The IPV vaccine, also known as the Inactivated Poliovirus Vaccine, is a crucial immunization tool used to prevent poliomyelitis, a highly contagious viral disease that can lead to paralysis and even death. Unlike the oral polio vaccine (OPV), which contains a weakened form of the virus, IPV is composed of inactivated (killed) poliovirus strains, making it safer for individuals with weakened immune systems. Administered through injection, IPV is widely used in many countries as part of routine childhood vaccination programs and has played a significant role in the global effort to eradicate polio. Its effectiveness and safety profile have made it a preferred choice in regions where the risk of vaccine-derived poliovirus is a concern.
Explore related products






What You'll Learn
- IPV Vaccine Full Name: Inactivated Polio Vaccine (IPV) is the formal name for the injectable polio vaccine
- IPV vs. OPV: IPV differs from Oral Polio Vaccine (OPV) in administration and virus type
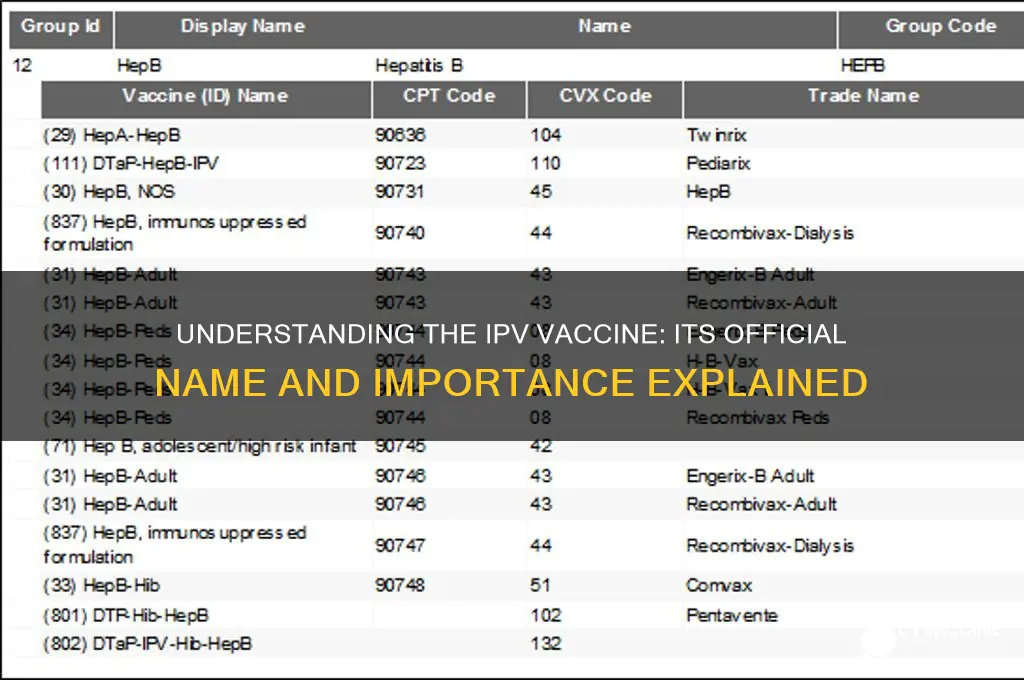
- IPV Brands: Common IPV brands include Ipol, Imovax Polio, and Pediacel
- IPV Schedule: Typically given in 3-4 doses during infancy and early childhood
- IPV Safety: IPV is safe, cannot cause polio, and has minimal side effects
![]()
IPV Vaccine Full Name: Inactivated Polio Vaccine (IPV) is the formal name for the injectable polio vaccine
The IPV vaccine, formally known as the Inactivated Polio Vaccine, is a critical tool in the global effort to eradicate polio. Unlike the oral polio vaccine (OPV), which uses a weakened form of the virus, IPV contains inactivated (killed) poliovirus. This key difference makes IPV safer for individuals with weakened immune systems, as it cannot revert to a virulent form and cause vaccine-derived polio. Administered through injection, typically in the leg or arm, IPV is recommended for children and adults in regions where polio remains a risk or for travelers to such areas. The vaccine is usually given in a series of doses, starting at 2 months of age, with boosters at 4 months, 6-18 months, and 4-6 years, ensuring long-term immunity.
From a practical standpoint, understanding the IPV vaccine’s full name clarifies its mechanism and purpose. The term "inactivated" emphasizes that the virus is dead and incapable of causing disease, making it a safer option for certain populations. For instance, pregnant women, immunocompromised individuals, and those with specific medical conditions are often advised to receive IPV instead of OPV. Healthcare providers must adhere to strict dosage guidelines: 0.5 mL for children under 7 years and 0.5 mL for older children and adults. Proper storage at 2°C to 8°C is essential to maintain the vaccine’s efficacy, and it should never be frozen.
Comparatively, while OPV offers the advantage of inducing intestinal immunity and stopping viral shedding, IPV’s safety profile makes it the preferred choice in polio-free countries. For example, the United States transitioned exclusively to IPV in 2000 to eliminate the rare risk of vaccine-associated paralytic polio (VAPP) linked to OPV. This shift underscores the importance of tailoring vaccination strategies to regional needs. In countries where polio is endemic, a combination of OPV and IPV may be used to maximize protection while minimizing risks.
Persuasively, the IPV vaccine’s formal name highlights its role as a cornerstone of polio prevention in modern medicine. Its inactivated nature ensures that it cannot cause polio, a critical factor in building public trust in vaccination programs. Parents and caregivers should be educated about the vaccine’s safety and efficacy, dispelling myths and encouraging adherence to immunization schedules. Additionally, travelers to polio-affected regions must receive IPV as part of their pre-travel health preparations, often requiring a booster dose if their last vaccination was over 10 years ago.
Descriptively, the IPV vaccine is a clear, colorless liquid administered via intramuscular or subcutaneous injection, depending on the recipient’s age and health status. Its formulation includes trace amounts of formaldehyde (used to inactivate the virus) and stabilizing agents like lactose or sucrose. While side effects are generally mild—such as soreness at the injection site, fever, or irritability—they are far outweighed by the vaccine’s benefits. For healthcare workers, proper technique is crucial: using the correct needle size, ensuring the injection site is clean, and disposing of sharps safely are all essential steps in administering IPV effectively.
Whooping Cough Vaccine Availability at Kroger: What You Need to Know
You may want to see also
Explore related products




![]()
IPV vs. OPV: IPV differs from Oral Polio Vaccine (OPV) in administration and virus type
The inactivated poliovirus vaccine (IPV) and the oral poliovirus vaccine (OPV) are two distinct tools in the fight against polio, each with unique characteristics that influence their use in global eradication efforts. While both aim to prevent poliomyelitis, their differences in administration, virus type, and immune response are critical to understanding their roles.
Administration and Dosage: IPV is administered through an injection, typically into the muscle (intramuscular) or just under the skin (subcutaneous). The standard schedule for IPV in many countries includes a primary series of 3–4 doses, starting at 2 months of age, followed by booster shots. For instance, the Centers for Disease Control and Prevention (CDC) recommends a series of 4 doses at 2 months, 4 months, 6–18 months, and 4–6 years. In contrast, OPV is delivered orally, often in the form of drops, making it easier to administer, especially in mass vaccination campaigns. The oral vaccine usually requires multiple doses, with the World Health Organization (WHO) recommending at least 3 doses for infants, starting at 6 weeks of age, followed by additional doses in subsequent years.
Virus Type and Immune Response: The key distinction lies in the virus type used. IPV contains inactivated (killed) poliovirus, ensuring it cannot cause paralysis. This vaccine primarily induces humoral immunity, leading to the production of antibodies in the bloodstream, which can prevent the virus from infecting the central nervous system. On the other hand, OPV uses a live, attenuated (weakened) virus. When administered, it replicates in the intestine, providing both humoral and mucosal immunity. This dual response not only protects against paralysis but also reduces the shedding and transmission of wild poliovirus, making OPV a powerful tool for interrupting polio circulation in communities.
Practical Considerations: The choice between IPV and OPV depends on various factors. IPV is preferred in regions where polio has been eliminated due to its inability to cause vaccine-associated paralytic polio (VAPP), a rare side effect of OPV. However, OPV's ease of administration and its ability to provide intestinal immunity make it invaluable in polio-endemic areas. In some countries, a combination of both vaccines is used, starting with OPV to rapidly induce mucosal immunity and following up with IPV to boost antibody levels. This sequential approach aims to maximize protection while minimizing risks.
Global Impact and Future Directions: The strategic use of IPV and OPV has been instrumental in the near-eradication of polio. As of 2023, wild poliovirus remains endemic in only a few countries. The Global Polio Eradication Initiative (GPEI) has been pivotal in this effort, coordinating vaccination campaigns and surveillance. The transition from trivalent OPV to bivalent OPV, and the introduction of IPV in routine immunization schedules, reflects the evolving strategies to address the challenges of polio eradication. As the world moves closer to a polio-free future, the careful selection and deployment of these vaccines will remain crucial.
In summary, while IPV and OPV share the common goal of polio prevention, their differences in administration, virus type, and immune response make them complementary tools in the global health arsenal. Understanding these distinctions is essential for healthcare providers, policymakers, and the public to ensure the effective use of these vaccines in the final push towards polio eradication.
Jenny McCarthy's Vaccine Views: A Change of Heart?
You may want to see also
Explore related products






![]()
IPV Brands: Common IPV brands include Ipol, Imovax Polio, and Pediacel
The inactivated poliovirus vaccine (IPV) is a critical tool in the global effort to eradicate polio, and several brands have been developed to meet this need. Among the most recognized are Ipol, Imovax Polio, and Pediacel, each with distinct characteristics tailored to different populations and healthcare settings. Understanding these brands is essential for healthcare providers and parents alike, as they play a pivotal role in ensuring effective immunization.
Ipol is a standalone IPV vaccine manufactured by Sanofi Pasteur. It is typically administered as a series of four doses, starting at 2 months of age, with subsequent doses given at 4 months, 6-18 months, and 4-6 years. This schedule ensures robust immunity against all three poliovirus types. Ipol is particularly favored in regions transitioning from oral polio vaccine (OPV) to IPV, as it provides a safe and effective alternative without the risk of vaccine-derived poliovirus (VDPV). Its single-antigen formulation makes it ideal for focused polio prevention.
Imovax Polio, also produced by Sanofi Pasteur, is another widely used IPV brand. Similar to Ipol, it is administered in a four-dose series but is often used in combination with other vaccines in certain countries. This brand is known for its stability and ease of storage, making it suitable for use in resource-limited settings. Healthcare providers appreciate its reliability, especially in mass vaccination campaigns where consistency is key.
Pediacel, on the other hand, is a combination vaccine that includes IPV alongside protection against diphtheria, tetanus, pertussis, and *Haemophilus influenzae* type b (DTaP-IPV-Hib). This all-in-one approach reduces the number of injections required for infants, making it a convenient option for parents and healthcare providers. Pediacel is typically given in a three-dose series at 2, 4, and 6 months of age, followed by a booster dose between 15-18 months. Its multi-antigen formulation streamlines immunization schedules, ensuring broader protection with fewer clinic visits.
When selecting an IPV brand, healthcare providers must consider factors such as patient age, vaccine availability, and regional polio prevalence. For instance, Ipol and Imovax Polio are preferred in areas where polio remains endemic, while Pediacel is ideal for regions with established polio eradication but a need for comprehensive childhood immunization. Parents should consult their healthcare provider to determine the most appropriate vaccine for their child, ensuring timely and effective protection against this debilitating disease.
In summary, Ipol, Imovax Polio, and Pediacel are cornerstone IPV brands, each designed to meet specific immunization needs. Their distinct formulations and administration schedules make them versatile tools in the fight against polio, offering tailored solutions for diverse healthcare landscapes. By understanding these brands, stakeholders can make informed decisions to safeguard public health effectively.
Understanding Zostavax Vaccine Costs: A Comprehensive Pricing Guide
You may want to see also
Explore related products


![]()
IPV Schedule: Typically given in 3-4 doses during infancy and early childhood
The IPV vaccine, known as the Inactivated Poliovirus Vaccine, is a critical tool in the global effort to eradicate polio. Its schedule is meticulously designed to provide robust immunity during the most vulnerable stages of life. Typically administered in 3-4 doses during infancy and early childhood, this regimen ensures that children develop strong protection against poliovirus before they are likely to encounter it. The first dose is usually given at 2 months of age, followed by subsequent doses at 4 months and 6-18 months, with a booster sometimes recommended between 4-6 years. This staggered approach allows the immune system to build and reinforce its defenses effectively.
From an analytical perspective, the IPV schedule reflects a balance between maximizing immunity and minimizing the risk of side effects. Unlike the oral polio vaccine (OPV), which uses a weakened live virus, IPV contains inactivated virus particles, making it safer for immunocompromised individuals and eliminating the rare risk of vaccine-derived poliovirus. The timing of doses is crucial because infants are born with passive immunity from their mothers, which wanes over the first few months. By starting vaccination at 2 months, the first dose begins to build active immunity just as maternal antibodies are declining, ensuring continuous protection.
For parents and caregivers, adhering to the IPV schedule requires careful planning and awareness. Missing a dose can delay the development of full immunity, leaving the child vulnerable. Practical tips include setting reminders for vaccination appointments, keeping a record of doses received, and consulting healthcare providers if there are concerns about timing or side effects. It’s also important to note that IPV is often administered as part of combination vaccines, such as DTaP-IPV-Hib, which protects against multiple diseases simultaneously, streamlining the immunization process.
Comparatively, the IPV schedule contrasts with that of OPV, which is administered orally and typically given in more frequent doses. While OPV has been instrumental in polio eradication efforts, particularly in low-resource settings, IPV is favored in regions where polio is no longer endemic due to its safety profile. The shift from OPV to IPV in many countries underscores the evolving strategies in vaccination programs, prioritizing long-term safety without compromising efficacy. This transition highlights the importance of tailoring vaccine schedules to local epidemiological contexts.
In conclusion, the IPV schedule is a cornerstone of polio prevention, offering a safe and effective way to protect children from a once-devastating disease. By understanding the rationale behind the timing and dosage, parents and healthcare providers can ensure that children receive the full benefits of this vaccine. As global health initiatives continue to push toward polio eradication, adherence to the IPV schedule remains a vital component of this effort, safeguarding future generations from the threat of poliovirus.
Essential Vaccinations for a Healthy Pregnancy: Expert Recommendations
You may want to see also
![]()
IPV Safety: IPV is safe, cannot cause polio, and has minimal side effects
The inactivated poliovirus vaccine (IPV) stands as a cornerstone in the global eradication of polio, a once-feared disease now on the brink of extinction. Unlike the oral polio vaccine (OPV), which contains a weakened form of the virus, IPV is crafted from inactivated (killed) poliovirus, rendering it incapable of causing polio. This fundamental difference ensures that IPV is not only safe but also eliminates the rare risk of vaccine-derived poliovirus associated with OPV. Administered through injection, typically in the leg or arm, IPV is recommended for children in a series of doses starting at 2 months of age, with boosters at 4 months, 6-18 months, and 4-6 years. This schedule ensures robust immunity without the risk of infection from the vaccine itself.
From a safety perspective, IPV’s track record is impeccable. Extensive clinical trials and decades of global use have confirmed its minimal side effects, which are generally mild and short-lived. Common reactions include soreness at the injection site, mild fever, or irritability, affecting less than 1 in 10 recipients. Severe allergic reactions are exceedingly rare, occurring in approximately 1 in a million doses. For parents and caregivers, this profile offers peace of mind, especially when compared to the devastating effects of polio, which can cause paralysis or death. The vaccine’s safety is further underscored by its approval for use in immunocompromised individuals, a group for whom live vaccines like OPV are contraindicated.
A comparative analysis highlights IPV’s advantages over OPV, particularly in regions nearing polio eradication. While OPV’s ease of administration (oral drops) made it ideal for mass campaigns, its rare ability to revert to a virulent form posed a risk in areas with high vaccination coverage. IPV, by contrast, provides individual protection without contributing to environmental virus circulation. This makes it the preferred choice in countries transitioning from OPV to a safer, more controlled immunization strategy. For travelers to polio-endemic regions, a single booster dose of IPV is often recommended, ensuring immunity without the risks associated with live vaccines.
Practical considerations for IPV administration include proper storage and handling to maintain vaccine efficacy. The vaccine should be stored between 2°C and 8°C and protected from light. Healthcare providers must adhere to strict aseptic techniques during injection to prevent contamination. For parents, ensuring children complete the full vaccination series is critical, as partial immunity leaves them vulnerable. Missed doses can be administered at any time, with no need to restart the series. In the rare event of a severe reaction, immediate medical attention is advised, though such instances are exceptionally uncommon.
In conclusion, IPV’s safety profile, inability to cause polio, and minimal side effects make it a vital tool in the fight against this crippling disease. Its inactivated nature ensures it poses no risk of infection, even to those with weakened immune systems. By adhering to recommended dosages and schedules, individuals and communities can achieve robust immunity, bringing the world closer to a polio-free future. For anyone questioning the safety of vaccines, IPV stands as a testament to the rigor and success of modern immunization science.
Discovering India's COVID-19 Vaccine: Covaxin and Covishield Explained
You may want to see also
Frequently asked questions
The IPV vaccine is called the Inactivated Poliovirus Vaccine.
Yes, the IPV vaccine is commonly referred to as the polio shot or polio vaccine, as it protects against poliomyelitis (polio).
While the scientific name remains Inactivated Poliovirus Vaccine (IPV), it may be marketed under various brand names depending on the manufacturer and region, such as Ipol or Imovax Polio.