When considering the best coronavirus vaccine to have, it’s essential to recognize that all authorized vaccines, such as Pfizer-BioNTech, Moderna, AstraZeneca, and Johnson & Johnson, have proven effective in preventing severe illness, hospitalization, and death from COVID-19. The best vaccine often depends on individual factors like age, health conditions, and availability in your region. Health authorities, including the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC), emphasize that the most effective vaccine is the one you can get promptly, as timely vaccination is crucial for protection. Additionally, staying updated with booster doses and following local health guidelines ensures maximum immunity against evolving variants. Ultimately, consulting with a healthcare provider can help determine the most suitable option for your specific needs.
Explore related products



$11.93 $21.99


What You'll Learn
- Efficacy Rates: Comparing vaccine effectiveness against COVID-19 symptoms, hospitalization, and death across different vaccines
- Side Effects: Analyzing common and rare side effects of each vaccine for informed decision-making
- Availability: Assessing global and local access to vaccines based on distribution and supply chains
- Variants Coverage: Evaluating vaccine performance against emerging COVID-19 variants like Delta and Omicron
- Booster Recommendations: Understanding the need and timing for booster shots with different vaccines
![]()
Efficacy Rates: Comparing vaccine effectiveness against COVID-19 symptoms, hospitalization, and death across different vaccines
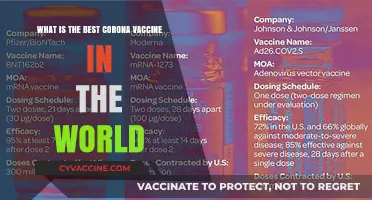
The efficacy of COVID-19 vaccines varies across different outcomes, such as preventing symptoms, hospitalization, and death. For instance, the Pfizer-BioNTech mRNA vaccine demonstrated 95% efficacy in preventing symptomatic COVID-19 in clinical trials, while the Oxford-AstraZeneca viral vector vaccine showed 70% efficacy in similar trials. However, these numbers don’t tell the whole story. When it comes to severe outcomes, such as hospitalization and death, the gap between vaccines narrows significantly. Both Pfizer and AstraZeneca vaccines have shown over 90% effectiveness in preventing COVID-19-related hospitalizations in real-world studies, highlighting that even vaccines with lower symptomatic efficacy can still provide robust protection against severe disease.
Consider the role of dosage and administration intervals, which can influence efficacy rates. The Moderna mRNA-1273 vaccine, administered in two doses 28 days apart, boasts 94.1% efficacy against symptomatic COVID-19. In contrast, the Johnson & Johnson single-dose viral vector vaccine offers 66% efficacy globally but rises to 72% in the U.S., where COVID-19 variants and healthcare access differ. Interestingly, a study in *The Lancet* found that delaying the second dose of the AstraZeneca vaccine to 12 weeks increased efficacy to 81%, compared to 55% with a 4-week interval. This underscores the importance of following recommended dosing schedules to maximize protection.
For specific populations, such as older adults and immunocompromised individuals, efficacy rates may vary. The Pfizer vaccine maintains 94% effectiveness against hospitalization in individuals over 65, while AstraZeneca’s efficacy in this age group is around 80%. However, real-world data from Israel showed that even with high vaccination rates, breakthrough infections occurred more frequently in older adults, emphasizing the need for booster doses. The CDC recommends boosters for all adults, particularly those over 50, to restore waning immunity and maintain high protection levels against severe outcomes.
Practical considerations also play a role in vaccine choice. mRNA vaccines (Pfizer and Moderna) require ultra-cold storage, which can limit accessibility in low-resource settings. In contrast, AstraZeneca and Johnson & Johnson vaccines are stable at standard refrigeration temperatures, making them more suitable for global distribution. For individuals in regions with limited healthcare infrastructure, a single-dose vaccine like Johnson & Johnson may be the most practical option, despite its slightly lower symptomatic efficacy, as it ensures full protection after one dose.
In conclusion, while symptomatic efficacy rates are a common metric for comparing vaccines, their effectiveness against hospitalization and death is the critical factor in preventing severe public health outcomes. Factors like dosage intervals, population demographics, and logistical considerations further shape the "best" vaccine choice. Rather than focusing solely on trial data, individuals should consider real-world performance, local variant prevalence, and personal health status when deciding. Ultimately, the best vaccine is the one that provides robust protection against severe disease and is readily accessible.
Ask Cities: Do They Vaccinate Immigrants?
You may want to see also
Explore related products





![]()
Side Effects: Analyzing common and rare side effects of each vaccine for informed decision-making
Understanding the side effects of COVID-19 vaccines is crucial for making an informed decision. While all approved vaccines have proven effective in preventing severe illness and death, their side effect profiles differ, influencing individual preferences. Common side effects across Pfizer-BioNTech, Moderna, Johnson & Johnson, and AstraZeneca vaccines include pain at the injection site, fatigue, headache, and muscle pain, typically resolving within a few days. These reactions indicate the immune system is responding to the vaccine, not an infection. For instance, mRNA vaccines (Pfizer and Moderna) often cause more pronounced side effects after the second dose, while the viral vector vaccines (J&J and AstraZeneca) may cause flu-like symptoms or rare clotting issues.
Rare but serious side effects require careful consideration. The Johnson & Johnson vaccine has been linked to a rare blood clotting disorder called thrombosis with thrombocytopenia syndrome (TTS), occurring in approximately 7 per 1 million vaccinated women aged 18–49. AstraZeneca reports a similar risk, though slightly higher, particularly in younger adults. Conversely, mRNA vaccines have a rare association with myocarditis or pericarditis, primarily in adolescent males and young adults after the second dose. The CDC notes 1–2 cases per 100,000 vaccinated individuals in this demographic. These risks, though low, highlight the importance of age and health status in vaccine selection.
For informed decision-making, consider individual health factors. Pregnant individuals, for example, are advised to receive Pfizer or Moderna due to robust safety data and reduced risk of rare complications. Those with a history of severe allergies to vaccine components should consult a healthcare provider before proceeding. Age is another critical factor: individuals under 30 may opt for mRNA vaccines despite the slight myocarditis risk, while older adults might prioritize accessibility, such as the single-dose J&J vaccine. Dosage also matters—Pfizer’s 30-microgram dose for adults contrasts with Moderna’s 100-microgram dose, potentially influencing side effect severity.
Practical tips can mitigate side effects. Hydration, over-the-counter pain relievers (e.g., acetaminophen or ibuprofen), and rest are effective for managing common symptoms. Avoid strenuous activity post-vaccination, especially after the second dose of mRNA vaccines. For rare side effects, awareness is key: seek medical attention for persistent headaches, blurred vision, or chest pain after J&J or AstraZeneca vaccination, or chest pain and shortness of breath after mRNA vaccines. Monitoring for 2–3 weeks post-vaccination ensures timely intervention if complications arise.
Ultimately, the "best" vaccine depends on balancing efficacy, side effect profiles, and individual circumstances. While rare side effects exist, the risk of severe COVID-19 far outweighs vaccine risks. Public health bodies emphasize that any approved vaccine is preferable to no vaccine. By analyzing side effects and personal health factors, individuals can make confident choices, contributing to both personal and community protection.
Vaccine Conspiracy Debunked: Separating Fact from 'Mark of the Beast' Fiction
You may want to see also
Explore related products






![]()
Availability: Assessing global and local access to vaccines based on distribution and supply chains
Global vaccine distribution has been a stark reminder of inequity, with high-income countries securing the lion's share of doses early in the pandemic. By mid-2021, COVAX, the global initiative aimed at equitable access, had delivered just 10% of its initial target, while wealthy nations stockpiled vaccines. This disparity wasn’t merely a moral failing; it prolonged the pandemic by allowing variants like Delta and Omicron to emerge in under-vaccinated regions. Supply chains, reliant on ultra-cold storage for mRNA vaccines like Pfizer-BioNTech (requiring -70°C) and Moderna (-20°C), further disadvantaged low-income countries lacking such infrastructure. In contrast, AstraZeneca and Johnson & Johnson’s vaccines, stable at standard refrigeration temperatures (2-8°C), became lifelines for resource-constrained regions, though their rollout was hampered by production delays and safety concerns.
Locally, vaccine availability often hinged on logistical finesse and political will. In the U.S., Operation Warp Speed prioritized rapid production but left states scrambling to distribute doses, with some rural areas receiving fewer vaccines per capita due to storage limitations. In India, the Serum Institute’s production of the Oxford-AstraZeneca vaccine (branded Covishield) enabled mass vaccination, but export bans during domestic surges highlighted the fragility of global supply chains. Meanwhile, South Africa’s Aspen Pharmacare became a key producer of Johnson & Johnson’s single-dose vaccine, yet local uptake was hindered by misinformation and hesitancy. These examples underscore how distribution networks, not just manufacturing capacity, dictate access.
For individuals navigating vaccine availability, understanding local supply chains is crucial. In regions with limited mRNA vaccine access, opting for AstraZeneca or Sinopharm—which require simpler storage—may be more practical. Age and health conditions also factor in; for instance, many countries prioritized Pfizer for adolescents (approved for ages 5+ in some regions) due to its robust safety data in younger populations, while Johnson & Johnson’s single-dose regimen was favored for hard-to-reach communities. Practical tips include monitoring local health department updates, leveraging community health workers for information, and being flexible with vaccine type to ensure timely protection.
The takeaway is clear: the “best” vaccine is often the one most accessible to you, shaped by global supply chains and local infrastructure. While mRNA vaccines boast higher efficacy rates (95% for Pfizer, 94% for Moderna), their distribution remains skewed toward wealthy nations. Viral vector vaccines like AstraZeneca (70-80% efficacy) and protein-based vaccines like Novavax (90% efficacy) offer viable alternatives, particularly in regions with limited cold-chain capabilities. Ultimately, global equity in vaccine distribution isn’t just a humanitarian imperative—it’s a public health necessity to end the pandemic for all.
Puppy Fatigue Post-Vaccination: Understanding Normal Tiredness After Shots
You may want to see also
Explore related products





![EvolveFISH Vaccines Cause Adults Bumper Sticker - [11'' x 3'']](https://m.media-amazon.com/images/I/61kmYe3Td1L._AC_UL320_.jpg)
![]()
Variants Coverage: Evaluating vaccine performance against emerging COVID-19 variants like Delta and Omicron
The emergence of COVID-19 variants like Delta and Omicron has underscored the critical need to evaluate vaccine performance beyond initial efficacy rates. While vaccines were developed to target the original SARS-CoV-2 strain, their effectiveness against mutations in the virus’s spike protein—key to infection—varies significantly. For instance, the Omicron variant’s extensive mutations have led to reduced neutralizing antibody responses in fully vaccinated individuals, though protection against severe disease remains robust. This highlights the importance of assessing vaccines not just by their initial performance but by their adaptability to evolving threats.
Analyzing variant coverage requires examining both laboratory data and real-world outcomes. Studies measuring neutralizing antibody titers post-vaccination provide early indicators of potential efficacy against new strains. For example, mRNA vaccines (Pfizer-BioNTech and Moderna) have shown higher titers compared to viral vector vaccines (AstraZeneca and Johnson & Johnson) in some studies, though all vaccines maintain substantial protection against hospitalization and death. However, lab data alone is insufficient; population-level surveillance in countries with high vaccination rates, such as Israel and the UK, has been pivotal in understanding how vaccines perform against Delta and Omicron in diverse age groups and immune statuses.
Practical considerations for individuals include booster doses and vaccine mixing. Boosters significantly enhance neutralizing antibody levels, particularly against Omicron. For mRNA vaccines, a third dose administered 6 months after the initial series restores protection to over 75% against symptomatic infection, according to CDC data. Heterologous boosting—using a different vaccine type for the booster—has also shown promise, with studies indicating improved immune responses compared to homologous boosting. For example, individuals who received AstraZeneca initially may benefit from an mRNA booster to broaden their immune response.
Age and comorbidities play a critical role in variant coverage. While vaccines remain highly effective in preventing severe outcomes across all age groups, older adults and immunocompromised individuals may experience waning immunity faster. For those over 65 or with conditions like diabetes or heart disease, timely boosters are essential. Additionally, pediatric populations, now eligible for vaccination in many countries, show robust responses to age-appropriate doses (e.g., 10 µg for Pfizer in children 5-11 vs. 30 µg for adults), though data on variant-specific efficacy is still emerging.
In conclusion, evaluating vaccine performance against variants like Delta and Omicron requires a multifaceted approach, combining lab research, real-world data, and tailored strategies for different populations. While no single vaccine guarantees complete protection against all variants, the ability to prevent severe disease and death remains a consistent strength across vaccine types. Staying updated with recommended doses, considering boosters, and monitoring public health guidelines are practical steps individuals can take to maximize protection in the face of evolving viral threats.
Vaccinations: Training Our Adaptive Immune Response
You may want to see also
Explore related products






![]()
Booster Recommendations: Understanding the need and timing for booster shots with different vaccines
The effectiveness of COVID-19 vaccines wanes over time, making booster shots crucial for maintaining immunity against severe illness, hospitalization, and death. While all authorized vaccines provide robust initial protection, their longevity varies, necessitating tailored booster strategies. For instance, mRNA vaccines (Pfizer-BioNTech and Moderna) typically show a more pronounced decline in efficacy after 6 months, whereas viral vector vaccines (AstraZeneca and Johnson & Johnson) may require boosters sooner due to lower initial antibody levels. Understanding these differences is essential for informed decision-making.
Analyzing Timing and Eligibility: Booster timing depends on the primary vaccine series and individual risk factors. For Pfizer and Moderna recipients, the CDC recommends a booster 5 months after the second dose, with a second booster for those over 50 or immunocompromised. AstraZeneca recipients, particularly in regions where it was widely used, often require a booster 3–6 months after their second dose, ideally with an mRNA vaccine for enhanced immunity. Johnson & Johnson recipients should receive a booster 2 months after their initial dose, as a single shot provides less durable protection. Age, health status, and exposure risk further refine these timelines, emphasizing the need for personalized recommendations.
Comparing Booster Efficacy: Studies show that mRNA boosters significantly increase antibody levels, reducing the risk of symptomatic infection and severe outcomes. For example, a Pfizer booster restores efficacy to over 90% against severe disease. Mixing vaccines, such as using an mRNA booster after AstraZeneca, often yields superior results compared to homologous boosting. This heterologous approach leverages the strengths of different vaccine platforms, providing broader immune responses. However, vaccine availability and regulatory approvals may limit these options in certain regions, underscoring the importance of local guidelines.
Practical Tips for Booster Scheduling: To ensure timely boosting, track your vaccination dates and stay informed about eligibility updates. Many countries offer online tools or apps to simplify this process. If you’re traveling, verify booster requirements at your destination, as some regions mandate specific vaccines or intervals. For immunocompromised individuals, consult a healthcare provider to determine the optimal timing and dosage, as additional doses may be necessary. Finally, plan for potential side effects, such as fatigue or soreness, by scheduling boosters during periods of lower activity.
Takeaway: Booster shots are not one-size-fits-all. Their necessity and timing hinge on the primary vaccine, individual health, and evolving viral threats. By understanding these nuances, individuals can maximize their protection and contribute to collective immunity. Stay proactive, follow local health advisories, and prioritize boosting as a critical step in the ongoing fight against COVID-19.
Strategies to Support Your Team in Meeting Vaccination Quotas Effectively
You may want to see also
Frequently asked questions
There is no single "best" coronavirus vaccine; all vaccines authorized by health agencies (e.g., Pfizer-BioNTech, Moderna, AstraZeneca, Johnson & Johnson, Sinovac, Sinopharm) are highly effective at preventing severe illness, hospitalization, and death from COVID-19. The best vaccine is the one available to you.
mRNA vaccines (Pfizer and Moderna) have shown high efficacy rates and are widely used, but other vaccines like AstraZeneca (viral vector) and Sinovac (inactivated virus) are also effective, especially in preventing severe outcomes. The choice depends on availability and individual health considerations.
While efficacy rates vary slightly between vaccines, all authorized vaccines provide strong protection against severe COVID-19. Focus on getting vaccinated as soon as possible rather than waiting for a specific vaccine.
Studies show that mixing vaccines (heterologous vaccination) can be safe and effective, often providing robust immune responses. Many countries recommend this approach, especially if the same vaccine is not available for a second dose.
For children, Pfizer-BioNTech is widely approved and recommended for ages 5 and up. For older adults, all vaccines are effective, but some countries prioritize mRNA vaccines due to their high efficacy and booster recommendations. Consult local health guidelines for specific advice.