An attenuated vaccine, also known as a live attenuated vaccine, is a type of vaccine that uses a weakened (attenuated) form of the live virus or bacteria to stimulate an immune response without causing the disease. Unlike inactivated vaccines, which use killed pathogens, attenuated vaccines contain organisms that have been modified to reduce their virulence while retaining their ability to induce a robust and long-lasting immune response. This approach mimics a natural infection, prompting the body to produce antibodies and memory cells that provide protection against future encounters with the actual pathogen. Commonly used attenuated vaccines include those for measles, mumps, rubella (MMR), varicella (chickenpox), and yellow fever. While highly effective, attenuated vaccines are generally not recommended for individuals with compromised immune systems due to the risk of the weakened pathogen causing illness.
| Characteristics | Values |
|---|---|
| Definition | A vaccine containing a live, weakened (attenuated) form of a virus or bacterium that triggers an immune response without causing the disease. |
| Mechanism | The attenuated pathogen replicates in the body, stimulating a strong immune response, including the production of antibodies and memory cells. |
| Immunity | Provides long-lasting immunity, often requiring fewer doses compared to inactivated vaccines. |
| Examples | Measles, Mumps, Rubella (MMR), Varicella (Chickenpox), Yellow Fever, Oral Polio Vaccine (OPV). |
| Advantages | Mimics natural infection, strong and durable immunity, often single-dose or fewer doses required. |
| Disadvantages | May not be suitable for immunocompromised individuals, rare risk of reversion to virulence, requires cold chain storage. |
| Stability | Less stable than inactivated vaccines, requiring refrigeration to maintain potency. |
| Administration | Typically administered orally, intranasally, or via injection, depending on the vaccine. |
| Safety | Generally safe, but may cause mild, vaccine-related symptoms (e.g., fever, rash) in some individuals. |
| Development | Developed through serial passage of the pathogen in cell culture or animal hosts to reduce its virulence. |
Explore related products






What You'll Learn
- Definition: Live, weakened pathogens unable to cause disease but trigger immune response
- Mechanism: Stimulates immunity by mimicking natural infection without severe symptoms
- Examples: Measles, mumps, rubella (MMR), varicella (chickenpox) vaccines
- Advantages: Long-lasting immunity, fewer doses needed, cost-effective
- Limitations: Requires refrigeration, potential risks for immunocompromised individuals
![]()
Definition: Live, weakened pathogens unable to cause disease but trigger immune response
Attenuated vaccines represent a cornerstone of modern immunology, leveraging live but weakened pathogens to safely prepare the immune system for future threats. Unlike inactivated vaccines, which use killed pathogens, attenuated vaccines contain organisms that have been modified to lose their disease-causing ability while retaining their immunogenicity. This delicate balance ensures the vaccine can replicate mildly in the body, stimulating a robust immune response without inducing illness. For instance, the measles, mumps, and rubella (MMR) vaccine uses attenuated viruses, administered as a single 0.5 mL dose subcutaneously, typically starting at 12–15 months of age, with a booster at 4–6 years.
The attenuation process involves serial passage of the pathogen through a foreign host or cell culture, selecting for variants less adapted to causing disease in humans. This method, pioneered by scientists like Albert Sabin for the oral polio vaccine, reduces the pathogen’s virulence while preserving its antigenic properties. The resulting vaccine triggers both humoral and cell-mediated immunity, often conferring long-lasting protection with fewer doses compared to inactivated vaccines. However, attenuated vaccines require careful storage, usually between 2°C and 8°C, to maintain the viability of the live organisms.
While attenuated vaccines are highly effective, they are not without limitations. Individuals with compromised immune systems, such as those undergoing chemotherapy or living with HIV, may be at risk if exposed to even weakened pathogens. Additionally, rare instances of reversion to virulence have been documented, though stringent safety testing minimizes this risk. For example, the varicella vaccine, administered as a 0.5 mL dose subcutaneously at 12–15 months and 4–6 years, is contraindicated in immunocompromised children, highlighting the need for personalized vaccination strategies.
Comparatively, attenuated vaccines offer distinct advantages over other vaccine types. Their ability to mimic natural infection often results in stronger, more durable immunity than subunit or conjugate vaccines. This makes them particularly valuable for preventing highly contagious diseases like yellow fever, where a single 0.5 mL dose provides lifelong protection for most recipients. However, their live nature necessitates careful consideration of contraindications and storage requirements, underscoring the importance of healthcare provider guidance in their administration.
In practice, attenuated vaccines exemplify the elegance of immunological manipulation, transforming potential threats into tools for protection. Their development requires precision, balancing pathogen weakening with immune stimulation, but their impact is profound. From eradicating smallpox to controlling polio, these vaccines have reshaped global health. For parents and caregivers, understanding their mechanism—live, weakened pathogens unable to cause disease but trigger immune response—empowers informed decision-making, ensuring timely and safe immunization for vulnerable populations.
Mercury in Vaccines: Understanding the Amount and Safety Concerns
You may want to see also
Explore related products






![]()
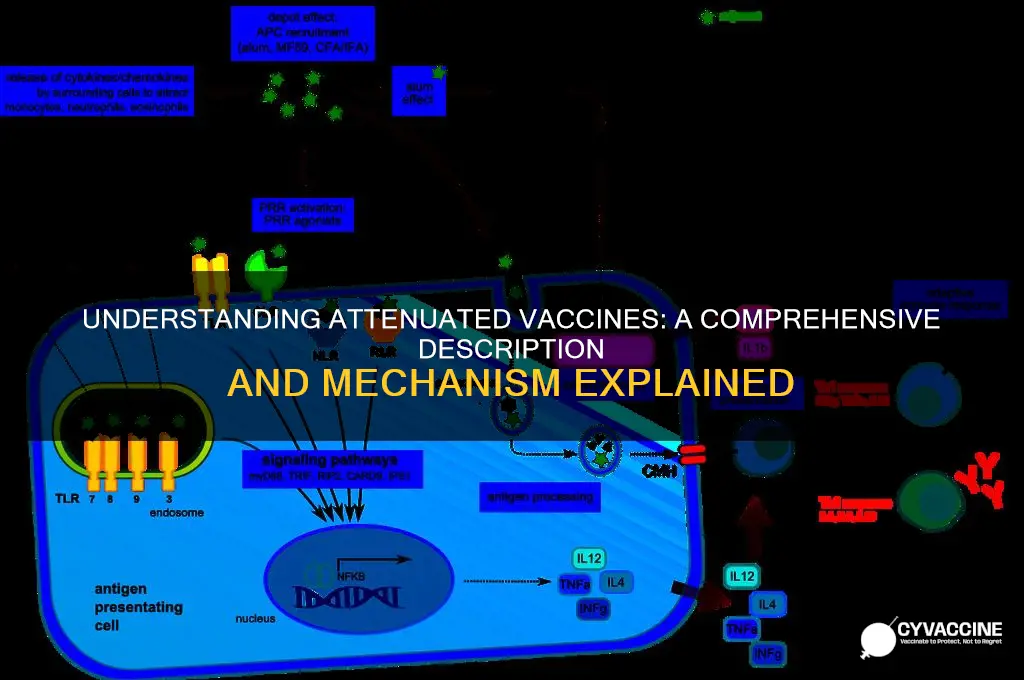
Mechanism: Stimulates immunity by mimicking natural infection without severe symptoms
Attenuated vaccines are a cornerstone of modern immunology, designed to harness the body’s natural defense mechanisms without the risks associated with wild-type pathogens. At their core, these vaccines introduce a weakened (attenuated) version of a virus or bacterium, which retains its ability to provoke an immune response but lacks the virulence to cause severe disease. This delicate balance allows the immune system to recognize, respond to, and remember the pathogen, effectively mimicking a natural infection without the associated morbidity. For instance, the measles, mumps, and rubella (MMR) vaccine uses attenuated strains of each virus, administered in a single dose to children aged 12–15 months, with a booster at 4–6 years. This approach ensures lifelong immunity for over 95% of recipients while avoiding the complications of the actual diseases, such as encephalitis or congenital rubella syndrome.
The mechanism of attenuated vaccines hinges on their ability to replicate within the body, albeit at a reduced rate compared to wild-type pathogens. This limited replication triggers both innate and adaptive immune responses. Innate immunity, the body’s first line of defense, is activated as cells detect pathogen-associated molecular patterns (PAMPs), prompting the release of cytokines and chemokines. Simultaneously, antigen-presenting cells (APCs) engulf the attenuated pathogen, process it, and present its antigens to T cells, initiating adaptive immunity. Unlike inactivated or subunit vaccines, which often require adjuvants to enhance immunity, attenuated vaccines inherently stimulate a robust, multifaceted response due to their live nature. This includes the production of neutralizing antibodies and the generation of memory B and T cells, ensuring rapid protection upon future exposure.
One of the most compelling advantages of attenuated vaccines is their ability to confer long-lasting immunity with minimal doses. For example, the yellow fever vaccine, a live-attenuated product, provides lifelong protection after a single 0.5 mL subcutaneous injection for individuals aged 9 months and older. This efficiency contrasts with subunit vaccines like the hepatitis B vaccine, which typically requires a three-dose series over 6 months. However, this strength also comes with a caveat: attenuated vaccines must be stored and transported under strict cold chain conditions to maintain viability. Exposure to heat or improper handling can render the vaccine ineffective, underscoring the importance of adherence to storage protocols, particularly in resource-limited settings.
Despite their efficacy, attenuated vaccines are not without limitations. Their live nature contraindicates their use in immunocompromised individuals, such as those with HIV/AIDS or undergoing chemotherapy, as the weakened pathogen could potentially cause disease in these populations. Additionally, rare instances of reversion to virulence, where the attenuated strain regains its pathogenicity, have been documented, though such cases are exceedingly uncommon. For example, the oral polio vaccine (OPV), while highly effective, has been associated with vaccine-derived poliovirus (VDPV) in areas with low vaccination coverage. These risks, however, are outweighed by the benefits, particularly in regions where diseases like polio remain endemic. Careful patient selection and monitoring are essential to maximize safety and efficacy.
In practice, the success of attenuated vaccines lies in their ability to replicate the immunological benefits of natural infection while circumventing its dangers. This makes them particularly valuable for preventing diseases with high morbidity and mortality rates, such as varicella (chickenpox) and rotavirus. The varicella vaccine, for instance, is administered in two doses—the first at 12–15 months and the second at 4–6 years—achieving over 90% efficacy in preventing severe disease. For rotavirus, a leading cause of childhood diarrhea, the live-attenuated vaccine is given orally in a 2–3 dose series starting at 6 weeks of age, reducing hospitalizations by 85–90%. These examples highlight the practical utility of attenuated vaccines in public health, offering a safe, effective, and durable solution to some of the world’s most pressing infectious diseases.
Smallpox Vaccine: Active or Passive Immunity?
You may want to see also
Explore related products






![]()
Examples: Measles, mumps, rubella (MMR), varicella (chickenpox) vaccines
Attenuated vaccines, such as the measles, mumps, rubella (MMR) and varicella (chickenpox) vaccines, are cornerstone tools in modern medicine, leveraging weakened pathogens to stimulate immunity without causing disease. These vaccines are administered via injection, typically in combination, to streamline immunization schedules. The MMR vaccine, for instance, is given in two doses: the first at 12–15 months of age and the second at 4–6 years. Similarly, the varicella vaccine follows a two-dose regimen, with the first dose administered between 12–15 months and the second at 4–6 years. This coordinated approach ensures robust protection against four highly contagious diseases with a single set of appointments, minimizing disruption for families and healthcare providers.
Analyzing the MMR vaccine reveals its profound impact on public health. Measles, mumps, and rubella were once common childhood illnesses with severe complications, including encephalitis, deafness, and congenital rubella syndrome. Since the MMR vaccine’s introduction in 1971, global incidence rates have plummeted by over 99%. The attenuated viruses in the vaccine mimic natural infection, prompting the immune system to produce antibodies and memory cells. However, vaccine efficacy hinges on high uptake rates; coverage below 95% can allow outbreaks, as seen in recent measles resurgences linked to vaccine hesitancy. This underscores the importance of community-wide adherence to immunization schedules.
The varicella vaccine, introduced in 1995, transformed chickenpox from a nearly universal childhood experience into a rare occurrence in vaccinated populations. Prior to its development, chickenpox resulted in approximately 10,000 hospitalizations and 100 deaths annually in the U.S. alone. The attenuated varicella-zoster virus in the vaccine reduces the risk of severe disease by 97% and prevents complications like bacterial skin infections and pneumonia. Notably, the vaccine also lowers the risk of shingles later in life by maintaining immune system vigilance against the virus. Parents should be aware that mild side effects, such as a rash or fever, may occur post-vaccination, but these are far less severe than the risks associated with natural infection.
A comparative examination of these vaccines highlights their shared attenuated nature but distinct formulations and outcomes. While the MMR vaccine combines three live attenuated viruses in a single shot, the varicella vaccine targets a single pathogen. Both vaccines boast high efficacy, yet their impact varies due to differences in disease severity and transmission dynamics. For example, rubella’s most critical risk—congenital rubella syndrome—is entirely preventable through vaccination, whereas varicella’s primary benefit lies in reducing morbidity rather than mortality. This nuance emphasizes the need for tailored public health messaging to address specific concerns about each disease.
Practically, parents and caregivers can optimize vaccine effectiveness by adhering to recommended schedules and addressing misconceptions. For children with mild illnesses, vaccination can proceed as planned, but severe illnesses may warrant postponement. Storage and handling are critical; healthcare providers must maintain vaccines at 2–8°C to preserve potency. For those traveling to regions with high disease prevalence, ensuring up-to-date immunization is essential. Finally, open communication with healthcare providers can alleviate concerns and reinforce trust in these life-saving interventions. By understanding the specifics of attenuated vaccines like MMR and varicella, individuals can make informed decisions to protect themselves and their communities.
Understanding Vaccines: How Immunizations Build Lasting Immunity in Your Body
You may want to see also
![]()
Advantages: Long-lasting immunity, fewer doses needed, cost-effective
Attenuated vaccines, crafted from weakened pathogens, offer a robust immune response that mimics natural infection without causing disease. This design inherently confers long-lasting immunity, often rivaling or exceeding that of live exposure. For instance, the measles, mumps, and rubella (MMR) vaccine provides protection for decades, if not a lifetime, after just two doses administered at 12–15 months and 4–6 years of age. This durability reduces the need for frequent boosters, simplifying vaccination schedules and ensuring sustained protection across populations.
One of the most practical advantages of attenuated vaccines is their ability to confer immunity with fewer doses compared to other vaccine types. The yellow fever vaccine, for example, requires a single dose to provide lifelong immunity for most recipients. This efficiency is particularly critical in resource-limited settings, where repeated clinic visits are logistically challenging. Fewer doses also mean lower administrative costs and reduced opportunities for missed vaccinations, enhancing overall coverage rates.
From a cost perspective, attenuated vaccines are a financially prudent choice for both healthcare systems and individuals. Their long-lasting immunity and minimal dosing requirements translate to lower production, distribution, and administration expenses. The oral polio vaccine (OPV), an attenuated vaccine, costs as little as $0.15 per dose, making it accessible even in low-income countries. This cost-effectiveness allows for broader allocation of healthcare resources, enabling investment in other critical health interventions.
To maximize the benefits of attenuated vaccines, healthcare providers should prioritize adherence to recommended schedules. For example, the varicella (chickenpox) vaccine, administered in two doses at 12–15 months and 4–6 years, achieves 98% efficacy when properly timed. Parents and caregivers should also be educated about the importance of completing the full series, as partial vaccination may not confer adequate immunity. Additionally, storing and handling attenuated vaccines correctly—typically at 2°C to 8°C—is essential to maintain their potency and ensure optimal outcomes.
In summary, attenuated vaccines stand out for their ability to provide long-lasting immunity, require fewer doses, and offer cost-effective solutions. These advantages make them a cornerstone of global vaccination efforts, from eradicating polio to preventing measles outbreaks. By understanding and leveraging these benefits, healthcare systems can optimize immunization programs, protect vulnerable populations, and achieve public health goals more efficiently.
Anti-Vaccine Movement vs. Alternative Medicine: Key Differences Explained
You may want to see also
![]()
Limitations: Requires refrigeration, potential risks for immunocompromised individuals
Attenuated vaccines, while highly effective in preventing infectious diseases, come with specific logistical and safety challenges. One significant limitation is their requirement for refrigeration, often referred to as the "cold chain." Unlike some inactivated or subunit vaccines, attenuated vaccines contain live, weakened pathogens that must be kept at precise temperatures (typically 2°C to 8°C) to remain viable. This necessity complicates distribution, particularly in remote or resource-limited areas where reliable electricity or refrigeration infrastructure may be lacking. For instance, the measles, mumps, and rubella (MMR) vaccine, a live attenuated vaccine, loses potency if exposed to temperatures outside this range, rendering it ineffective. Ensuring a consistent cold chain is not just a matter of convenience but a critical factor in vaccine efficacy and public health outcomes.
Another critical limitation of attenuated vaccines is their potential risk to immunocompromised individuals. Because these vaccines contain live pathogens, albeit weakened, they can pose a threat to those with weakened immune systems. For example, the varicella vaccine (for chickenpox) is contraindicated in individuals with severe immune deficiencies, as the attenuated virus could replicate unchecked, leading to severe illness. Similarly, the oral polio vaccine (OPV), though rarely used in developed countries, has been associated with vaccine-derived poliovirus cases in immunocompromised patients. Healthcare providers must carefully assess a patient’s immune status before administering such vaccines, often relying on blood tests or medical history to determine eligibility. This precaution underscores the delicate balance between protecting the individual and preventing disease transmission.
To mitigate these limitations, practical strategies can be employed. For the cold chain challenge, innovations like solar-powered refrigerators and temperature-monitoring devices are being deployed in low-resource settings. Additionally, vaccine manufacturers are exploring formulations that are more heat-stable, reducing reliance on refrigeration. For immunocompromised individuals, alternative vaccination strategies, such as using inactivated vaccines or delaying immunization until immune function improves, can be considered. For example, a child undergoing chemotherapy might receive the inactivated polio vaccine (IPV) instead of OPV. Clear communication between healthcare providers and patients is essential to ensure informed decision-making and minimize risks.
Despite these challenges, attenuated vaccines remain a cornerstone of preventive medicine, offering robust immunity through mimicry of natural infection. However, their limitations demand careful planning and resource allocation. For instance, global vaccination campaigns must account for cold chain maintenance, while individual healthcare providers must tailor vaccine choices to patient-specific risks. By addressing these constraints proactively, the benefits of attenuated vaccines can be maximized while minimizing potential harm. This dual focus on efficacy and safety ensures that these vaccines continue to play a vital role in global health initiatives.
Schedule Your Vaccine Appointment in Oregon: A Step-by-Step Guide
You may want to see also
Frequently asked questions
An attenuated vaccine is a type of vaccine that contains a weakened (attenuated) form of a live virus or bacteria, which is unable to cause severe disease in healthy individuals but can still elicit a strong immune response.
An attenuated vaccine differs from inactivated or subunit vaccines because it uses a live, albeit weakened, pathogen. This allows the immune system to respond more robustly, often providing longer-lasting immunity with fewer doses compared to other vaccine types.
Examples of attenuated vaccines include the measles, mumps, and rubella (MMR) vaccine, the varicella (chickenpox) vaccine, the yellow fever vaccine, and the oral polio vaccine (OPV). These vaccines have been widely used and are highly effective in preventing diseases.