The inactivated poliovirus vaccine (IPV) is a critical tool in the global effort to eradicate polio, a highly contagious viral disease that can lead to paralysis or death. Unlike the oral polio vaccine (OPV), which uses a weakened form of the virus, IPV contains inactivated (killed) poliovirus strains, making it incapable of causing the disease. Administered through injection, IPV stimulates the body’s immune system to produce antibodies against all three types of poliovirus, providing robust protection without the risk of vaccine-derived poliovirus cases, which can occur with OPV. Widely used in many countries, IPV plays a vital role in maintaining polio-free status and ensuring long-term immunity, particularly in regions transitioning from OPV to IPV as part of the global polio eradication strategy.
| Characteristics | Values |
|---|---|
| Definition | A vaccine containing inactivated (killed) poliovirus strains (Type 1, 2, and 3) to induce immunity without risk of viral replication. |
| Administration Route | Intramuscular or subcutaneous injection |
| Dose | Varies by age and formulation (e.g., 0.5 mL for adults, 0.1 mL for infants) |
| Schedule | Typically a series of 3-4 doses starting at 2 months of age, followed by boosters |
| Efficacy | Highly effective in preventing paralytic polio and long-term immunity |
| Storage | Requires refrigeration (2°C to 8°C) to maintain potency |
| Side Effects | Mild: pain at injection site, fever, irritability; Rare: severe allergic reactions |
| Contraindications | Severe allergic reaction to previous dose or vaccine components |
| Global Use | Widely used in polio eradication efforts, especially in endemic regions |
| Brand Examples | IPV (generic), Ipol, Imovax Polio, Pediacel (combined vaccines) |
| Development | Introduced in 1955 as an alternative to the oral polio vaccine (OPV) |
| WHO Recommendation | Preferred in polio-free countries due to zero risk of vaccine-derived poliovirus |
| Immune Response | Stimulates humoral immunity (antibodies) but not mucosal immunity |
| Cost | Varies by region; generally more expensive than OPV |
| Stability | Sensitive to heat and light; must be handled and stored properly |
| Eradication Impact | Key tool in the global polio eradication initiative |
Explore related products






What You'll Learn
- Vaccine Composition: Contains inactivated poliovirus strains 1, 2, and 3, grown in cell cultures
- Administration Method: Typically given via intramuscular or subcutaneous injection in multiple doses
- Immunity Mechanism: Stimulates production of antibodies against poliovirus, preventing infection and paralysis
- Effectiveness: Provides long-term protection, reducing polio cases by over 99% globally
- Side Effects: Mild reactions include soreness, fever, or allergic responses, rarely severe complications
![]()
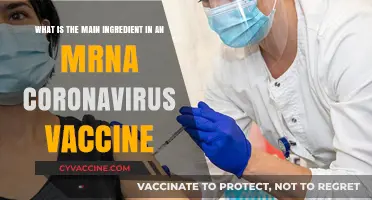
Vaccine Composition: Contains inactivated poliovirus strains 1, 2, and 3, grown in cell cultures
The inactivated poliovirus vaccine (IPV) is a cornerstone of global efforts to eradicate polio, a once-feared disease that can cause paralysis and death. Its composition is precise and purposeful: it contains inactivated (killed) strains of poliovirus types 1, 2, and 3, grown in cell cultures. This method ensures the virus cannot replicate in the body but still triggers a robust immune response, preparing the immune system to recognize and combat live poliovirus if exposed. Unlike the oral polio vaccine (OPV), which uses weakened live virus, IPV eliminates the rare risk of vaccine-derived poliovirus cases, making it a safer option for widespread use.
From a manufacturing perspective, the process of creating IPV is highly controlled. The poliovirus strains are cultivated in specialized cell cultures, often using Vero cells, which provide a reliable and consistent environment for viral growth. Once the virus has multiplied, it is harvested, purified, and inactivated using formaldehyde. This inactivation step is critical—it ensures the virus is no longer capable of causing disease while retaining its immunogenic properties. The final product is a clear, colorless liquid, typically administered intramuscularly or subcutaneously, depending on regional protocols.
For parents and caregivers, understanding IPV’s composition is key to appreciating its safety and efficacy. The vaccine is recommended for children starting at 2 months of age, with a series of doses typically given at 2, 4, and 6–18 months, followed by a booster at 4–6 years. Each dose contains a carefully measured amount of inactivated virus—usually 40 D-antigen units (DU) for type 1, 8 DU for type 2, and 32 DU for type 3. This standardized formulation ensures consistent protection across populations. It’s also worth noting that IPV can be administered alongside other vaccines, simplifying immunization schedules and reducing the number of clinic visits required.
Comparatively, IPV’s cell culture-based production sets it apart from earlier polio vaccines, which relied on animal-derived tissues. This modern approach not only improves safety but also aligns with ethical and practical considerations, as it avoids the risks associated with animal-derived materials. Additionally, the use of inactivated virus makes IPV suitable for individuals with weakened immune systems, who might be at risk from live vaccines. This inclusivity is a significant advantage in global vaccination campaigns, ensuring broader protection against polio.
In practice, the inactivated poliovirus vaccine’s composition underscores its role as a reliable tool in public health. Its targeted design, combining strains 1, 2, and 3, ensures comprehensive immunity against all known poliovirus types. For healthcare providers, this means a straightforward administration process, with minimal side effects typically limited to mild soreness at the injection site. For communities, it means a powerful defense against a disease that, though nearly eradicated, remains a threat in some parts of the world. By understanding what’s in the vaccine, we can better appreciate its role in safeguarding future generations.
Vaccinated Measles Cases: Unraveling the Numbers and Trends
You may want to see also
Explore related products






![]()
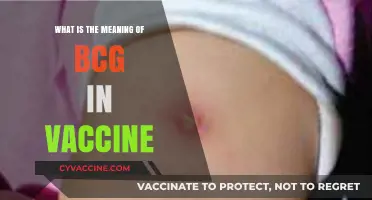
Administration Method: Typically given via intramuscular or subcutaneous injection in multiple doses
The inactivated poliovirus vaccine (IPV) is a cornerstone of global polio eradication efforts, offering robust protection against a disease that once paralyzed millions. Its administration method is as critical as its formulation, ensuring the vaccine’s efficacy and safety. Typically given via intramuscular or subcutaneous injection, this delivery system is designed to trigger a strong immune response while minimizing discomfort and risks. The choice between intramuscular (into the muscle) and subcutaneous (under the skin) routes depends on factors like age, dose volume, and healthcare provider preference, but both methods are proven to deliver the vaccine effectively to the body’s immune system.
Intramuscular injection is the more common route for IPV, particularly in older children and adults. This method delivers the vaccine directly into muscle tissue, where it is rapidly absorbed into the bloodstream. For infants and young children, a smaller dose is administered subcutaneously, often in the thigh or upper arm, to reduce pain and ensure proper absorption. The World Health Organization (WHO) recommends a primary series of three to four doses, starting as early as 6 weeks of age, with intervals of 4 to 8 weeks between doses. This multi-dose regimen is essential to build and sustain immunity, as a single dose provides only partial protection against poliovirus.
Practical considerations for administration include proper needle selection and injection technique. For intramuscular injections, a 22- to 25-gauge needle is typically used, with the injection site being the vastus lateralis muscle in the thigh for infants or the deltoid muscle in older children and adults. Subcutaneous injections require a shorter needle, usually 23- to 25-gauge, and are administered at a 45-degree angle to ensure the vaccine remains in the subcutaneous tissue. Healthcare providers must also ensure the vaccine is stored and handled correctly, as IPV is sensitive to heat and light, which can degrade its potency.
Comparatively, IPV’s injection-based administration sets it apart from the oral polio vaccine (OPV), which is delivered as drops. While OPV offers the advantage of ease and mucosal immunity, IPV’s injectable form eliminates the rare risk of vaccine-derived poliovirus cases. This makes IPV the preferred choice in polio-free regions, where the focus is on maintaining immunity without the risk of vaccine-associated disease. However, the injection method does require trained personnel and sterile equipment, which can pose challenges in resource-limited settings.
For parents and caregivers, understanding the administration process can alleviate concerns and ensure cooperation during vaccination. It’s important to prepare children by explaining the procedure in simple terms and offering comfort during the injection. Distraction techniques, such as singing or showing a favorite toy, can help reduce anxiety. After vaccination, mild side effects like soreness at the injection site or low-grade fever are normal and typically resolve within a day or two. Adhering to the full dose schedule is crucial, as incomplete vaccination leaves individuals vulnerable to poliovirus infection. In the global fight against polio, the precise and consistent administration of IPV is a vital step toward eradication.
Decoding Your Shot Record: Understanding Meningitis Vaccine Documentation
You may want to see also
Explore related products






![]()
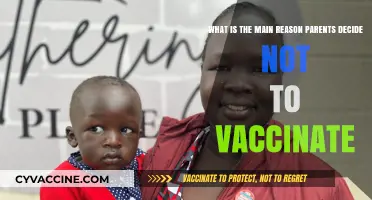
Immunity Mechanism: Stimulates production of antibodies against poliovirus, preventing infection and paralysis
The inactivated poliovirus vaccine (IPV) operates by priming the immune system to recognize and combat poliovirus without exposing the body to the risks of live virus. Unlike oral polio vaccine (OPV), which uses a weakened form of the virus, IPV contains killed poliovirus strains, making it incapable of causing disease. When administered, typically via intramuscular injection, the vaccine introduces viral antigens into the body, triggering a precise immune response. This mechanism is crucial for individuals with compromised immune systems or those living in regions where vaccine-derived poliovirus circulation is a concern.
At the heart of IPV’s immunity mechanism is the stimulation of antibody production. Once the vaccine’s viral particles are detected, B cells—a type of white blood cell—are activated to produce antibodies specific to the three poliovirus serotypes (1, 2, and 3). These antibodies circulate in the bloodstream, ready to neutralize the virus if exposure occurs. Unlike OPV, which also induces mucosal immunity in the gut, IPV primarily generates humoral immunity, meaning it focuses on preventing viremia (virus in the blood) rather than blocking viral replication in the intestinal tract. This distinction is critical for understanding IPV’s role in preventing paralysis, as poliovirus must enter the bloodstream to reach the central nervous system and cause paralytic disease.
For optimal protection, the World Health Organization (WHO) recommends a multi-dose schedule for IPV, typically starting at 2 months of age. In many countries, infants receive a series of 3–4 doses, with intervals of 4–8 weeks between doses, followed by a booster at 4–6 years. The exact dosage and timing may vary by region, so adherence to local immunization guidelines is essential. For adults traveling to polio-endemic areas, a single lifetime booster dose of IPV is often sufficient if they received a complete childhood series. It’s important to note that while IPV prevents paralysis and severe disease, it may not completely halt asymptomatic transmission, underscoring the need for high population coverage to achieve herd immunity.
Practical considerations for IPV administration include ensuring proper storage at 2°C–8°C to maintain vaccine potency and using sterile techniques during injection to prevent contamination. Parents and caregivers should be informed about potential mild side effects, such as soreness at the injection site or low-grade fever, which are normal immune responses. Unlike OPV, IPV cannot cause vaccine-associated paralytic polio (VAPP), making it a safer option for immunocompromised individuals. However, its higher cost and logistical challenges, such as the need for trained healthcare workers to administer injections, have limited its use in low-resource settings, where OPV remains the primary tool for polio eradication.
In summary, IPV’s immunity mechanism hinges on its ability to stimulate antibody production, effectively neutralizing poliovirus and preventing it from causing paralysis. While it lacks the mucosal immunity benefits of OPV, its safety profile and targeted action make it a cornerstone of polio prevention strategies, particularly in the endgame of global eradication efforts. By understanding its unique mechanism and practical implications, healthcare providers and policymakers can optimize its use to protect vulnerable populations and sustain a polio-free world.
Monsanto's Medical Research Division: Vaccine Involvement Explored
You may want to see also
Explore related products






![]()
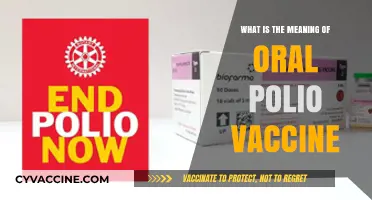
Effectiveness: Provides long-term protection, reducing polio cases by over 99% globally
The inactivated poliovirus vaccine (IPV) stands as a cornerstone in the global effort to eradicate polio, a once-feared disease that caused paralysis and death, particularly among children. Its effectiveness is not just a statistical triumph but a transformative force in public health. Since its introduction, IPV has provided long-term protection, slashing polio cases by over 99% globally. This achievement is a testament to the vaccine’s ability to induce robust immunity without the risks associated with live attenuated vaccines. Administered through injection, typically in a series of doses starting at 2 months of age, IPV contains inactivated (killed) poliovirus strains, ensuring safety while triggering a strong immune response. This method has been pivotal in protecting individuals and communities, especially in regions where polio remains a threat.
Consider the practical implications of this effectiveness. For parents, the IPV schedule is straightforward: a primary series of 3–4 doses, followed by a booster. In the U.S., the CDC recommends doses at 2, 4, and 6–18 months, with a final dose at 4–6 years. This regimen ensures sustained immunity, reducing the risk of infection even in areas with low vaccination rates. For healthcare providers, IPV’s long-term protection simplifies follow-up care, as immunity persists for decades, often requiring no additional boosters in adulthood. This reliability has been critical in low-income countries, where consistent access to healthcare can be challenging. By providing durable immunity, IPV not only protects individuals but also contributes to herd immunity, breaking the chain of transmission and edging the world closer to polio eradication.
A comparative analysis highlights IPV’s superiority in certain contexts. Unlike the oral polio vaccine (OPV), which uses live attenuated virus and carries a rare risk of vaccine-derived poliovirus, IPV eliminates this concern entirely. While OPV is cheaper and easier to administer, IPV is the preferred choice in polio-free regions to prevent reintroduction of the virus. This distinction underscores the strategic use of IPV in the endgame of polio eradication. For instance, countries transitioning from OPV to IPV as part of the Global Polio Eradication Initiative have seen sustained immunity without the risks of vaccine-associated paralytic polio. This shift exemplifies how IPV’s effectiveness is tailored to the evolving needs of global health strategies.
Persuasively, the data speaks for itself: IPV’s 99% reduction in polio cases is not just a number but a lifeline for millions. In India, for example, the introduction of IPV alongside OPV in 2016 strengthened immunity and accelerated the country’s polio-free status. Similarly, in Africa, IPV has been instrumental in maintaining eradication gains, even in conflict-affected areas. Critics might argue that IPV’s higher cost and injection requirement pose barriers, but its long-term benefits far outweigh these challenges. By preventing paralysis and death, IPV saves healthcare systems billions in treatment costs and improves quality of life for entire populations. Its effectiveness is not just a medical achievement but a moral imperative to protect future generations.
Finally, a descriptive lens reveals the human impact of IPV’s effectiveness. Imagine a world where polio is a relic of the past, where children no longer face the specter of paralysis. IPV has made this vision a reality in most countries, thanks to its ability to provide long-term protection. From urban clinics to remote villages, the vaccine’s reach has been transformative. A mother in Nigeria, for instance, can now raise her child without the fear of polio, thanks to IPV’s inclusion in routine immunization programs. This peace of mind is the ultimate measure of the vaccine’s success. As the world inches closer to eradication, IPV’s role as a guardian of health and hope cannot be overstated. Its effectiveness is not just in numbers but in the lives it saves and the futures it secures.
Skipping Second Varicella Shot: Risks, Complications, and Prevention Strategies
You may want to see also
Explore related products



![]()
Side Effects: Mild reactions include soreness, fever, or allergic responses, rarely severe complications
The inactivated poliovirus vaccine (IPV) is a cornerstone of global efforts to eradicate polio, offering robust protection against this once-feared disease. Like any medical intervention, it comes with potential side effects, though these are generally mild and manageable. Understanding these reactions is crucial for informed decision-making and peace of mind.
Mild reactions to IPV are common and typically resolve within a few days. Soreness, redness, or swelling at the injection site is the most frequent complaint, affecting up to 1 in 4 recipients. A low-grade fever (around 100°F or 37.8°C) may also occur, particularly in children under 5. These symptoms are the body’s natural response to the vaccine, signaling the immune system’s activation. Over-the-counter pain relievers like acetaminophen can alleviate discomfort, but aspirin should be avoided in children due to the risk of Reye’s syndrome.
Allergic responses to IPV are rare but warrant attention. Symptoms may include hives, itching, or mild rash, typically appearing within minutes to hours after vaccination. Severe allergic reactions, such as difficulty breathing or swelling of the face and throat, are extremely uncommon, occurring in fewer than 1 in a million doses. Individuals with a history of severe allergies to vaccine components, such as neomycin or streptomycin, should consult a healthcare provider before receiving IPV.
Severe complications from IPV are virtually unheard of, as the vaccine contains inactivated (killed) virus particles that cannot cause polio. Unlike the oral polio vaccine (OPV), which uses a weakened live virus, IPV carries no risk of vaccine-derived poliovirus. However, as with any injection, there is a minimal risk of infection at the injection site if proper sterilization techniques are not followed. Ensuring vaccination is administered by trained professionals in clean settings mitigates this risk.
Practical tips can enhance the vaccination experience. Scheduling IPV doses during cooler parts of the day may reduce fever discomfort. Applying a cool, damp cloth to the injection site can soothe soreness. For children, distraction techniques—such as singing or offering a favorite toy—can ease anxiety during administration. Parents should monitor their child for unusual symptoms post-vaccination and report any concerns to a healthcare provider promptly.
In summary, while IPV side effects are typically mild and transient, awareness and preparedness can further smooth the vaccination process. The vaccine’s unparalleled safety profile and efficacy in preventing polio far outweigh the minimal risks, making it a vital tool in public health.
Live Virus Vaccines: Impact on IGRA Test Accuracy Explained
You may want to see also
Frequently asked questions
The inactivated poliovirus vaccine (IPV) is a vaccine used to prevent poliomyelitis (polio). It contains inactivated (killed) poliovirus strains of all three types, making it safe and effective for immunization.
The IPV works by introducing inactivated poliovirus particles into the body, which stimulate the immune system to produce antibodies. These antibodies protect against infection if the individual is later exposed to the live poliovirus.
The IPV is recommended for infants, children, and adults as part of routine immunization schedules. It is also used in polio eradication efforts and for travelers to regions where polio is still endemic.
The IPV is generally safe, with minimal side effects. Common reactions include mild soreness at the injection site, low-grade fever, or irritability. Serious side effects are extremely rare.