Vaccinations for small children are a critical component of public health, providing protection against serious and potentially life-threatening diseases. The current schedule for childhood immunizations is designed to ensure that children receive vaccines at the optimal times to maximize their effectiveness and safety. Typically, the schedule begins shortly after birth, with the first doses of vaccines like hepatitis B, followed by a series of immunizations in the first year, including DTaP (diphtheria, tetanus, and pertussis), Hib (Haemophilus influenzae type b), PCV (pneumococcal conjugate vaccine), and IPV (inactivated poliovirus vaccine). Subsequent doses and additional vaccines, such as MMR (measles, mumps, and rubella), varicella (chickenpox), and hepatitis A, are administered during the toddler and preschool years. It is essential for parents and caregivers to follow the recommended schedule, as deviations can leave children vulnerable to preventable diseases. Always consult with a healthcare provider for the most up-to-date and region-specific vaccination guidelines.
Explore related products






What You'll Learn
- Recommended Vaccines by Age: List of vaccines for infants and toddlers, including timing and dosages
- Vaccine Schedule Changes: Updates to the current immunization schedule for young children
- Combination Vaccines: Overview of multi-disease vaccines available for small children
- Catch-Up Immunizations: Guidelines for missed doses and catch-up schedules for delayed vaccinations
- Vaccine Safety: Information on safety protocols and common side effects for childhood vaccines
![]()
Recommended Vaccines by Age: List of vaccines for infants and toddlers, including timing and dosages
Infants and toddlers receive a series of vaccinations during their first two years to protect against serious diseases. The Centers for Disease Control and Prevention (CDC) recommends a specific schedule to ensure timely immunity. At birth to 2 months, the first doses of the Hepatitis B (HepB) vaccine are administered, often in the hospital. This is followed by the first doses of the DTaP (Diphtheria, Tetanus, Pertussis), Hib (Haemophilus influenzae type b), IPV (Inactivated Polio Vaccine), PCV13 (Pneumococcal Conjugate Vaccine), and RV (Rotavirus) vaccines at 2 months. Each vaccine is given in precise dosages: DTaP (0.5 mL), Hib (0.5 mL), IPV (0.5 mL), PCV13 (0.5 mL), and RV (oral, 2.5 mL). Parents should ensure their child receives these vaccines on time, as delays can leave them vulnerable to preventable illnesses.
By 4 months, the second doses of DTaP, Hib, IPV, PCV13, and RV are due, reinforcing the immune response. At 6 months, the third doses of DTaP, Hib, and RV are administered, while PCV13 and IPV schedules may vary based on brand and provider recommendations. Notably, the Influenza (Flu) vaccine is introduced at 6 months, with an initial two doses given one month apart in the first year, followed by annual doses thereafter. This staggered approach ensures robust protection as the child’s immune system matures. Caregivers should monitor for mild side effects like fever or fussiness, which are normal and typically resolve within 24–48 hours.
Between 12 and 15 months, toddlers receive critical boosters and new vaccines. The MMR (Measles, Mumps, Rubella), Varicella (Chickenpox), and HepA (Hepatitis A) vaccines are introduced, each with specific dosages: MMR (0.5 mL), Varicella (0.5 mL), and HepA (0.5 mL). The Hib and PCV13 series conclude with final doses, depending on previous immunization history. This age range is also when the 4th dose of DTaP and IPV is given, ensuring continued protection. Parents should keep a detailed record of these vaccinations, as they are often required for school enrollment.
Practical tips for caregivers include scheduling appointments early in the day when children are well-rested and bringing a favorite toy or snack to comfort the child. For infants, breastfeeding during or after vaccination can help soothe them. Toddlers may benefit from simple explanations about the importance of vaccines, framed in a positive light. Adhering to the CDC’s recommended schedule not only safeguards individual children but also contributes to herd immunity, protecting vulnerable populations who cannot be vaccinated. Always consult a healthcare provider for personalized advice and to address any concerns about vaccine timing or dosages.
Rochester NY Vaccine Sign-Up Guide: Easy Steps to Register
You may want to see also
Explore related products






![]()
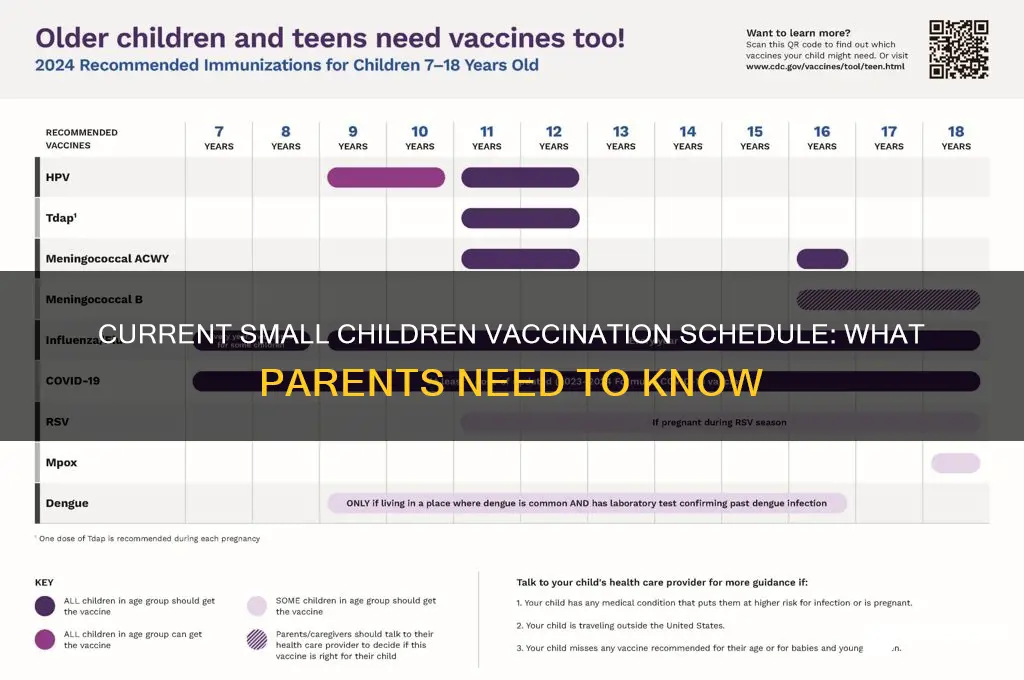
Vaccine Schedule Changes: Updates to the current immunization schedule for young children
The Centers for Disease Control and Prevention (CDC) recently updated the immunization schedule for young children, reflecting advancements in vaccine science and public health priorities. One notable change is the introduction of the COVID-19 vaccine for children as young as 6 months, administered in a lower dosage (3 micrograms for Pfizer, 25 micrograms for Moderna) compared to adult formulations. This addition underscores the evolving nature of vaccine schedules, which now address both longstanding and emerging infectious threats. Parents should consult their pediatrician to ensure their child’s vaccinations align with the latest recommendations, as timing and dosage specifics have been refined to optimize immunity and safety.
Another significant update involves the human papillomavirus (HPV) vaccine, which is now recommended for children starting at age 9, down from the previous starting age of 11 or 12. This change aims to maximize the vaccine’s effectiveness, as earlier administration can lead to a stronger immune response. The series consists of two doses for children under 15, spaced 6 to 12 months apart, compared to the three-dose regimen for older adolescents. This adjustment not only simplifies the schedule but also encourages earlier protection against HPV-related cancers. Parents should note that this vaccine is now framed as a routine part of pre-teen immunizations, alongside vaccines like Tdap and meningococcal.
The influenza vaccine remains an annual requirement but now includes clearer guidance on timing. Children aged 6 months through 8 years who are receiving the flu vaccine for the first time should get two doses, spaced at least four weeks apart. This ensures robust immunity in younger children, who are more susceptible to severe flu complications. The CDC emphasizes administering the first dose as soon as the vaccine becomes available, typically in July or August, to allow sufficient time for the second dose before flu season peaks. Parents should plan ahead to avoid delays, as protection takes about two weeks to develop after the final dose.
Lastly, the updated schedule highlights the importance of catch-up vaccinations for children who fall behind due to missed appointments or delays. For example, the measles, mumps, and rubella (MMR) vaccine, typically given at 12-15 months and 4-6 years, can now be administered with a minimum interval of 28 days between doses in catch-up scenarios. This flexibility ensures children can quickly get back on track without compromising immunity. Pediatricians are encouraged to use tools like immunization information systems to identify gaps and create personalized catch-up plans. For parents, staying proactive and maintaining open communication with healthcare providers is key to navigating these changes effectively.
Vaccination's Impact: Infant Mortality's Dramatic Decline
You may want to see also
Explore related products






![]()
Combination Vaccines: Overview of multi-disease vaccines available for small children
Combination vaccines streamline childhood immunization schedules by consolidating multiple disease protections into a single shot, reducing clinic visits and minimizing discomfort for young children. For instance, the DTaP-IPV-Hib vaccine, administered at 2, 3, and 4 months of age, shields against diphtheria, tetanus, pertussis, polio, and *Haemophilus influenzae* type b in one dose. This approach not only simplifies scheduling but also improves adherence, as parents are more likely to complete a less complex regimen. Pediatricians often recommend these combinations for their efficiency, ensuring children receive critical vaccines without overwhelming their developing immune systems.
One of the most widely used combination vaccines is the MMRV, which protects against measles, mumps, rubella, and varicella (chickenpox). Typically given as a single dose around 12–15 months, with a second dose between 4–6 years, it consolidates two separate vaccines into one injection. While MMRV offers convenience, healthcare providers caution about a slightly increased risk of fever-related seizures in young children compared to administering MMR and varicella vaccines separately. Parents should weigh this risk against the benefits of fewer injections and discuss concerns with their pediatrician.
Another notable combination is the Pentavalent vaccine, available in many countries, which covers diphtheria, tetanus, pertussis, hepatitis B, and *Haemophilus influenzae* type b. This vaccine is often given in a 3-dose series at 6, 10, and 14 weeks of age, followed by boosters. Its introduction has significantly reduced the number of injections infants receive in their first year, improving vaccine acceptance and coverage rates globally. However, availability varies by region, so parents should consult local health guidelines to confirm inclusion in their child’s schedule.
Combination vaccines also address practical challenges, such as storage and administration. For example, the Hexavalent vaccine, which adds polio protection to the Pentavalent formula, further reduces the number of shots required. This all-in-one approach is particularly beneficial in resource-limited settings, where frequent clinic visits may be impractical. Despite their advantages, combination vaccines undergo rigorous testing to ensure safety and efficacy, with studies confirming they elicit immune responses comparable to individual vaccines.
Incorporating combination vaccines into a child’s immunization plan requires careful consideration of timing and contraindications. Parents should adhere to the recommended schedule, as delaying doses can leave children vulnerable to preventable diseases. Practical tips include scheduling appointments early in the day to minimize disruptions and using distraction techniques, like singing or toys, during administration. By leveraging these multi-disease vaccines, caregivers can provide comprehensive protection while simplifying the vaccination process for their little ones.
Vaccine Differences: Europe and the US
You may want to see also
Explore related products






![]()
Catch-Up Immunizations: Guidelines for missed doses and catch-up schedules for delayed vaccinations
Life happens, and sometimes vaccinations get delayed. Whether due to illness, travel, or simply falling behind schedule, missed doses can leave parents worried about their child’s protection. Catch-up immunizations are designed to get children back on track, ensuring they receive the full benefit of vaccines even if they’ve fallen behind. The key is to act promptly and follow evidence-based guidelines tailored to the child’s age and the specific vaccine.
For infants and toddlers, catch-up schedules often involve accelerating the timing between doses while maintaining safety and efficacy. For example, if a child misses the 2-month dose of the DTaP (diphtheria, tetanus, pertussis) vaccine, the next dose can be administered as soon as 4 weeks later, rather than the standard 8 weeks. This principle applies to many vaccines, including IPV (polio), Hib (Haemophilus influenzae type b), and pneumococcal conjugate (PCV13). However, minimum intervals must be respected to avoid adverse reactions and ensure immune response. For instance, the minimum interval between doses of MMR (measles, mumps, rubella) is 4 weeks, though the recommended interval is 12 months for the second dose.
School-aged children who have missed vaccines face different considerations. For example, if a child misses the 4–6-year-old booster dose of DTaP, it can be given at any time thereafter, but the transition to Tdap (tetanus, diphtheria, pertussis) should occur at age 11–12. Similarly, if the second dose of varicella (chickenpox) vaccine is missed between ages 4–6, it can be administered at any time, even concurrently with other catch-up doses. The HPV vaccine, typically started at age 9–12, requires a catch-up schedule of 2 or 3 doses depending on the age at initiation—those starting before age 15 need 2 doses 6–12 months apart, while those 15 and older require 3 doses.
Practical tips can ease the catch-up process. First, consult a healthcare provider to create a personalized plan based on the child’s immunization history and current health. Utilize combination vaccines, such as Pentacel (DTaP, IPV, Hib), to minimize the number of injections needed. Keep a detailed record of all doses received, including dates and vaccine types, to avoid confusion. Finally, leverage tools like immunization information systems or smartphone apps to track progress and set reminders for upcoming doses.
Catch-up immunizations are a testament to the flexibility and adaptability of vaccination programs. While staying on schedule is ideal, missed doses do not mean starting over. With clear guidelines and proactive planning, children can achieve full immunity, protecting them from preventable diseases and contributing to community health. The goal is simple: ensure every child is up to date, no matter where they started.
Enrolling Your Child in School Without Vaccinations: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Vaccine Safety: Information on safety protocols and common side effects for childhood vaccines
Childhood vaccines undergo rigorous testing and monitoring to ensure their safety, a process that begins with laboratory research and progresses through multiple phases of clinical trials involving thousands of participants. Before approval, regulatory bodies like the FDA and CDC scrutinize data for efficacy and potential risks. Even after distribution, vaccines are continuously monitored through systems like the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) to detect rare or long-term side effects. This multi-layered approach ensures that vaccines meet stringent safety standards before they are administered to children.
Common side effects of childhood vaccines are typically mild and short-lived, serving as indicators that the immune system is responding as expected. For example, the MMR (Measles, Mumps, Rubella) vaccine may cause fever in about 1 in 6 children and a mild rash in 1 in 20. The DTaP (Diphtheria, Tetanus, Pertussis) vaccine can lead to soreness at the injection site in up to 1 in 4 children and low-grade fever in 1 in 16. These reactions usually resolve within 1–2 days and can be managed with over-the-counter pain relievers like acetaminophen, following the recommended dosage for the child’s age and weight. It’s essential to monitor children post-vaccination and consult a healthcare provider if symptoms persist or worsen.
Serious side effects from vaccines are extremely rare but are taken seriously when reported. For instance, severe allergic reactions (anaphylaxis) occur in approximately 1 in a million doses. Such reactions typically appear within minutes to hours after vaccination and require immediate medical attention. To mitigate risks, healthcare providers follow safety protocols, such as screening for allergies before administration and having emergency treatments like epinephrine readily available. Parents should inform providers of any history of severe allergies or previous vaccine reactions to ensure appropriate precautions are taken.
Practical tips can enhance the vaccination experience for both children and caregivers. Dressing infants in loose clothing for easy access to the thigh (the recommended injection site for babies) can streamline the process. For older children, distraction techniques like singing, storytelling, or bringing a favorite toy can reduce anxiety. After vaccination, encourage gentle movement of the vaccinated limb to ease soreness, and ensure the child stays hydrated. Keeping a record of vaccination dates and any observed reactions can also aid in future medical discussions and ensure adherence to the recommended schedule.
In summary, vaccine safety is upheld through meticulous testing, ongoing monitoring, and adherence to established protocols. While common side effects are mild and manageable, rare occurrences are addressed with swift medical intervention. By understanding these safety measures and preparing for vaccinations, parents can confidently protect their children from preventable diseases while minimizing discomfort. Always consult healthcare providers for personalized advice and to address specific concerns.
Fake Vaccines: Risks, Consequences, and Impact on Public Health
You may want to see also
Frequently asked questions
The current vaccination schedule for small children typically starts at birth and continues through early childhood. Key vaccines include Hepatitis B (at birth), Rotavirus, DTaP (Diphtheria, Tetanus, Pertussis), Hib (Haemophilus influenzae type b), Pneumococcal, Polio, and Influenza. The CDC and WHO provide detailed schedules, often with doses given at 2, 4, 6, and 12-15 months, followed by boosters.
As of 2023, minor updates may have been made to the vaccination schedule based on new research or vaccine availability. It’s recommended to consult the CDC’s or local health department’s guidelines for the most current schedule, as adjustments can occur annually.
While the standard schedule is designed for optimal protection, some flexibility exists for medical reasons or special circumstances. However, delaying vaccines increases the risk of preventable diseases. Always consult a healthcare provider before altering the recommended schedule.