Influenza A vaccines are designed to stimulate the immune system to recognize and combat the influenza A virus, a major cause of seasonal flu outbreaks. These vaccines primarily work by introducing inactivated or attenuated forms of the virus, or specific viral proteins like hemagglutinin (HA), to the body. Upon vaccination, the immune system identifies these components as foreign, prompting the production of antibodies that target and neutralize the virus. Additionally, vaccines can induce memory cells, which provide a rapid and effective response upon future exposure to the virus. The mechanism relies on mimicking a natural infection without causing illness, thereby preparing the immune system to prevent or mitigate influenza A infections. However, the virus's ability to mutate requires annual updates to the vaccine composition to match circulating strains, ensuring continued efficacy.
| Characteristics | Values |
|---|---|
| Vaccine Type | Inactivated (IIV), Live Attenuated (LAIV), Recombinant (RIV), Cell-based, Egg-based |
| Target Antigen | Hemagglutinin (HA) and Neuraminidase (NA) surface proteins of Influenza A virus |
| Mechanism of Action | Induces humoral immune response by stimulating production of neutralizing antibodies against HA and NA |
| Immune Response | Primarily IgG antibodies targeting HA head region, preventing viral attachment and entry into host cells |
| Efficacy | Varies annually (20-60%) due to antigenic drift and vaccine-virus mismatch; higher in years with good match |
| Duration of Protection | 6-8 months, waning due to antibody decline and viral mutation |
| Administration Route | Intramuscular (IIV, RIV) or Intranasal (LAIV) |
| Age Indication | IIV: 6 months and older; LAIV: 2-49 years (healthy, non-pregnant individuals) |
| Dose | Standard dose (15 µg HA per strain) or high-dose (60 µg HA per strain for ≥65 years) |
| Strain Composition | Updated annually by WHO/CDC based on global surveillance data (typically 2 Influenza A strains: H1N1 and H3N2) |
| Adjuvants | MF59 (squalene-based) or AS03 in some formulations to enhance immunogenicity, especially in elderly |
| Storage | Refrigerated (2-8°C) for IIV/RIV; Frozen (-15°C) for LAIV |
| Side Effects | Mild: Injection site pain, headache, fatigue; Rare: Guillain-Barré syndrome (GBS) |
| Contraindications | Severe allergic reaction to vaccine components; LAIV contraindicated in immunocompromised, pregnant, or asthmatic individuals |
| Latest Advances | Universal flu vaccines (targeting conserved epitopes), mRNA-based vaccines, and nanoparticle technologies under development |
| Annual Update | Required due to antigenic drift and shift in circulating influenza A strains |
Explore related products






What You'll Learn
- Antigen Selection: Process of choosing specific viral strains for vaccine development based on global surveillance data
- Vaccine Types: Overview of inactivated, live attenuated, and recombinant influenza A vaccine technologies
- Immune Response: How vaccines stimulate antibody production and T-cell activation against influenza A viruses
- Manufacturing Process: Steps from virus cultivation to formulation, purification, and quality control of vaccines
- Efficacy Factors: Influence of age, immunity, and viral mutation on vaccine effectiveness against influenza A
![]()
Antigen Selection: Process of choosing specific viral strains for vaccine development based on global surveillance data
Influenza A viruses are masters of disguise, constantly evolving through antigenic drift and shift to evade our immune systems. This shape-shifting ability necessitates a proactive approach to vaccine development, where the selection of specific viral strains is a critical, data-driven process. Global surveillance networks act as the sentinel, monitoring circulating influenza strains worldwide, identifying emerging variants, and predicting which ones are most likely to dominate in the upcoming season.
This global surveillance data is the cornerstone of antigen selection. It's a complex dance, analyzing virus samples from diverse geographic regions, sequencing their genomes, and assessing their antigenic properties. This information is then fed into a sophisticated decision-making process, considering factors like the prevalence of specific strains, their genetic relatedness to previous vaccine strains, and their potential to cause severe disease.
Imagine a vast, interconnected web of laboratories and health organizations, constantly collecting and sharing data on influenza viruses. This real-time intelligence allows scientists to identify emerging strains with pandemic potential, track the evolution of existing strains, and predict which variants are most likely to circulate widely in the coming months. This predictive power is crucial, as it takes months to manufacture and distribute influenza vaccines.
The World Health Organization (WHO) plays a pivotal role in this process, convening twice annually to analyze global surveillance data and recommend the specific strains to be included in the upcoming season's influenza vaccines. These recommendations are then adopted by vaccine manufacturers worldwide, ensuring a coordinated global effort to combat the ever-changing influenza virus.
The antigen selection process is a delicate balance between scientific rigor and practical considerations. While ideally, the vaccine would perfectly match the circulating strains, this is rarely achievable due to the virus's rapid evolution. Therefore, the goal is to select strains that provide the broadest possible protection, even against slightly mismatched viruses. This is achieved through a combination of genetic analysis, antigenic characterization, and serological studies, which assess the immune response elicited by potential vaccine candidates.
Ultimately, the success of influenza vaccination hinges on the accuracy of antigen selection. By leveraging global surveillance data and sophisticated analytical tools, scientists strive to stay one step ahead of the virus, ensuring that the vaccines we receive offer the best possible protection against this ever-evolving threat.
Missouri Vaccine Lottery Sign-Up Guide: Easy Steps to Enter and Win
You may want to see also
Explore related products

$248.11 $319





![]()
Vaccine Types: Overview of inactivated, live attenuated, and recombinant influenza A vaccine technologies
Influenza A vaccines are designed to stimulate the immune system to recognize and combat the virus, reducing the severity and spread of the disease. Among the various technologies employed, inactivated, live attenuated, and recombinant vaccines stand out as the primary approaches. Each type operates through distinct mechanisms, offering unique advantages and considerations for different populations.
Inactivated Influenza A Vaccines are the most widely used and are produced by growing the virus in eggs or cell cultures, then inactivating it using chemicals like formaldehyde. This process renders the virus unable to replicate but leaves its surface proteins intact, allowing the immune system to recognize and mount a response. These vaccines are typically administered via intramuscular injection, with a standard dose of 0.5 mL for adults and children over 3 years. They are suitable for individuals aged 6 months and older, including those with chronic conditions, as they pose minimal risk of virus-related complications. However, their effectiveness can wane over time, necessitating annual revaccination due to viral mutation and immune system changes.
Live Attenuated Influenza Vaccines (LAIV), such as the nasal spray FluMist, contain weakened forms of the virus that can replicate but do not cause illness in healthy individuals. This replication triggers a robust immune response, including mucosal immunity in the respiratory tract, which is the primary site of infection. LAIV is administered intranasally, with a dose of 0.2 mL (0.1 mL per nostril) for children and adults. It is approved for individuals aged 2 to 49 years but is contraindicated for pregnant women, immunocompromised individuals, and those with certain chronic conditions due to the theoretical risk of virus reversion to a virulent form. LAIV’s advantage lies in its ease of administration and potentially broader immune response, though its efficacy can vary depending on the circulating strains.
Recombinant Influenza A Vaccines represent a cutting-edge approach, utilizing genetic engineering to produce viral proteins without the need for live virus. These vaccines contain recombinant hemagglutinin (HA), a key surface protein of the influenza virus, which is manufactured in insect cells using baculovirus vectors. This method eliminates the risk of egg-related allergies and allows for rapid production scalability during pandemics. Recombinant vaccines, such as Flublok, are approved for individuals aged 18 and older and are administered as a 0.5 mL intramuscular injection. They are particularly beneficial for those with egg allergies and offer a highly purified, consistent antigen. However, their cost and limited availability can be barriers to widespread use.
In summary, the choice of influenza A vaccine depends on factors such as age, health status, and specific immune response needs. Inactivated vaccines provide a safe, broad option for most populations, while LAIV offers convenience and mucosal immunity for healthy individuals. Recombinant vaccines cater to niche needs, such as egg allergies, and showcase the potential of modern biotechnology. Understanding these mechanisms empowers healthcare providers and individuals to make informed decisions, optimizing protection against this ever-evolving virus.
Is the Smallpox Vaccine Included in Childhood Immunizations Today?
You may want to see also
Explore related products






![]()
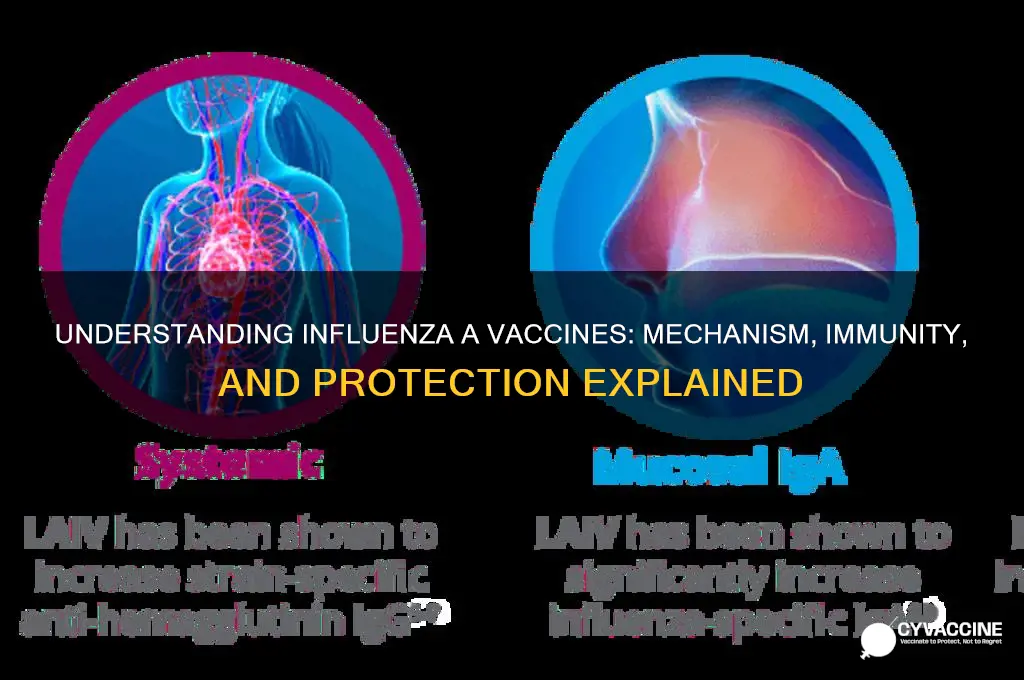
Immune Response: How vaccines stimulate antibody production and T-cell activation against influenza A viruses
Influenza A viruses are notorious for their ability to mutate rapidly, making annual vaccination a critical public health strategy. The mechanism behind influenza A vaccines hinges on their ability to stimulate a robust immune response, specifically by triggering antibody production and T-cell activation. These vaccines, typically administered as inactivated virus particles or recombinant proteins, introduce viral antigens—such as hemagglutinin (HA)—to the immune system without causing illness. Upon vaccination, antigen-presenting cells (APCs) engulf these antigens, process them, and present fragments (epitopes) on their surface via major histocompatibility complex (MHC) molecules. This presentation is the first step in a cascade that mobilizes both humoral and cellular immunity.
The humoral immune response is primarily mediated by B lymphocytes, which differentiate into plasma cells upon recognizing the presented antigens. These plasma cells secrete antibodies, specifically IgG and IgA, that bind to the HA protein on the surface of influenza A viruses. Neutralizing antibodies prevent viral attachment to host cells, effectively blocking infection. For optimal protection, the World Health Organization recommends vaccines induce an HA inhibition (HAI) titer of at least 1:40 in adults and 1:110 in the elderly, as these levels correlate with reduced disease risk. However, antibody production alone is insufficient for complete immunity, particularly in populations with waning immune function, such as the elderly or immunocompromised.
T-cell activation complements the humoral response by targeting infected cells directly. When APCs present viral epitopes via MHC class I or II molecules, they activate CD8+ cytotoxic T cells and CD4+ helper T cells, respectively. CD8+ T cells identify and destroy virus-infected cells, while CD4+ T cells provide essential support by secreting cytokines like interferon-gamma and interleukin-2, which enhance both antibody production and cytotoxic activity. This dual-pronged approach ensures that even if the virus evades neutralizing antibodies, the immune system can still control the infection. Studies show that T-cell responses are particularly crucial in individuals with pre-existing immunity, as they can recognize conserved viral epitopes despite HA mutations.
Practical considerations for maximizing vaccine efficacy include timing and dosage. Annual vaccination is recommended due to antigenic drift in influenza A viruses, with optimal administration in early fall to ensure peak immunity during flu season. Standard doses for adults contain 15 µg of HA per strain, while high-dose vaccines (up to 60 µg) are available for individuals over 65 to compensate for age-related immune decline. Adjuvanted vaccines, such as those containing AS03 or MF59, enhance immune responses by promoting APC activation and prolonging antigen presentation, making them particularly beneficial for the elderly or immunocompromised.
In conclusion, influenza A vaccines harness the immune system’s innate ability to recognize and combat pathogens by stimulating both antibody production and T-cell activation. Understanding this mechanism underscores the importance of vaccination not only as a preventive measure but also as a tool for reducing disease severity in breakthrough infections. By tailoring vaccine formulations and dosages to specific populations, public health strategies can optimize protection against this ever-evolving virus.
Vaccinated Children Mortality Rates: Debunking Myths with Scientific Evidence
You may want to see also
Explore related products






![]()
Manufacturing Process: Steps from virus cultivation to formulation, purification, and quality control of vaccines
The manufacturing of influenza A vaccines is a complex, multi-step process that begins with virus cultivation and culminates in a purified, formulated product ready for administration. This journey ensures the vaccine’s safety, efficacy, and consistency, adhering to stringent regulatory standards. Here’s a detailed breakdown of the steps involved, from the lab to the vial.
Virus Cultivation: The Foundation of Vaccine Production
The process starts with the selection and growth of influenza A viruses. These are typically cultivated in embryonated chicken eggs or cell-based systems, such as Madin-Darby Canine Kidney (MDCK) cells. For egg-based methods, fertilized eggs are inoculated with the virus, which replicates within the embryonic cells. Cell-based systems, on the other hand, offer a faster and more scalable alternative, particularly during pandemics. The choice of method depends on factors like cost, scalability, and the specific virus strain. Once the virus reaches sufficient titers, it is harvested, marking the first critical step in vaccine production.
Formulation: Crafting the Vaccine’s Structure
After cultivation, the virus undergoes inactivation or attenuation to ensure it cannot cause disease. Inactivated vaccines, the most common type, are treated with chemicals like formaldehyde. Attenuated vaccines, used in nasal sprays, are weakened through genetic modification. Next, the antigen is combined with adjuvants (e.g., aluminum salts) to enhance immune response, stabilizers (e.g., gelatin) to prolong shelf life, and preservatives (e.g., thiomersal) to prevent contamination. The formulation is carefully calibrated to deliver the optimal dose, typically 15 µg of hemagglutinin per strain for adults and adjusted for pediatric populations.
Purification: Removing Impurities for Safety
Purification is a critical step to remove cellular debris, residual egg proteins, and other contaminants. Techniques such as ultrafiltration, chromatography, and centrifugation are employed to isolate the viral antigens. For egg-based vaccines, this step is particularly important to minimize allergic reactions in sensitive individuals. The purified antigen is then tested for purity and potency, ensuring it meets regulatory requirements before proceeding to the final formulation.
Quality Control: Ensuring Safety and Efficacy
Rigorous quality control measures are implemented at every stage to verify the vaccine’s safety, potency, and consistency. Tests include sterility checks, antigen quantification, and stability assessments under various conditions. For example, the single radial immunodiffusion (SRID) assay is commonly used to measure hemagglutinin content. Batches that fail any quality control test are discarded. Additionally, clinical trials in humans further validate the vaccine’s immunogenicity and safety before it is approved for distribution.
Practical Considerations and Takeaways
The manufacturing process of influenza A vaccines is a testament to scientific precision and regulatory oversight. From virus cultivation to final formulation, each step is designed to maximize efficacy while minimizing risks. For healthcare providers, understanding this process underscores the importance of proper storage (e.g., 2–8°C for most vaccines) and administration (e.g., intramuscular injection for inactivated vaccines). For the public, it highlights the meticulous efforts behind every dose, reinforcing confidence in vaccination as a critical public health tool.
How Vaccines Work: A Journey Through Your Immune System
You may want to see also
Explore related products





![]()
Efficacy Factors: Influence of age, immunity, and viral mutation on vaccine effectiveness against influenza A
The effectiveness of influenza A vaccines is not uniform across all populations, and understanding the factors that influence efficacy is crucial for optimizing vaccination strategies. Age, immunity, and viral mutation play pivotal roles in determining how well these vaccines protect against infection. For instance, older adults, particularly those over 65, often exhibit reduced vaccine efficacy due to immunosenescence—the gradual decline of the immune system with age. This demographic may require higher-dose vaccines, such as the Fluzone High-Dose, which contains four times the antigen of standard vaccines, to elicit a robust immune response. Conversely, children and young adults typically respond more vigorously to standard doses, though prior immunity from previous infections or vaccinations can modulate their response.
Immunity, whether innate or acquired, significantly impacts vaccine effectiveness. Individuals with pre-existing immunity, either from past influenza infections or vaccinations, may produce a faster and stronger antibody response upon vaccination. However, this can also lead to "original antigenic sin," where the immune system preferentially recalls memory B cells from earlier exposures, potentially reducing the efficacy against new strains. For immunocompromised individuals, such as those with HIV or undergoing chemotherapy, vaccine effectiveness is often diminished, necessitating additional measures like booster shots or antiviral prophylaxis. Understanding these immune dynamics is essential for tailoring vaccination protocols to specific populations.
Viral mutation, particularly antigenic drift in the hemagglutinin (HA) protein, poses a constant challenge to vaccine efficacy. Influenza A viruses evolve rapidly, altering their surface proteins to evade immune recognition. This is why the World Health Organization updates vaccine strains annually based on global surveillance data. However, mismatches between vaccine strains and circulating viruses can occur, reducing effectiveness. For example, during the 2014-2015 flu season, the H3N2 strain underwent significant mutations, leading to vaccine effectiveness estimates as low as 13%. Such instances highlight the need for next-generation vaccines, like universal flu vaccines targeting conserved viral regions, to provide broader and more durable protection.
Practical considerations for maximizing vaccine efficacy include timing and adherence. Vaccination should ideally occur before the flu season peaks, typically by the end of October in the Northern Hemisphere, to ensure adequate immune response development. For older adults, combining vaccination with lifestyle measures like regular exercise and a balanced diet can enhance immune function. Additionally, public health campaigns should emphasize the importance of annual vaccination, as immunity wanes over time and viral strains evolve. By addressing these efficacy factors, healthcare providers can improve outcomes and reduce the burden of influenza A.
Navigating Family Vaccine Refusal: Strategies for Respectful Conversations and Boundaries
You may want to see also
Frequently asked questions
Influenza A vaccines primarily work by stimulating the immune system to produce antibodies against the hemagglutinin (HA) and neuraminidase (NA) proteins on the surface of the influenza virus. These antibodies help neutralize the virus and prevent infection or reduce the severity of the disease.
Influenza A vaccines achieve long-term immunity by inducing the formation of memory B cells and T cells. Memory B cells can quickly produce antibodies upon re-exposure to the virus, while memory T cells help recognize and eliminate infected cells, providing a rapid and effective immune response.
Influenza A vaccines need to be updated annually due to the virus's ability to undergo antigenic drift, where genetic mutations alter the HA and NA proteins. These changes can make previous antibodies less effective, necessitating new vaccine formulations to match the circulating strains.