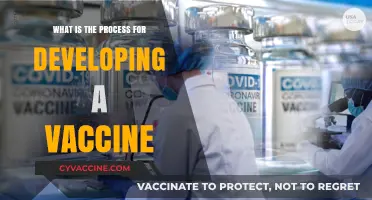
Administering a vaccine requires strict adherence to established protocols to ensure safety, efficacy, and patient well-being. The proper procedure begins with verifying the patient’s identity, medical history, and consent, followed by confirming the correct vaccine type, dosage, and expiration date. The vaccine should be stored and handled according to manufacturer guidelines, and the appropriate injection site (e.g., deltoid muscle for most adults) must be cleaned with an antiseptic. Using a sterile needle and syringe, the vaccine is administered at the correct angle and depth, followed by disposal of sharps in a designated container. Post-vaccination, the patient is monitored for immediate adverse reactions, and documentation of the vaccine details is recorded in the patient’s medical record and immunization registry. Adhering to these steps minimizes risks and maximizes the vaccine’s protective benefits.
| Characteristics | Values |
|---|---|
| Vaccine Selection | Choose the appropriate vaccine based on age, health status, and indication. |
| Storage Requirements | Store vaccines at recommended temperatures (e.g., 2-8°C for most vaccines). |
| Pre-Administration Check | Verify patient identity, consent, and medical history (e.g., allergies). |
| Vaccine Preparation | Follow manufacturer instructions for reconstitution (if required). |
| Injection Site | Administer intramuscularly (e.g., deltoid muscle) or subcutaneously. |
| Needle Size | Use appropriate needle length (e.g., 1-1.5 inches for adults). |
| Injection Technique | Insert needle at a 90-degree angle for intramuscular injections. |
| Dosage | Administer the correct dose as per age and vaccine guidelines. |
| Post-Injection Care | Apply gentle pressure if bleeding occurs; provide a record of vaccination. |
| Observation Period | Observe the patient for 15-30 minutes post-vaccination for adverse reactions. |
| Documentation | Record vaccine type, date, lot number, and administration details. |
| Adverse Event Reporting | Report severe reactions to relevant health authorities (e.g., VAERS). |
| Personal Protective Equipment (PPE) | Use gloves and dispose of sharps safely. |
| Waste Management | Dispose of vaccine vials and needles in biohazard containers. |
| Patient Education | Inform about potential side effects and follow-up requirements. |
| Storage of Records | Maintain vaccination records for future reference. |
Explore related products

$5.36 $19.95





What You'll Learn
- Pre-vaccination Screening: Check medical history, allergies, and current health status before administering the vaccine
- Vaccine Storage: Ensure vaccines are stored at correct temperatures to maintain potency and safety
- Site Preparation: Clean injection site with alcohol swab to prevent infection and ensure sterility
- Injection Technique: Use proper needle size, angle, and depth for intramuscular or subcutaneous administration
- Post-vaccination Care: Monitor for adverse reactions, provide aftercare instructions, and schedule follow-up if needed
![]()
Pre-vaccination Screening: Check medical history, allergies, and current health status before administering the vaccine
Before administering any vaccine, a thorough pre-vaccination screening is essential to ensure safety and efficacy. This process involves a detailed review of the individual’s medical history, known allergies, and current health status. For instance, a history of severe allergic reactions (anaphylaxis) to a previous vaccine or its components, such as eggs or gelatin, is a critical contraindication for certain vaccines. Similarly, individuals with compromised immune systems, whether due to conditions like HIV or medications like corticosteroids, may require adjusted dosing or alternative vaccine types. This screening step is not merely bureaucratic—it’s a safeguard that prevents adverse reactions and ensures the vaccine’s intended benefits are realized.
The screening process begins with a structured questionnaire or interview, often conducted by a healthcare provider. Key questions include inquiries about previous vaccine reactions, chronic illnesses, and current medications. For example, a patient on high-dose steroids might need to delay vaccination until their immune system is less suppressed. Age-specific considerations are also vital: infants under 6 months are not eligible for most vaccines due to their underdeveloped immune systems, while older adults may require higher dosages or adjuvanted formulations for improved immunity. Practical tips for providers include verifying the patient’s identity to avoid errors and using standardized forms to ensure no critical information is overlooked.
Comparatively, pre-vaccination screening differs from routine medical check-ups in its focus on vaccine-specific risks. While a general health assessment evaluates overall well-being, this screening hones in on factors that could interact negatively with the vaccine. For instance, a mild fever might warrant postponing a live-attenuated vaccine like MMR, as the body’s immune response could be compromised. In contrast, an inactivated vaccine like the flu shot may still be administered with caution. This targeted approach underscores the importance of tailoring the vaccination process to the individual, rather than applying a one-size-fits-all method.
Persuasively, skipping pre-vaccination screening can lead to preventable complications, ranging from mild discomfort to life-threatening reactions. Consider the case of a patient with an undiagnosed egg allergy receiving the influenza vaccine, which is often cultured in egg proteins. Without screening, this could result in anaphylaxis, a scenario easily avoided with proper assessment. Furthermore, documenting this screening process provides legal protection for healthcare providers and builds trust with patients, who feel assured that their health is prioritized. In a world where vaccine hesitancy persists, this step is not just clinical—it’s a cornerstone of public health communication.
In conclusion, pre-vaccination screening is a critical yet often underemphasized step in vaccine administration. By systematically evaluating medical history, allergies, and current health status, healthcare providers can minimize risks and maximize benefits. This process requires attention to detail, age-specific considerations, and a proactive approach to patient safety. As vaccines continue to evolve, so too must the rigor of pre-vaccination screening, ensuring that every dose administered is as safe and effective as possible.
Vaccines and Infant Survival: A Decline in Mortality Rates?
You may want to see also
Explore related products






![]()
Vaccine Storage: Ensure vaccines are stored at correct temperatures to maintain potency and safety
Vaccines are delicate biological products, and their efficacy hinges on proper storage conditions. Temperature deviations, even minor ones, can compromise potency, rendering vaccines ineffective or, worse, unsafe. This vulnerability underscores the critical importance of adhering to strict storage protocols throughout the supply chain, from manufacturer to administration site.
Vaccines are categorized into three main temperature ranges: frozen (typically -58°F to 5°F or -50°C to -15°C), refrigerated (35°F to 46°F or 2°C to 8°C), and room temperature (controlled, short-term exposure). Each vaccine has a specific storage requirement, meticulously outlined by the manufacturer and health authorities. For instance, the measles, mumps, and rubella (MMR) vaccine requires refrigeration, while the smallpox vaccine demands frozen storage. Deviations from these ranges, even for brief periods, can lead to irreversible damage. A study published in the *Journal of Infectious Diseases* found that exposure to temperatures above 8°C for just 24 hours significantly reduced the potency of the influenza vaccine, highlighting the narrow margin for error.
Maintaining these precise temperatures requires specialized equipment and vigilant monitoring. Refrigerators and freezers used for vaccine storage must be purpose-built, with features like digital temperature displays, alarms for temperature excursions, and backup power supplies. Regular calibration and maintenance are essential to ensure accuracy. Additionally, vaccines should be stored in the appropriate compartments within these units: refrigerated vaccines on the middle shelves to avoid temperature fluctuations near the door, and frozen vaccines in the center of the freezer, away from the walls.
Human error poses a significant risk to vaccine storage integrity. Common mistakes include overloading refrigerators, blocking vents, and failing to monitor temperatures regularly. To mitigate these risks, healthcare facilities should implement robust standard operating procedures (SOPs). These SOPs should include daily temperature checks, documented by trained staff, and immediate action plans for addressing temperature deviations. For example, if a refrigerator’s temperature rises above 8°C, staff should relocate vaccines to a backup unit, notify the vaccine coordinator, and investigate the cause of the malfunction.
The consequences of improper storage are far-reaching. Administering a compromised vaccine not only fails to confer immunity but can also erode public trust in vaccination programs. In 2019, a storage error in a North Carolina health department led to the wastage of over 1,000 doses of the HPV vaccine, costing thousands of dollars and delaying vaccinations for at-risk adolescents. Such incidents underscore the need for continuous training and accountability in vaccine management.
In conclusion, vaccine storage is a cornerstone of immunization programs, demanding precision, vigilance, and adherence to protocols. By understanding the unique requirements of each vaccine, investing in appropriate equipment, and fostering a culture of accountability, healthcare providers can ensure that every dose administered fulfills its life-saving potential.
Vaccine Mandates for Healthcare Workers in New York
You may want to see also
Explore related products

$49.99 $50





![]()
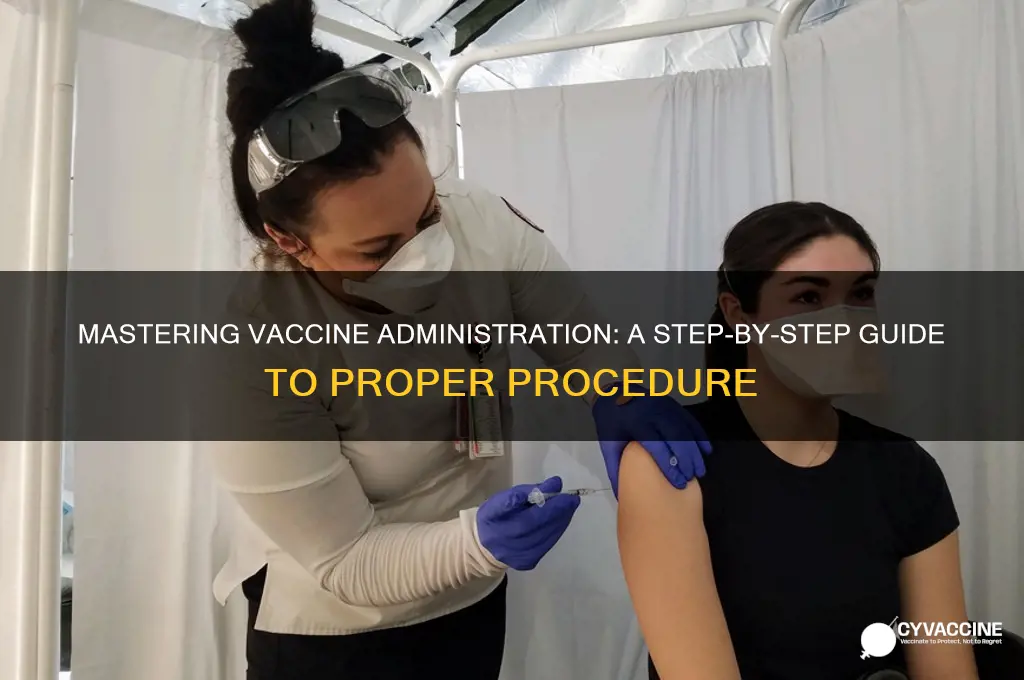
Site Preparation: Clean injection site with alcohol swab to prevent infection and ensure sterility
Before administering a vaccine, ensuring the injection site is clean and sterile is a critical step that cannot be overlooked. The skin, though a formidable barrier, is not impermeable to pathogens. Microorganisms like bacteria and viruses can enter the body through even the smallest breach, potentially leading to localized or systemic infections. An alcohol swab, typically containing 70% isopropyl alcohol, is the gold standard for this purpose. This concentration is optimal because it effectively denatures proteins in microorganisms, disrupting their cell membranes and rendering them harmless. Higher concentrations of alcohol can be less effective due to the rapid evaporation rate, which may leave behind residual pathogens.
The process of cleaning the injection site is straightforward but requires precision. Begin by removing the alcohol swab from its sterile packaging, ensuring the seal is intact to prevent contamination. Gently but firmly wipe the intended injection site—typically the deltoid muscle for adults or the vastus lateralis muscle in infants and young children—in a circular motion. The motion should be outward, starting from the center of the site and moving toward the periphery. This technique minimizes the risk of pushing pathogens deeper into the skin. Allow the area to air dry for approximately 30 seconds; using a fan or rubbing the area can reintroduce contaminants. For individuals with sensitive skin or allergies, healthcare providers should verify the absence of adverse reactions to alcohol-based products and consider alternative antiseptics like povidone-iodine if necessary.
Comparing alcohol swabs to other antiseptic methods highlights their efficiency and practicality. While povidone-iodine is effective and may be preferred for those with alcohol sensitivities, it requires a longer drying time and can stain clothing or skin. Chlorhexidine is another alternative, often used in surgical settings, but its higher cost and potential for skin irritation make it less ideal for routine vaccinations. Alcohol swabs, on the other hand, are cost-effective, fast-acting, and widely available, making them the preferred choice for most vaccination protocols. Their ease of use also ensures compliance, even in high-pressure or resource-limited settings.
From a practical standpoint, proper site preparation is not just about preventing infection—it’s about building trust and ensuring patient comfort. A clean injection site reduces the risk of post-vaccination complications such as abscesses, cellulitis, or localized reactions, which can erode confidence in vaccination programs. For pediatric populations, where fear and anxiety are common, a quick and painless site preparation process can significantly improve the overall experience. Parents and caregivers are more likely to return for future vaccinations if they perceive the procedure as safe and well-executed. This step, though seemingly minor, is a cornerstone of effective vaccine delivery and public health.
In conclusion, the use of an alcohol swab to clean the injection site is a simple yet indispensable part of vaccine administration. It combines scientific rigor with practical efficiency, ensuring sterility while minimizing discomfort and risk. Healthcare providers must adhere to this step meticulously, as it directly impacts both individual outcomes and the broader success of immunization efforts. By prioritizing site preparation, we not only protect against infection but also reinforce the integrity of vaccination as a life-saving intervention.
Air Travel and Masks: Vaccinated, but Masked?
You may want to see also
Explore related products






![]()
Injection Technique: Use proper needle size, angle, and depth for intramuscular or subcutaneous administration
The choice of needle size, angle, and depth is critical for effective vaccine delivery, ensuring the antigen reaches the intended tissue while minimizing discomfort and adverse reactions. For intramuscular (IM) injections, the needle length should correspond to the patient's age and body mass to penetrate the muscle tissue adequately. Adults and older children typically require a 1- to 1.5-inch needle, while infants and younger children may need a 5/8-inch needle. Subcutaneous (SC) injections, on the other hand, use shorter needles—usually 5/8 inch or less—to deposit the vaccine into the fatty tissue just beneath the skin. Selecting the correct needle gauge is equally important; a 22- to 25-gauge needle is standard for most vaccinations, balancing ease of injection with patient comfort.
The injection angle varies depending on the administration route. For IM injections, a 90-degree angle is optimal, ensuring the needle penetrates the muscle tissue fully. This is particularly important for vaccines like the influenza or COVID-19 vaccines, which are commonly administered IM. For SC injections, a 45-degree angle is recommended to ensure the vaccine is delivered into the subcutaneous layer without entering the muscle. Proper technique here is crucial for vaccines such as the measles, mumps, and rubella (MMR) vaccine, which is administered SC. Incorrect angles can result in incomplete delivery or unintended tissue penetration, reducing vaccine efficacy or causing pain.
Depth of injection is another key factor. IM injections must reach the muscle tissue, which requires full needle insertion for adults and older children. For infants, the vastus lateralis muscle is the preferred site, and the needle should be inserted to its full length to ensure intramuscular delivery. SC injections, however, require only a partial insertion of the needle, typically just under the skin’s surface. Over-insertion can lead to intramuscular delivery, while under-insertion may result in vaccine leakage. For example, the hepatitis B vaccine, administered IM, requires precise depth to ensure the antigen reaches the muscle, while the varicella vaccine, given SC, must stay within the subcutaneous layer.
Practical tips can enhance injection technique and patient experience. For IM injections, stabilize the needle with one hand while using the other to gently stretch the skin, reducing movement and discomfort. For SC injections, pinching the skin creates a tent-like fold, ensuring the needle stays within the subcutaneous layer. Always aspirate slightly after needle insertion for IM injections to check for blood, which indicates accidental intravenous entry. If blood is present, withdraw the needle and reinsert it at a different site. Finally, after injection, apply gentle pressure with a dry swab if bleeding occurs, but avoid massaging the site, as this can disrupt vaccine absorption.
Mastering injection technique is not just about following guidelines—it’s about ensuring safety, efficacy, and patient trust. A poorly administered vaccine can lead to reduced immunity, increased side effects, or even mistrust in vaccination programs. For instance, improper IM injection of the tetanus vaccine can cause localized pain and swelling, while incorrect SC administration of the HPV vaccine may result in inadequate immune response. By adhering to proper needle size, angle, and depth, healthcare providers can maximize vaccine effectiveness while minimizing patient discomfort, reinforcing the importance of precision in every step of the vaccination process.
Vaccination Deadline: Key Dates You Need to Know Now
You may want to see also
Explore related products






![]()
Post-vaccination Care: Monitor for adverse reactions, provide aftercare instructions, and schedule follow-up if needed
After administering a vaccine, the immediate focus shifts to ensuring the recipient’s safety and comfort. Monitoring for adverse reactions is critical, as it allows for swift intervention if complications arise. Common side effects like mild fever, soreness at the injection site, or fatigue are typically benign and resolve within 24–48 hours. However, severe reactions such as difficulty breathing, swelling of the face or throat, or persistent high fever (above 103°F or 39.4°C) require immediate medical attention. For children under 5, caregivers should watch for unusual crying, lethargy, or refusal to eat, as these may signal a serious issue. Adults, particularly those with pre-existing conditions, should be vigilant for symptoms like rapid heartbeat or dizziness. Always keep emergency contact information readily available during this observation period.
Providing clear aftercare instructions empowers recipients to manage post-vaccination symptoms effectively. Encourage hydration and rest, as these aid the body’s immune response. Over-the-counter pain relievers like acetaminophen (500–1000 mg every 4–6 hours for adults) can alleviate discomfort, but avoid aspirin for children under 18 due to the risk of Reye’s syndrome. Applying a cool, damp cloth to the injection site can reduce swelling, but refrain from strenuous activity for at least 24 hours. For infants and toddlers, gentle massaging around the injection site may ease pain. If a rash or persistent redness develops, consult a healthcare provider. Emphasize the importance of avoiding antihistamines or other medications unless specifically advised by a professional, as they may mask symptoms of a severe reaction.
Scheduling follow-up appointments is essential for vaccines requiring multiple doses or booster shots. For example, the COVID-19 mRNA vaccines typically require a second dose 3–4 weeks after the first, while the HPV vaccine series spans 6–12 months for adolescents aged 9–14. Adults receiving the shingles vaccine (Shingrix) need a second dose 2–6 months later. Follow-up visits also provide an opportunity to assess long-term immunity and address any lingering concerns. Keep a vaccination record handy, noting dates, vaccine types, and lot numbers, as this information is crucial for future healthcare decisions. Digital tools like immunization apps can simplify tracking, especially for families managing multiple schedules.
Comparing post-vaccination care across age groups highlights the need for tailored approaches. While adolescents and adults may tolerate mild side effects with minimal intervention, infants and the elderly often require closer monitoring. For instance, older adults receiving the flu vaccine should be observed for signs of confusion or weakness, which could indicate a rare but serious reaction. Conversely, parents of young children should be advised to monitor for high-pitched crying or seizures, which, though rare, are red flags for conditions like febrile seizures. Cultural sensitivity is also key; some communities may prefer natural remedies, so healthcare providers should offer evidence-based alternatives that align with their beliefs while ensuring safety.
In conclusion, post-vaccination care is a multifaceted process that demands vigilance, clear communication, and individualized attention. By monitoring for adverse reactions, providing detailed aftercare instructions, and scheduling necessary follow-ups, healthcare providers can maximize vaccine efficacy while minimizing risks. This proactive approach not only ensures recipient safety but also builds trust in immunization programs, fostering a healthier community for all.
Delta Variant vs. Vaccines: Effectiveness, Breakthrough Cases, and Protection
You may want to see also
Frequently asked questions
Before administering a vaccine, verify the patient’s identity, medical history, and allergies. Check the vaccine’s expiration date, storage conditions, and dosage. Ensure the correct needle size and syringe are used, and prepare the vaccine according to manufacturer instructions (e.g., reconstitution if required).
For intramuscular (IM) injections, insert the needle at a 90-degree angle into the deltoid muscle (upper arm) or vastus lateralis muscle (thigh for infants/young children). For subcutaneous (SC) injections, insert the needle at a 45- to 90-degree angle into the fatty tissue of the upper arm or thigh. Aspirate only if using a multidose vial to check for blood.
Store vaccines in a refrigerator at 2°C to 8°C (36°F to 46°F) or as per manufacturer guidelines. Avoid freezing unless specified. Protect vaccines from light and use a calibrated thermometer to monitor temperature. Do not use vaccines if storage conditions have been compromised.
After administering the vaccine, dispose of the needle and syringe in a sharps container. Provide the patient with a vaccination record card and inform them about potential side effects. Observe the patient for 15–30 minutes for immediate adverse reactions, especially if they have a history of allergies. Report any severe reactions to the appropriate health authorities.