As of recent data, the percentage of adults vaccinated in the United States has been a critical metric in tracking the nation's progress in combating the COVID-19 pandemic. According to the Centers for Disease Control and Prevention (CDC), approximately 78% of adults aged 18 and older have received at least one dose of a COVID-19 vaccine, while around 67% are fully vaccinated. These figures reflect a significant public health achievement, though disparities persist across demographic groups, geographic regions, and socioeconomic statuses. Efforts to increase vaccination rates continue, with a focus on addressing hesitancy, improving access, and promoting booster shots to enhance immunity against emerging variants.
Explore related products






What You'll Learn
- Vaccination Rates by Age Group: Breakdown of vaccinated adults by age ranges (18-29, 30-49, 50-64, 65+)
- Geographic Distribution: Vaccination percentages across states, urban vs. rural areas, and regional trends
- Vaccine Type Preferences: Distribution of adults vaccinated with Pfizer, Moderna, Johnson & Johnson, or others
- Demographic Disparities: Vaccination rates by race, ethnicity, gender, and socioeconomic status
- Time Trends: Monthly or quarterly changes in adult vaccination percentages since vaccine rollout
![]()
Vaccination Rates by Age Group: Breakdown of vaccinated adults by age ranges (18-29, 30-49, 50-64, 65+)
As of recent data, vaccination rates among adults in the U.S. vary significantly by age group, reflecting differences in health priorities, access, and societal influences. The 65+ age group consistently leads with the highest vaccination rates, often surpassing 90%, due to heightened vulnerability to severe illness and targeted public health campaigns. In contrast, the 18-29 age group lags behind, with rates typically below 70%, influenced by factors like vaccine hesitancy, lower perceived risk, and logistical barriers. Understanding these disparities is crucial for tailoring interventions to boost overall immunity.
Analyzing the 30-49 and 50-64 age groups reveals a middle ground in vaccination uptake. The 50-64 cohort generally achieves rates around 80-85%, driven by increasing health awareness and proximity to Medicare eligibility. Meanwhile, the 30-49 group hovers between 70-75%, balancing work and family responsibilities that may delay vaccination. Employers and healthcare providers can play a pivotal role here by offering on-site clinics or flexible scheduling to remove access barriers. Encouraging this group to complete booster doses, typically recommended every 2-5 years depending on the vaccine, could further enhance protection.
Persuasive efforts must address the 18-29 demographic with targeted strategies. Social media campaigns, peer-led initiatives, and partnerships with colleges or workplaces can combat misinformation and emphasize the long-term benefits of vaccination. For instance, highlighting how the HPV vaccine, ideally administered before age 26, reduces cancer risks can resonate with younger adults. Additionally, simplifying registration processes through apps or walk-in clinics can improve participation. This age group’s lower rates aren’t just a statistic—they represent a critical gap in herd immunity that requires creative solutions.
Comparatively, the success of the 65+ group offers lessons for other age ranges. Seniors benefit from clear messaging about the risks of unvaccinated aging, coupled with accessible resources like transportation to clinics and Medicare coverage for vaccines. Applying similar principles to younger groups—such as linking vaccination to maintaining an active lifestyle or protecting family members—could bridge the gap. For example, framing the flu vaccine as a way to safeguard children or grandparents might motivate the 30-49 group. Tailoring approaches to each age group’s needs and behaviors is key to elevating overall vaccination rates.
Descriptively, the age-based breakdown underscores the importance of a nuanced approach to public health. While older adults have embraced vaccination as a lifeline, younger generations require incentives that align with their values and lifestyles. Practical tips, such as bundling vaccine appointments with routine check-ups for the 50-64 group or offering incentives like gift cards for the 18-29 demographic, can make a tangible difference. By addressing each age group’s unique challenges, the U.S. can move closer to achieving comprehensive vaccine coverage and safeguarding public health for all.
PCV-13 Vaccine: Shielding Against Pneumonia, Meningitis, and Blood Infections
You may want to see also
Explore related products



$32.99 $32.99



![]()
Geographic Distribution: Vaccination percentages across states, urban vs. rural areas, and regional trends
As of recent data, the percentage of fully vaccinated adults in the United States hovers around 68%, with significant variations across geographic regions. This disparity is not random; it reflects a complex interplay of socioeconomic factors, political leanings, and public health infrastructure. To understand these differences, let’s dissect the geographic distribution of vaccination rates, focusing on state-by-state comparisons, the urban-rural divide, and emerging regional trends.
Consider the Northeast, where states like Vermont and Connecticut boast vaccination rates exceeding 80%. These states share common traits: high population density, robust healthcare systems, and strong public health messaging. In contrast, Southern states like Mississippi and Alabama lag behind, with rates below 55%. This regional gap can be attributed to lower access to healthcare, higher poverty rates, and political skepticism toward vaccines. For instance, in Mississippi, only 48% of adults have completed their primary vaccine series, compared to 79% in Vermont. To bridge this gap, targeted outreach programs in underserved areas could emphasize vaccine accessibility through mobile clinics and community partnerships.
The urban-rural divide further complicates the picture. Urban areas consistently report higher vaccination rates than rural regions, often by a margin of 15–20 percentage points. Cities like New York and Los Angeles have rates above 75%, while rural counties in states like Wyoming and Montana struggle to reach 50%. This disparity stems from limited healthcare resources in rural areas, coupled with lower population density and higher reliance on misinformation. A practical solution for rural communities could involve leveraging local trusted figures, such as farmers or clergy, to promote vaccination and address hesitancy.
Regional trends also highlight the impact of policy decisions. States with proactive mandates or incentives, like California’s vaccine verification system, have seen steady increases in vaccination rates. Conversely, states that resisted public health measures, such as Florida and Texas, experienced slower uptake. For example, California’s adult vaccination rate stands at 73%, while Florida’s is 62%. Policymakers in low-vaccination regions should consider adopting proven strategies, such as employer-based incentives or school vaccination drives, to boost coverage.
Finally, age-specific trends within geographic areas reveal further nuances. In most states, older adults (65+) have vaccination rates above 85%, while younger adults (18–29) lag behind, often in the 50–60% range. This gap is particularly pronounced in rural areas, where younger populations face barriers like transportation and misinformation. Tailored campaigns targeting younger demographics, such as social media-driven initiatives or college campus vaccination events, could help close this gap. By addressing these geographic disparities with precision and empathy, the U.S. can move closer to achieving equitable vaccine coverage nationwide.
The Surprising Truth: A Vaccine Already Exists – Here’s How
You may want to see also
Explore related products






![]()
Vaccine Type Preferences: Distribution of adults vaccinated with Pfizer, Moderna, Johnson & Johnson, or others
As of recent data, approximately 70% of adults in the United States are fully vaccinated against COVID-19, reflecting a significant public health achievement. However, this aggregate figure masks the nuanced distribution of vaccine type preferences among the population. Understanding which vaccines—Pfizer, Moderna, Johnson & Johnson, or others—adults have chosen provides insight into public trust, accessibility, and individual health considerations.
Pfizer-BioNTech’s mRNA vaccine leads the distribution, accounting for roughly 58% of all doses administered to adults. Its early authorization in December 2020, coupled with high efficacy rates (95% in clinical trials) and a two-dose regimen (30 µg per dose, 21 days apart), positioned it as a frontrunner. Parents often prefer Pfizer for adolescents aged 12 and older due to its approval for this age group, further boosting its uptake. Moderna follows closely, representing about 38% of adult vaccinations. Its mRNA platform mirrors Pfizer’s but with a higher dosage (100 µg per dose, 28 days apart), which initially raised questions about side effects. However, its efficacy and availability in harder-to-reach areas, such as rural communities, have solidified its role in the vaccination campaign.
Johnson & Johnson’s single-dose viral vector vaccine, while comprising only 4% of adult vaccinations, serves a critical niche. Its one-and-done convenience appealed to individuals hesitant about a multi-dose regimen or those with limited access to healthcare. However, rare but serious side effects, such as thrombosis with thrombocytopenia syndrome (TTS), led to temporary pauses in its rollout, dampening public confidence. Other vaccines, including Novavax and those administered under emergency use authorizations, make up less than 1% of the distribution. Novavax, a protein subunit vaccine, gained traction among those wary of mRNA technology, but its late authorization in July 2022 limited its impact on initial vaccination efforts.
Practical considerations influence vaccine type preferences. For instance, individuals with a history of severe allergies to polyethylene glycol (PEG), a component in mRNA vaccines, may opt for Johnson & Johnson or Novavax. Similarly, those prioritizing rapid protection might choose Johnson & Johnson, despite its lower efficacy (66% in global trials), to avoid the wait between doses. Healthcare providers often recommend Pfizer or Moderna for pregnant individuals due to more extensive safety data, while Johnson & Johnson remains an option for those seeking immediate protection.
In conclusion, the distribution of vaccine type preferences among U.S. adults reflects a combination of scientific efficacy, logistical convenience, and individual health needs. Pfizer’s dominance underscores the public’s trust in early, well-publicized data, while Moderna’s strong showing highlights the importance of accessibility. Johnson & Johnson’s niche role and the emergence of alternatives like Novavax demonstrate the value of diverse vaccine options in addressing varied population needs. Understanding these preferences is essential for tailoring future public health strategies and ensuring equitable protection.
Respect My Privacy: Why 'Are You Vaccinated?' Is Off-Limits
You may want to see also
Explore related products






![]()
Demographic Disparities: Vaccination rates by race, ethnicity, gender, and socioeconomic status
As of the latest data, approximately 70% of adults in the United States are fully vaccinated against COVID-19, but this figure masks significant disparities across demographic groups. These differences in vaccination rates are not random; they reflect deeper systemic inequalities in access, trust, and healthcare infrastructure. Understanding these disparities is crucial for tailoring interventions that ensure equitable health outcomes.
Race and Ethnicity: A Persistent Divide
Vaccination rates among racial and ethnic minorities in the U.S. highlight stark inequities. For instance, while 72% of White adults are fully vaccinated, only 62% of Hispanic and 58% of Black adults have received their doses. These gaps are rooted in historical mistrust of medical institutions, exacerbated by structural barriers like limited access to vaccination sites in underserved communities. For example, in rural areas with predominantly Black populations, vaccine hesitancy is often compounded by a lack of nearby pharmacies or clinics. Addressing this requires culturally sensitive outreach, such as partnering with community leaders to disseminate accurate information and establishing mobile vaccination units in high-need areas.
Gender: Subtle but Significant Differences
Gender plays a less pronounced but still notable role in vaccination disparities. Data shows that women are slightly more likely than men to be vaccinated, with 71% of women fully vaccinated compared to 68% of men. This gap may stem from differences in health-seeking behavior, as women are generally more likely to engage with preventive healthcare. However, among younger age groups (18–29), men are more hesitant, often influenced by misinformation about vaccine side effects. Tailored messaging that addresses specific concerns, such as fertility myths, can help bridge this gap. For instance, campaigns featuring male role models discussing their vaccination experiences could resonate with hesitant men.
Socioeconomic Status: Wealth and Health Inequities
Socioeconomic status is a powerful predictor of vaccination rates. Adults with higher incomes and education levels are significantly more likely to be vaccinated. For example, 80% of adults with a college degree are fully vaccinated, compared to just 58% of those with a high school diploma or less. This disparity is driven by factors like job flexibility (allowing time for vaccination), access to reliable transportation, and digital literacy to schedule appointments. Practical solutions include offering vaccines at workplaces, schools, and community centers, as well as providing paid time off for vaccination and recovery. Additionally, simplifying registration processes and offering multilingual support can reduce barriers for low-income populations.
Intersectionality: Where Disparities Converge
The most significant disparities emerge at the intersection of multiple demographics. For example, low-income Black women face compounded challenges due to racial bias, gendered health disparities, and economic instability. In these cases, one-size-fits-all approaches fall short. Instead, targeted strategies are needed, such as community-based initiatives that address specific concerns (e.g., debunking myths about vaccines affecting fertility) while providing tangible support like childcare during vaccination appointments. By acknowledging these intersections, public health efforts can move beyond broad statistics to address the nuanced needs of marginalized groups.
In conclusion, while the overall vaccination rate in the U.S. is substantial, demographic disparities reveal a fragmented landscape. Closing these gaps requires a multifaceted approach that tackles systemic barriers, builds trust, and meets communities where they are. Only then can we achieve true health equity.
Shingrix Vaccine: Is It Covered by Medicare Part B?
You may want to see also
Explore related products






![]()
Time Trends: Monthly or quarterly changes in adult vaccination percentages since vaccine rollout
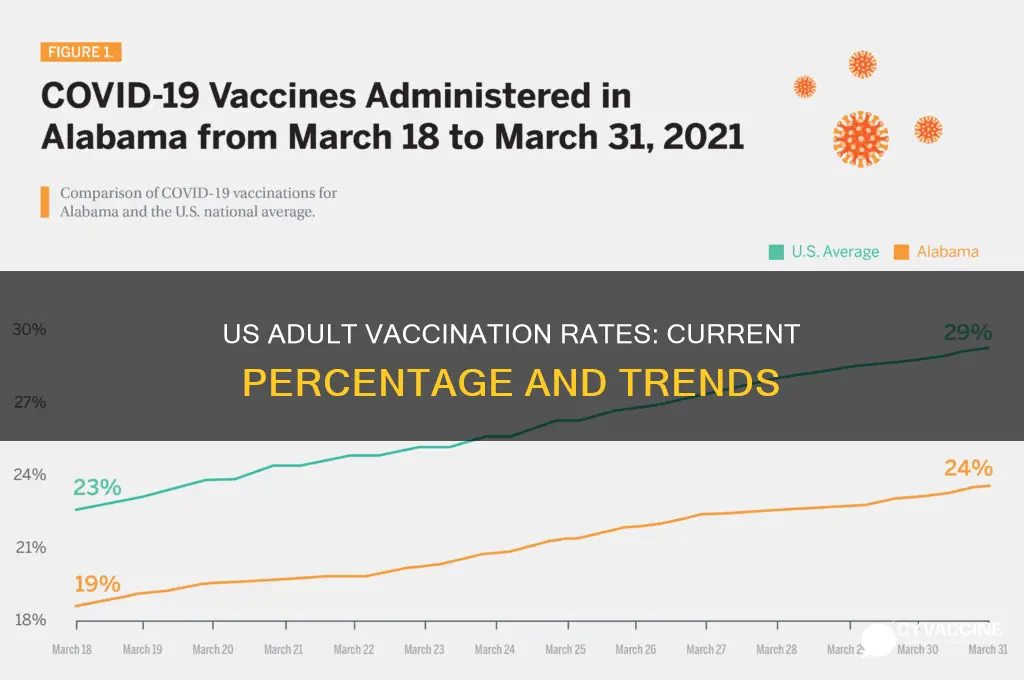
The rollout of COVID-19 vaccines in the United States marked a pivotal moment in the pandemic, with adult vaccination rates serving as a critical metric for public health progress. Analyzing monthly or quarterly changes in these percentages reveals a dynamic landscape shaped by factors such as vaccine availability, public trust, and evolving health guidelines. In the early months of 2021, vaccination rates surged as eligibility expanded from healthcare workers and the elderly to the general adult population. By April 2021, over 50% of adults had received at least one dose, a testament to the rapid mobilization of resources and public enthusiasm. However, this momentum began to wane by mid-2021, with monthly increases slowing as vaccine hesitancy and logistical barriers emerged.
Quarterly data highlights distinct phases in the vaccination campaign. The second quarter of 2021 saw a peak in first-dose administrations, driven by widespread availability and public health messaging. By the third quarter, focus shifted to completing the two-dose series for mRNA vaccines, with monthly changes reflecting efforts to close the gap between partially and fully vaccinated adults. For example, the percentage of fully vaccinated adults rose from 43% in June 2021 to 54% by September 2021, a 25% relative increase. This period also saw the introduction of booster shots, adding complexity to tracking vaccination trends as metrics expanded beyond initial doses.
Instructively, understanding these time trends requires disaggregating data by age, geography, and vaccine type. Younger adults (18–29 years) initially lagged behind older age groups but experienced steady quarterly increases as targeted outreach campaigns addressed hesitancy. Rural areas consistently trailed urban centers, underscoring the need for localized strategies. For instance, monthly vaccination rates in rural counties rose by an average of 1.5% between July and December 2021, compared to 2.2% in urban counties, highlighting persistent disparities.
Persuasively, the data underscores the importance of sustained efforts to maintain momentum. The fourth quarter of 2021 exemplified this, as the emergence of the Omicron variant spurred a 10% quarterly increase in booster uptake among adults. However, monthly changes also revealed fatigue, with growth rates plateauing despite ongoing campaigns. Practical tips for policymakers include leveraging seasonal health campaigns (e.g., flu shot drives) to promote COVID-19 boosters and addressing misinformation through trusted community messengers.
Comparatively, the U.S. experience contrasts with countries like Israel and Canada, where quarterly vaccination increases remained steadier due to stronger centralized coordination. The U.S.’s decentralized approach led to variability, with some states achieving over 70% adult vaccination by late 2021, while others remained below 50%. This comparison suggests that while flexibility has benefits, consistent national strategies could mitigate monthly fluctuations.
In conclusion, tracking monthly or quarterly changes in adult vaccination percentages provides actionable insights for refining public health strategies. From the rapid initial uptake to the challenges of sustaining growth, these trends reveal both successes and areas for improvement. By focusing on granular data and adapting approaches in real time, stakeholders can navigate evolving dynamics and drive progress toward higher vaccination coverage.
Chickenpox Post-Vaccination: Symptoms, Appearance, and What to Expect
You may want to see also
Frequently asked questions
As of the latest data, approximately 70-75% of adults in the U.S. have received at least one dose of a COVID-19 vaccine, with about 65-70% being fully vaccinated.
Vaccination rates are highest among older adults, with over 90% of those aged 65 and older fully vaccinated, while younger adults (18-29) have lower rates, typically around 50-60%.
Approximately 30-40% of fully vaccinated adults in the U.S. have received at least one booster dose, though this varies by age and region.
Yes, vaccination rates vary widely by state, with some states exceeding 80% of adults fully vaccinated, while others have rates below 50%, influenced by factors like politics, access, and public health messaging.