A vaccine, in the context of biology, is a biological preparation that provides active, acquired immunity to a particular infectious disease. It typically contains a weakened or inactivated form of the disease-causing pathogen, such as a virus or bacterium, or specific components of the pathogen, like proteins or sugars. When administered, the vaccine stimulates the immune system to recognize and produce antibodies against the pathogen, creating a memory response. This immune memory allows the body to mount a faster and more effective defense if exposed to the actual pathogen in the future, thereby preventing or reducing the severity of the disease. Vaccines are a cornerstone of public health, playing a critical role in preventing the spread of infectious diseases and reducing mortality rates globally.
| Characteristics | Values |
|---|---|
| Definition | A biological preparation that provides active acquired immunity to a particular infectious disease. |
| Purpose | To stimulate the immune system to recognize and combat pathogens, either by preventing infection or reducing disease severity. |
| Composition | Contains antigens (weakened/killed pathogens, toxins, or parts of pathogens) and sometimes adjuvants to enhance immune response. |
| Administration | Typically delivered via injection, orally, or nasally. |
| Types | Live-attenuated, inactivated, subunit/recombinant, mRNA, viral vector, toxoid, conjugate. |
| Immune Response | Induces production of antibodies, memory cells, and other immune components specific to the pathogen. |
| Efficacy | Effectiveness varies by vaccine and individual; measured by reduction in disease incidence or severity. |
| Safety | Rigorously tested for safety and monitored post-approval; side effects are generally mild and rare. |
| Herd Immunity | Protects communities by reducing pathogen spread when a large portion of the population is vaccinated. |
| Examples | COVID-19, influenza, measles, mumps, rubella (MMR), polio, tetanus, diphtheria, pertussis (DTaP). |
Explore related products





What You'll Learn
- Vaccine Composition: Contains antigens, adjuvants, and stabilizers to stimulate immune response and ensure efficacy
- Immune Response: Triggers production of antibodies and memory cells for future pathogen protection
- Types of Vaccines: Includes live-attenuated, inactivated, mRNA, subunit, and viral vector vaccines
- Vaccine Development: Involves research, clinical trials, and regulatory approval for safety and effectiveness
- Vaccine Efficacy: Measures ability to prevent disease, reduce severity, and provide long-term immunity
![]()
Vaccine Composition: Contains antigens, adjuvants, and stabilizers to stimulate immune response and ensure efficacy
Vaccines are biological preparations that prime the immune system to recognize and combat pathogens, such as viruses or bacteria. At their core, vaccines contain antigens—molecules derived from or resembling the pathogen—that trigger an immune response without causing disease. However, antigens alone are often insufficient to elicit a robust and lasting immunity. This is where adjuvants come into play. Adjuvants are substances added to vaccines to enhance the immune system’s response to the antigen, ensuring that the body produces enough antibodies and memory cells for future protection. Stabilizers, another critical component, are included to maintain the vaccine’s potency during storage and transportation, particularly in varying environmental conditions. Together, these elements form a carefully calibrated composition designed to maximize efficacy while ensuring safety.
Consider the influenza vaccine, a seasonal staple in preventive healthcare. Its composition typically includes inactivated viral antigens specific to the strains predicted to circulate that year. To amplify the immune response, adjuvants like aluminum salts (e.g., aluminum hydroxide) are added, particularly in formulations for older adults whose immune systems may be less responsive. Stabilizers such as gelatin or sugars (e.g., sucrose) are also incorporated to protect the vaccine’s integrity, especially in multi-dose vials. For instance, the Fluzone High-Dose vaccine, recommended for adults over 65, contains a higher antigen concentration and adjuvant levels to compensate for age-related immune decline. This tailored composition underscores the importance of balancing antigen, adjuvant, and stabilizer ratios to meet specific population needs.
From a practical standpoint, understanding vaccine composition can inform administration and storage practices. For example, vaccines with aluminum-based adjuvants may cause mild local reactions, such as soreness at the injection site, but these are generally short-lived and outweighed by the benefits of enhanced immunity. Stabilizers like gelatin, while effective, can pose risks for individuals with rare allergies, necessitating alternative formulations. Storage requirements are equally critical; vaccines with sensitive stabilizers, such as those in live-attenuated vaccines (e.g., MMR), must be refrigerated at 2–8°C to prevent degradation. Healthcare providers must adhere to these guidelines to ensure vaccine efficacy, particularly in resource-limited settings where temperature fluctuations are common.
A comparative analysis of vaccine compositions reveals the evolution of design principles. Early vaccines, like the smallpox vaccine, relied solely on weakened or inactivated pathogens, with no additional components. Modern vaccines, however, are engineered with precision, incorporating adjuvants and stabilizers to address specific challenges. For instance, mRNA vaccines, such as Pfizer-BioNTech’s COVID-19 vaccine, use lipid nanoparticles as both a delivery system and an adjuvant, stimulating a potent immune response without traditional additives. In contrast, subunit vaccines, like the hepatitis B vaccine, contain purified antigen proteins and aluminum adjuvants, offering targeted immunity with minimal side effects. These innovations highlight the adaptability of vaccine composition to meet diverse immunological and logistical demands.
In conclusion, the interplay of antigens, adjuvants, and stabilizers defines the effectiveness and reliability of vaccines. Antigens provide the immune system with a target, adjuvants amplify the response, and stabilizers ensure longevity. This tripartite composition is not one-size-fits-all; it is meticulously tailored to the pathogen, population, and delivery context. For instance, pediatric vaccines often include higher antigen doses and milder adjuvants to accommodate developing immune systems, while travel vaccines may prioritize stability for use in remote areas. By understanding these components, healthcare professionals and the public can better appreciate the science behind vaccination and the importance of adhering to recommended schedules and storage protocols. This knowledge empowers informed decision-making, fostering trust in one of medicine’s most transformative tools.
Measuring Vaccine Effectiveness: A Comprehensive Guide to Efficacy Calculation
You may want to see also
Explore related products





![]()
Immune Response: Triggers production of antibodies and memory cells for future pathogen protection
Vaccines are biological preparations that stimulate the immune system to recognize and combat pathogens, such as viruses or bacteria, without causing the disease itself. Central to their function is the activation of the immune response, a complex process designed to protect the body from harmful invaders. When a vaccine is administered, it introduces a harmless form of the pathogen—whether inactivated, weakened, or a fragment—to the immune system. This triggers a cascade of events that culminate in the production of antibodies and memory cells, the body’s defense arsenal for future encounters with the same pathogen.
Consider the mechanism in action: upon vaccination, antigen-presenting cells (APCs) engulf the vaccine’s antigen and transport it to lymph nodes, where they activate naïve T cells and B cells. B cells differentiate into plasma cells, which secrete antibodies specific to the antigen. These antibodies neutralize pathogens by binding to them, preventing infection or marking them for destruction. Simultaneously, some B cells and T cells transform into memory cells, which persist long-term in the body. Memory cells are the immune system’s strategic reserve, enabling a faster and more robust response if the same pathogen is encountered again. This dual outcome—immediate antibody production and memory cell formation—is the cornerstone of vaccine efficacy.
For optimal immune response, vaccine dosage and timing are critical. For instance, the measles, mumps, and rubella (MMR) vaccine is typically administered in two doses: the first at 12–15 months of age and the second at 4–6 years. This schedule ensures sufficient antibody production and memory cell formation. Booster doses, such as those for tetanus (every 10 years), reinforce memory cell activity, maintaining immunity over time. Adhering to recommended schedules is essential, as deviations can compromise the immune response, leaving individuals vulnerable to infection.
Practical considerations also play a role in maximizing vaccine effectiveness. Age-specific guidelines, such as the influenza vaccine for individuals over six months, ensure safety and efficacy across different populations. Storage and administration techniques, like maintaining vaccines at 2–8°C, preserve their integrity. Additionally, avoiding immunosuppressive medications or conditions around vaccination can enhance the immune response. For example, individuals with compromised immune systems may require higher doses or alternative vaccine types to achieve adequate protection.
In summary, vaccines harness the immune system’s ability to produce antibodies and memory cells, providing a durable defense against pathogens. By understanding the interplay of dosage, timing, and practical factors, individuals and healthcare providers can optimize vaccine efficacy. This knowledge underscores the importance of vaccines not just as preventive tools, but as architects of long-term immunity, safeguarding health across populations.
Spike Proteins in J&J Vaccine: What You Need to Know
You may want to see also
Explore related products





![]()
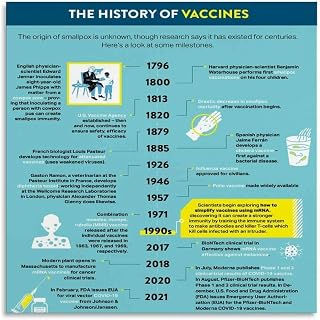
Types of Vaccines: Includes live-attenuated, inactivated, mRNA, subunit, and viral vector vaccines
Vaccines are biological preparations that stimulate the immune system to recognize and combat pathogens, preventing or reducing the severity of diseases. They achieve this by introducing a harmless form of a pathogen or its components, prompting the body to produce antibodies and memory cells for future protection. Among the diverse types of vaccines, each employs a distinct mechanism to confer immunity, tailored to the nature of the disease and the immune response required.
Live-attenuated vaccines use a weakened (attenuated) form of the live pathogen, incapable of causing severe disease but still able to induce a robust immune response. Examples include the measles, mumps, and rubella (MMR) vaccine and the varicella (chickenpox) vaccine. These vaccines typically require fewer doses—often just one or two—to provide long-lasting immunity. However, they are contraindicated for immunocompromised individuals due to the risk of the virus reverting to a virulent form. Storage at 2–8°C (36–46°F) is critical to maintain their efficacy, and they are generally administered to children over 12 months old, with boosters as needed.
Inactivated vaccines, in contrast, contain pathogens that have been killed through physical or chemical methods, rendering them unable to replicate. Examples include the polio (IPV) and hepatitis A vaccines. While these vaccines are safer for immunocompromised individuals, they often require multiple doses (e.g., three doses of IPV for infants at 2, 4, and 6–18 months) and adjuvants to enhance the immune response. Booster shots are frequently necessary to maintain immunity, as the response is generally less durable than with live-attenuated vaccines.
MRNA vaccines represent a groundbreaking approach, using messenger RNA to instruct cells to produce a harmless protein unique to the pathogen, triggering an immune response. The Pfizer-BioNTech and Moderna COVID-19 vaccines are prime examples. These vaccines are highly effective, with a two-dose regimen (typically 3–4 weeks apart) providing over 90% protection against severe disease. mRNA vaccines are stored at ultra-cold temperatures (–70°C for Pfizer, –20°C for Moderna) initially, though formulations stable at standard freezer temperatures are emerging. Their rapid development and scalability make them a promising platform for future vaccines.
Subunit vaccines contain specific pieces of a pathogen, such as proteins or sugars, rather than the entire organism. The hepatitis B and human papillomavirus (HPV) vaccines are notable examples. These vaccines are highly safe, as they cannot cause the disease, and are often administered in a series of two or three doses. Adjuvants are commonly added to boost the immune response. Subunit vaccines are ideal for individuals with weakened immune systems and are frequently used in pediatric and adult populations alike.
Viral vector vaccines employ a harmless virus (the vector) to deliver genetic material encoding a pathogen’s antigen into cells. The Johnson & Johnson COVID-19 vaccine and the Ebola vaccine (Ervebo) use this technology. A single dose is often sufficient, making them logistically advantageous, particularly in low-resource settings. However, rare side effects, such as thrombosis with thrombocytopenia syndrome (TTS), have been reported, necessitating careful patient screening. Storage at standard refrigerator temperatures (2–8°C) enhances their accessibility for global distribution.
Each vaccine type offers unique advantages and considerations, tailored to the pathogen and population served. Understanding these differences empowers healthcare providers and individuals to make informed decisions, ensuring optimal protection against infectious diseases.
Understanding Meningitis Vaccines: Exploring the Different Types Available
You may want to see also
Explore related products






![]()
Vaccine Development: Involves research, clinical trials, and regulatory approval for safety and effectiveness
Vaccine development is a rigorous, multi-stage process that ensures safety and efficacy before a product reaches the public. It begins with preclinical research, where scientists identify a target pathogen and explore potential vaccine candidates. This phase often involves animal testing to assess initial safety and immune response. For instance, the mRNA technology behind COVID-19 vaccines was first tested in mice to confirm its ability to elicit antibodies against the SARS-CoV-2 spike protein. This stage is critical for narrowing down the most promising candidates before advancing to human trials.
Once a candidate is selected, clinical trials commence, typically in three phases. Phase 1 trials involve a small group of healthy volunteers (20–100 individuals) to evaluate safety, dosage, and immune response. Dosages are carefully calibrated, often starting with microgram quantities (e.g., 30 µg for the Pfizer-BioNTech COVID-19 vaccine) to minimize risks. Phase 2 expands to several hundred participants, focusing on efficacy and side effects in specific populations, such as children or the elderly. Finally, Phase 3 involves thousands of participants to confirm effectiveness and monitor rare side effects. For example, the Moderna COVID-19 vaccine’s Phase 3 trial included 30,000 participants, demonstrating 94% efficacy in preventing symptomatic infection.
Regulatory approval is the final hurdle, where agencies like the FDA or EMA scrutinize trial data to ensure the vaccine meets stringent safety and efficacy standards. This process includes inspections of manufacturing facilities to verify consistency and quality. Post-approval, phase 4 monitoring continues to track long-term effects and rare adverse events in the general population. For instance, the CDC’s Vaccine Adverse Event Reporting System (VAERS) allows healthcare providers and the public to report side effects, ensuring ongoing safety.
Practical considerations during development include storage and distribution, especially for vaccines requiring ultra-cold temperatures (e.g., -70°C for Pfizer’s mRNA vaccine). Developers must also address global accessibility, balancing cost and scalability to ensure equitable distribution. For example, the COVAX initiative aimed to provide COVID-19 vaccines to low-income countries, highlighting the importance of international collaboration in vaccine deployment.
In summary, vaccine development is a complex, collaborative effort requiring scientific innovation, meticulous testing, and regulatory oversight. Each step, from lab research to post-market surveillance, is designed to protect public health while addressing practical challenges like dosage precision, age-specific needs, and global distribution. This process ensures that vaccines, such as those for influenza, measles, or COVID-19, are both safe and effective for widespread use.
CDC-Recommended Hepatitis B Vaccine Schedule: Timing and Spacing Explained
You may want to see also
Explore related products






![]()
Vaccine Efficacy: Measures ability to prevent disease, reduce severity, and provide long-term immunity
Vaccine efficacy is a critical metric that quantifies how well a vaccine performs in real-world settings. It is measured through clinical trials and population studies, where vaccinated groups are compared to unvaccinated or placebo groups. For instance, the Pfizer-BioNTech COVID-19 vaccine demonstrated 95% efficacy in preventing symptomatic disease in its Phase 3 trial, meaning vaccinated individuals were 95% less likely to develop COVID-19 compared to those who received a placebo. This figure is not just a number; it reflects the vaccine’s ability to interrupt disease transmission and protect individuals at scale. Efficacy rates vary by vaccine type and target disease, with some vaccines, like the measles vaccine, achieving near-perfect efficacy of 97% after two doses.
One of the key aspects of vaccine efficacy is its role in reducing disease severity, even when infection occurs. Vaccines train the immune system to recognize and combat pathogens, often leading to milder symptoms if breakthrough infections happen. For example, during the COVID-19 pandemic, vaccinated individuals were significantly less likely to require hospitalization or intensive care compared to the unvaccinated. This reduction in severity not only saves lives but also alleviates strain on healthcare systems. Similarly, the annual influenza vaccine, though its efficacy ranges from 40% to 60%, consistently lowers the risk of severe illness, particularly in high-risk groups like the elderly and immunocompromised.
Long-term immunity is another cornerstone of vaccine efficacy, though it varies widely depending on the vaccine and disease. Some vaccines, like those for hepatitis B or measles, provide lifelong immunity after a complete series, often requiring no boosters. Others, such as the tetanus vaccine, necessitate periodic boosters every 10 years to maintain protection. COVID-19 vaccines have introduced a new challenge, as their efficacy against infection wanes over time, particularly against emerging variants. Booster doses, typically administered 6 to 12 months after the initial series, have proven effective in restoring immunity and extending protection. Understanding these timelines is crucial for public health planning and individual decision-making.
Practical considerations for maximizing vaccine efficacy include adhering to recommended dosages and schedules. For children, vaccines like the MMR (measles, mumps, rubella) are administered in two doses, with the first at 12–15 months and the second at 4–6 years. Adults must stay current with boosters, such as the Tdap vaccine (tetanus, diphtheria, pertussis), which is recommended every 10 years. Storage and handling also play a role; vaccines must be kept at specific temperatures (e.g., 2°C–8°C for most) to maintain potency. For travelers, vaccines like yellow fever require a single dose at least 10 days before entering endemic areas, providing lifelong immunity. These details underscore the importance of following guidelines to ensure vaccines work as intended.
Finally, vaccine efficacy is not just an individual benefit but a collective one. High vaccination rates contribute to herd immunity, protecting those who cannot be vaccinated due to medical reasons. For example, the polio vaccine has nearly eradicated the disease globally, with cases dropping by over 99% since 1988. However, efficacy can be undermined by vaccine hesitancy or misinformation, as seen in recent measles outbreaks in communities with low vaccination rates. Public health campaigns must emphasize not only the personal benefits of vaccines but also their role in safeguarding entire populations. By understanding and communicating vaccine efficacy effectively, societies can build trust and ensure these tools reach their full potential.
Fond du Lac Humane Society: Vaccinations and More
You may want to see also
Frequently asked questions
A vaccine is a biological preparation that provides active, acquired immunity to a particular infectious disease. It typically contains a weakened or inactivated form of the disease-causing pathogen (such as a virus or bacterium) or its toxins, stimulating the immune system to recognize and combat the pathogen without causing the disease.
A vaccine works by introducing a harmless form of a pathogen or its components into the body, which triggers the immune system to produce antibodies and memory cells. This prepares the immune system to quickly recognize and neutralize the actual pathogen if it encounters it in the future, preventing or reducing the severity of the disease.
The main types of vaccines include live-attenuated vaccines (weakened pathogens), inactivated vaccines (killed pathogens), subunit vaccines (specific pathogen parts), mRNA vaccines (genetic material to produce antigens), and toxoid vaccines (inactivated toxins). Each type works differently to stimulate immunity.
Vaccines are a cornerstone of public health because they prevent the spread of infectious diseases, reduce morbidity and mortality, and contribute to herd immunity. By protecting individuals and communities, vaccines have eradicated or controlled diseases like smallpox, polio, and measles, making them essential tools in global health efforts.