert to a virulent form, making it suitable for individuals with compromised immune systems.
In contrast, OPV is administered orally, usually in the form of 2 drops (approximately 0.1 mL) for each dose. This route of administration mimics the natural infection pathway, inducing both humoral and mucosal immunity. The simplicity of oral delivery makes OPV particularly advantageous in mass vaccination campaigns, especially in low-resource settings where access to trained healthcare personnel may be limited. For instance, during the Global Polio Eradication Initiative, OPV was administered by volunteers and community health workers, facilitating rapid and widespread coverage. However, it is essential to note that OPV contains attenuated but live virus, which, in rare cases, can revert to a virulent form, causing vaccine-associated paralytic poliomyelitis (VAPP) or circulating vaccine-derived polioviruses (cVDPVs).
A comparative analysis highlights the trade-offs between IPV and OPV administration. While IPV’s injectable form ensures safety and individual protection, its distribution is logistically more demanding, requiring sterile equipment and skilled personnel. OPV, on the other hand, offers ease of administration and the added benefit of reducing wild poliovirus transmission through mucosal immunity. However, the risk of vaccine-derived polioviruses necessitates careful consideration of its use, particularly in regions with high vaccination coverage and low poliovirus circulation. In such areas, a sequential or mixed IPV-OPV schedule is often recommended to balance the benefits of both vaccines.
From a practical standpoint, the choice of vaccine administration depends on the epidemiological context, healthcare infrastructure, and target population. In regions with ongoing poliovirus transmission, OPV remains the vaccine of choice due to its ability to interrupt viral spread. In polio-free countries, IPV is preferred for routine immunization, often supplemented with OPV during outbreak responses. For travelers to polio-endemic areas, the CDC recommends a single lifetime IPV booster dose for adults who completed their primary series but were not previously vaccinated as adults. This tailored approach underscores the importance of considering administration routes in the broader strategy to eradicate poliomyelitis.
Ultimately, the distinct administration methods of IPV and OPV exemplify the principle that vaccine delivery is as crucial as the vaccine itself. While IPV’s injectable form prioritizes safety and individual protection, OPV’s oral administration excels in accessibility and herd immunity. Understanding these differences empowers healthcare providers, policymakers, and communities to make informed decisions, ensuring that the right vaccine reaches the right population at the right time. As the world edges closer to polio eradication, the strategic use of both administration routes will remain pivotal in sustaining progress and addressing emerging challenges.
Antibodies: How They Attack Pathogens
You may want to see also
Explore related products






![]()
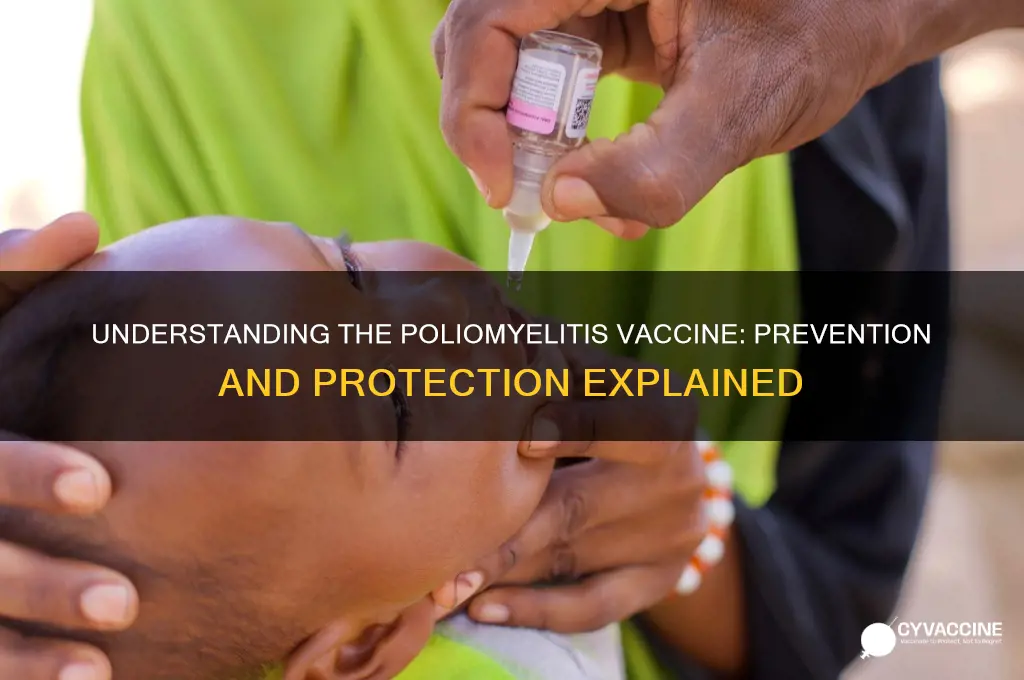
Global Eradication: Vaccination campaigns have reduced polio cases by over 99% worldwide since 1988
The success of global vaccination campaigns against poliomyelitis is nothing short of remarkable. Since 1988, concerted efforts led by organizations like the World Health Organization (WHO), UNICEF, and Rotary International have reduced polio cases by over 99%, from an estimated 350,000 cases annually to fewer than 100 in recent years. This achievement underscores the power of coordinated global health initiatives and the effectiveness of the polio vaccine. The two primary vaccines—the inactivated poliovirus vaccine (IPV) and the oral poliovirus vaccine (OPV)—have been instrumental in this progress, each playing distinct roles in different phases of eradication efforts.
Analytically, the decline in polio cases can be attributed to strategic vaccination drives targeting high-risk areas, particularly in low-income countries. The OPV, administered orally in drops, has been the backbone of mass immunization campaigns due to its ease of delivery and ability to induce intestinal immunity, which prevents viral shedding. However, its attenuated live virus can, in rare cases, revert to a virulent form, causing vaccine-derived poliovirus (VDPV). To mitigate this risk, IPV, an injectable vaccine containing inactivated virus, is increasingly used in regions where wild polio has been eliminated. This dual-vaccine strategy ensures both broad coverage and safety, adapting to the evolving needs of the eradication campaign.
Instructively, vaccination schedules vary by region but typically begin in infancy. The WHO recommends a primary series of at least three OPV doses, starting at 6 weeks of age, followed by additional doses to ensure long-term immunity. In countries transitioning to IPV, a combination of IPV and OPV is often used, with IPV administered at 2, 4, and 6–18 months, followed by OPV boosters. For travelers to polio-endemic areas, the CDC advises adults who completed their childhood vaccinations to receive a single lifetime IPV booster. Adhering to these schedules is critical, as even small gaps in immunity can allow the virus to circulate and mutate.
Persuasively, the near-eradication of polio highlights the importance of sustained global commitment. Despite challenges like vaccine hesitancy, inaccessible populations, and political instability, the campaign has demonstrated that eradication is achievable with sufficient resources and collaboration. However, complacency remains a threat. As long as a single child remains infected, the virus can resurge, undoing decades of progress. Continued funding, surveillance, and community engagement are essential to cross the finish line and ensure polio joins smallpox as a disease of the past.
Descriptively, the impact of polio eradication extends beyond health metrics. In countries once burdened by the disease, children who would have been paralyzed or died now walk, play, and contribute to their communities. Economically, eradication efforts have saved billions in healthcare costs and productivity losses. The infrastructure built for polio campaigns—cold chains, health worker training, and surveillance systems—has strengthened overall health systems, benefiting the fight against other diseases like measles and COVID-19. This legacy underscores the transformative potential of global health initiatives when driven by collective will and scientific innovation.
Flying in India: Is COVID-19 Vaccination Mandatory for Air Travel?
You may want to see also
Explore related products






![]()
Side Effects: Mild side effects include soreness at the injection site or mild fever, rarely serious
The poliomyelitis vaccine, a cornerstone of global health, has virtually eradicated this once-feared disease. Yet, like any medical intervention, it carries potential side effects. Understanding these reactions is crucial for informed decision-making and peace of mind.
Most individuals experience only mild, transient discomfort after receiving the polio vaccine. These common side effects typically manifest within 24 hours of vaccination and resolve within a few days. Soreness, redness, or swelling at the injection site are the most frequent complaints, akin to the tenderness one might feel after a flu shot. A mild fever, usually below 101°F (38.3°C), may also occur, often accompanied by fatigue or fussiness, particularly in young children. These reactions are a normal part of the body's immune response, signaling the vaccine is working to build protection against poliovirus.
It's important to differentiate these mild reactions from more serious adverse events, which are extremely rare. Severe allergic reactions to the polio vaccine are estimated to occur in less than one in a million doses. Symptoms of a severe reaction include difficulty breathing, swelling of the face and throat, rapid heartbeat, dizziness, and a severe skin rash. If any of these symptoms appear, immediate medical attention is crucial.
It's worth noting that the type of polio vaccine administered can influence the likelihood of side effects. The inactivated poliovirus vaccine (IPV), given as an injection, is the primary vaccine used in most countries today. IPV is known for its excellent safety profile, with serious side effects being exceptionally rare. The oral poliovirus vaccine (OPV), while highly effective, carries a minuscule risk of vaccine-associated paralytic polio (VAPP), occurring in approximately 1 in 2.7 million doses. This risk is why OPV is no longer routinely used in countries where polio has been eliminated.
For parents, understanding these potential side effects is essential for managing expectations and providing comfort to their children. Applying a cool, damp cloth to the injection site can alleviate soreness. Over-the-counter pain relievers like acetaminophen can help reduce fever and discomfort, but aspirin should be avoided in children due to the risk of Reye's syndrome. Ensuring adequate hydration and rest is also beneficial. By recognizing the typical mild reactions and knowing when to seek medical attention, individuals can approach polio vaccination with confidence, knowing the benefits far outweigh the minimal risks.
Hepatitis B Vaccine: Understanding the Injection Schedule and Doses
You may want to see also
Frequently asked questions
The vaccine for poliomyelitis (polio) is a medical product designed to protect against the poliovirus, which causes polio. There are two types of polio vaccines: the inactivated poliovirus vaccine (IPV) and the oral poliovirus vaccine (OPV).
The polio vaccine works by stimulating the body’s immune system to produce antibodies against the poliovirus. IPV, given as an injection, contains inactivated (killed) virus, while OPV, administered orally, contains weakened (attenuated) live virus. Both vaccines prevent the virus from causing paralysis and stop its spread.
The polio vaccine is recommended for all children as part of routine immunization schedules. Adults who are unvaccinated, traveling to polio-endemic areas, or at increased risk of exposure should also receive the vaccine. Pregnant women and immunocompromised individuals should consult a healthcare provider for specific guidance.
Yes, the polio vaccine is safe and highly effective. Common side effects are mild, such as soreness at the injection site for IPV or mild fever for OPV. Serious side effects are extremely rare. The vaccine has successfully eradicated polio in most countries, making it a cornerstone of global public health efforts.