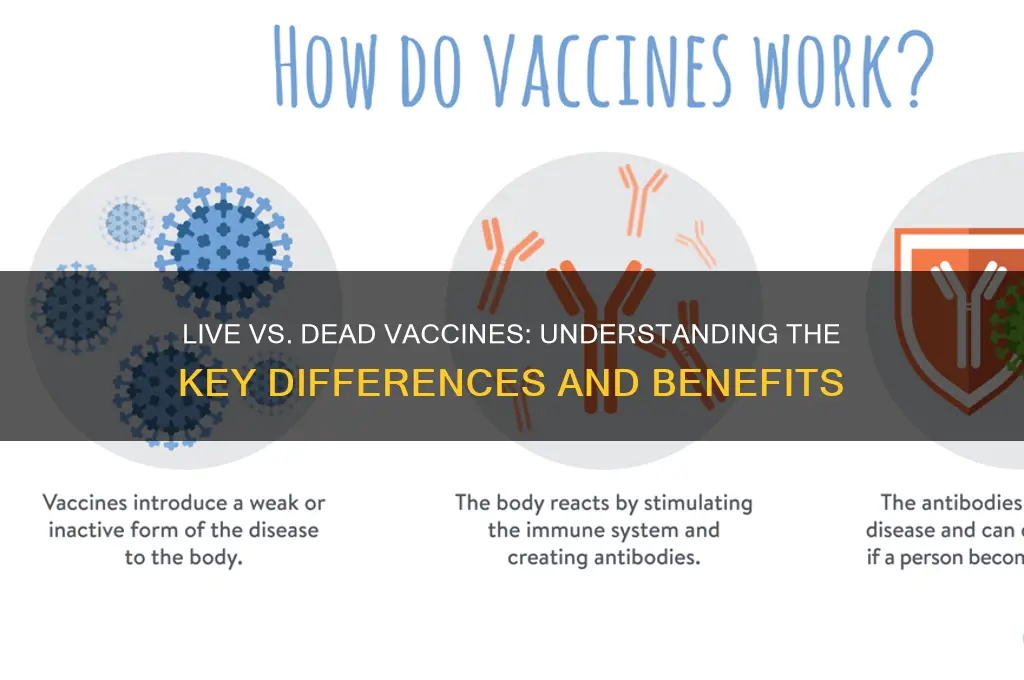
Vaccines are essential tools in preventing infectious diseases, and they can be broadly categorized into two main types: live vaccines and dead (or inactivated) vaccines. A live vaccine contains a weakened (attenuated) form of the virus or bacteria, which is still capable of replicating but does not cause severe disease in healthy individuals. This type of vaccine mimics a natural infection, triggering a robust immune response and often providing long-lasting immunity with fewer doses. Examples include the measles, mumps, and rubella (MMR) vaccine and the oral polio vaccine. In contrast, a dead vaccine uses a killed or inactivated version of the pathogen, rendering it unable to replicate. While this type of vaccine is safer for individuals with weakened immune systems, it typically requires multiple doses and booster shots to achieve and maintain immunity. Examples include the injectable polio vaccine and the hepatitis A vaccine. Understanding the differences between these vaccine types is crucial for appreciating their effectiveness, safety profiles, and appropriate use in public health strategies.
| Characteristics | Values |
|---|---|
| Type of Vaccine | Live (Attenuated) vs. Dead (Inactivated) |
| Virus/Bacteria State | Live: Weakened but alive; Dead: Killed or inactivated |
| Immune Response | Live: Stronger, more durable; Dead: Weaker, may require boosters |
| Doses Required | Live: Typically fewer doses; Dead: Multiple doses often needed |
| Storage Requirements | Live: Strict cold chain (refrigeration); Dead: More stable, easier storage |
| Safety | Live: Risk for immunocompromised; Dead: Generally safer for all |
| Examples | Live: MMR (Measles, Mumps, Rubella), Varicella; Dead: Polio (IPV), Flu |
| Efficacy | Live: High efficacy; Dead: Moderate to high, depends on pathogen |
| Cost | Live: Generally higher production cost; Dead: Lower cost |
| Administration Route | Both: Typically injected (intramuscular or subcutaneous) |
| Duration of Protection | Live: Long-lasting; Dead: Shorter, may wane over time |
| Risk of Reversion | Live: Rare risk of reverting to virulent form; Dead: No risk |
| Use in Immunocompromised | Live: Not recommended; Dead: Safe for immunocompromised individuals |
| Development Time | Live: Longer development process; Dead: Faster to produce |
| Adjuvants Needed | Dead: Often requires adjuvants to enhance immune response; Live: Rarely |
Explore related products


$19.95 $19.95




What You'll Learn
- Live Vaccines: Weakened pathogens, replicate in body, trigger strong immune response, long-lasting immunity
- Dead Vaccines: Inactivated pathogens, cannot replicate, safer, often require adjuvants or boosters
- Immune Response: Live vaccines mimic infection, dead vaccines rely on antigen presentation
- Storage & Stability: Live vaccines need refrigeration, dead vaccines more stable at room temperature
- Examples: Live (MMR, varicella), Dead (flu shot, polio IPV, hepatitis B)
![]()
Live Vaccines: Weakened pathogens, replicate in body, trigger strong immune response, long-lasting immunity
Live vaccines harness the power of weakened pathogens to stimulate a robust and enduring immune response. Unlike their inactivated counterparts, these vaccines contain attenuated microorganisms that retain the ability to replicate within the body, albeit at a reduced rate. This replication mimics a natural infection, prompting the immune system to mount a vigorous defense. The result? A memory response so potent that it often confers lifelong immunity with just one or two doses. For instance, the measles, mumps, and rubella (MMR) vaccine, a live attenuated formulation, provides over 95% protection against these diseases after two doses, typically administered at 12–15 months and 4–6 years of age.
The mechanism behind live vaccines’ effectiveness lies in their ability to engage multiple arms of the immune system. As the weakened pathogen replicates, it triggers both humoral (antibody-mediated) and cell-mediated immunity. This dual activation ensures a comprehensive defense, making live vaccines particularly effective against viruses and intracellular bacteria. However, this strength comes with a caveat: the replication process, though controlled, can pose risks for individuals with compromised immune systems. Immunocompromised individuals, such as those undergoing chemotherapy or living with HIV, are generally advised to avoid live vaccines due to the potential for the attenuated pathogen to cause disease.
One of the most compelling advantages of live vaccines is their ability to provide long-lasting immunity with minimal dosing. The varicella vaccine, for example, protects against chickenpox with a 98% efficacy rate after two doses, administered at 12–15 months and 4–6 years. This contrasts sharply with many inactivated vaccines, which often require booster shots to maintain immunity. The simplicity of the dosing regimen not only reduces healthcare costs but also improves compliance, particularly in pediatric populations where multiple injections can be challenging.
Despite their efficacy, live vaccines are not without limitations. Their sensitivity to temperature and storage conditions can complicate distribution, particularly in resource-limited settings. For instance, the oral polio vaccine (OPV), a live attenuated vaccine, must be stored between 2°C and 8°C to remain viable. Additionally, the risk of reversion—where the attenuated pathogen regains virulence—is a theoretical concern, though rare. Practical tips for healthcare providers include ensuring proper storage, verifying patient immune status before administration, and educating caregivers about potential mild side effects, such as fever or rash, which are typically transient and benign.
In summary, live vaccines represent a cornerstone of modern immunology, offering a powerful and efficient means of disease prevention. Their ability to replicate within the body, trigger a strong immune response, and confer long-lasting immunity makes them indispensable tools in the fight against infectious diseases. While their use requires careful consideration of patient immunity and storage logistics, the benefits far outweigh the challenges. As we continue to refine vaccine technologies, live attenuated vaccines will undoubtedly remain a vital component of global health strategies.
Half Vaccinated: Understanding Partial Immunity and Its Implications
You may want to see also
Explore related products





![]()
Dead Vaccines: Inactivated pathogens, cannot replicate, safer, often require adjuvants or boosters
Dead vaccines, also known as inactivated vaccines, are a cornerstone of modern immunization strategies. Unlike their live counterparts, these vaccines contain pathogens that have been killed or rendered incapable of replication. This fundamental difference in design imparts a unique safety profile, making them a preferred choice for certain populations, such as immunocompromised individuals or pregnant women, where the risk of a live vaccine's potential, albeit rare, complications is a concern.
Inactivated vaccines are created through various methods, including heat, chemicals, or radiation, effectively destroying the pathogen's ability to cause disease while preserving its antigenic properties. This process ensures that the immune system can still recognize and mount a response against the pathogen, generating protective antibodies and memory cells. For instance, the influenza vaccine, a widely administered dead vaccine, is typically given as a single dose annually, with specific formulations tailored for different age groups, such as the high-dose version for adults over 65.
The safety advantages of dead vaccines are particularly evident in their reduced reactogenicity compared to live vaccines. Since the pathogens cannot replicate, the risk of adverse reactions, such as fever or localized pain at the injection site, is generally lower. However, this safety comes at a cost: inactivated vaccines often require adjuvants, substances added to enhance the immune response, as the killed pathogens may not stimulate the immune system as effectively as live ones. Common adjuvants include aluminum salts, which have been used for decades and are considered safe for most individuals. Additionally, dead vaccines frequently necessitate booster doses to maintain immunity, as the initial response may wane over time.
Consider the hepatitis A vaccine, a dead vaccine administered in two doses, typically 6 to 18 months apart, for long-term protection. This dosing schedule highlights the importance of adherence to ensure optimal immunity. For travelers to endemic regions, it’s crucial to plan ahead, as the second dose is essential for sustained protection. Similarly, the rabies vaccine, another inactivated vaccine, is given in a series of shots over several weeks, often accompanied by rabies immune globulin for immediate protection in case of exposure. These examples underscore the need for careful planning and compliance with vaccination schedules to maximize the benefits of dead vaccines.
While dead vaccines offer significant safety advantages, their limitations must be acknowledged. The reliance on adjuvants and boosters can complicate vaccination campaigns, particularly in resource-limited settings where access to healthcare may be intermittent. Moreover, the manufacturing process for inactivated vaccines can be more complex and costly compared to live vaccines, potentially impacting their availability. Despite these challenges, dead vaccines remain a vital tool in public health, providing a safer alternative for vulnerable populations and contributing to the global effort to control and eradicate infectious diseases. Understanding their unique characteristics and requirements is essential for healthcare providers and individuals alike to make informed decisions about immunization.
Can Microchips Be Implanted via Vaccines? Debunking the Myth
You may want to see also
Explore related products






![]()
Immune Response: Live vaccines mimic infection, dead vaccines rely on antigen presentation
Live vaccines, such as the measles, mumps, and rubella (MMR) vaccine, introduce a weakened form of the virus into the body, triggering a robust immune response that closely mimics a natural infection. This approach stimulates both arms of the immune system: the innate response, which acts as the body’s immediate defense, and the adaptive response, which produces memory cells for long-term immunity. For instance, a single 0.5 mL dose of the MMR vaccine, typically administered at 12–15 months of age, confers lifelong protection in 97% of recipients. The key advantage here is the vaccine’s ability to replicate, albeit at a reduced rate, allowing the immune system to recognize and respond to the pathogen as it would in a real infection, without causing severe disease.
In contrast, dead vaccines, like the inactivated polio vaccine (IPV), rely on antigen presentation to elicit immunity. These vaccines contain viruses or bacteria that have been killed or inactivated, rendering them unable to replicate. The immune system identifies the presented antigens—specific proteins or structures from the pathogen—and mounts a targeted response. A standard 0.5 mL dose of IPV, given in multiple rounds starting at 2 months of age, provides robust protection by priming B cells to produce antibodies. However, because the pathogen cannot replicate, the immune response is generally less vigorous than with live vaccines, often requiring booster doses to maintain immunity.
The distinction in immune response between live and dead vaccines has practical implications for vaccine design and administration. Live vaccines, due to their ability to mimic infection, typically require fewer doses—often just one or two—to achieve lasting immunity. However, they are contraindicated in immunocompromised individuals, as the weakened pathogen could potentially cause disease in those with weakened immune systems. Dead vaccines, while safer for vulnerable populations, often necessitate multiple doses and adjuvants to enhance the immune response. For example, the hepatitis B vaccine, a dead vaccine, requires three doses over 6 months to ensure adequate protection.
Understanding these mechanisms allows healthcare providers to tailor vaccination strategies to specific populations. For healthy children and adults, live vaccines offer a highly effective, dose-sparing option. In contrast, dead vaccines are the preferred choice for pregnant women, the elderly, or those with compromised immunity, where the risk of even a mild vaccine-induced infection outweighs the benefits. By leveraging the unique immune responses triggered by live and dead vaccines, public health initiatives can maximize protection while minimizing risks, ensuring broader coverage and sustained immunity across diverse demographics.
Legal Ways to Decline Vaccines in California: Your Rights Explained
You may want to see also
Explore related products






![]()
Storage & Stability: Live vaccines need refrigeration, dead vaccines more stable at room temperature
Live vaccines, such as the measles, mumps, and rubella (MMR) vaccine, contain weakened but still active viruses or bacteria. This delicate balance between efficacy and safety demands precise storage conditions. Unlike their inactivated counterparts, live vaccines must be refrigerated at temperatures between 2°C and 8°C (36°F and 46°F) to maintain their potency. Even brief exposure to higher temperatures can render them ineffective, necessitating a cold chain—a temperature-controlled supply chain—from manufacturing to administration. This logistical challenge is particularly acute in remote or resource-limited areas, where reliable refrigeration may be scarce.
In contrast, dead or inactivated vaccines, like the polio (IPV) or hepatitis A vaccines, are far more forgiving. These vaccines contain viruses or bacteria that have been killed or rendered non-infectious, making them inherently more stable. Most can withstand room temperature for extended periods, often up to several weeks, without significant loss of efficacy. This stability simplifies distribution and storage, reducing the need for expensive refrigeration infrastructure. For instance, the IPV vaccine can be stored at room temperature for up to 25 days, according to the World Health Organization, making it a practical choice for mass immunization campaigns.
The stability of dead vaccines also translates to greater flexibility in administration. Live vaccines often require strict adherence to storage guidelines, with healthcare providers needing to ensure the vaccine remains refrigerated until just before use. Dead vaccines, however, can be transported and stored with less anxiety, allowing for more spontaneous or mobile vaccination efforts. This is particularly beneficial in emergency situations, such as disease outbreaks, where rapid deployment is critical.
Despite their stability, dead vaccines are not without storage considerations. While they tolerate room temperature better than live vaccines, prolonged exposure to heat or direct sunlight can still degrade their effectiveness. Manufacturers typically provide specific guidelines, such as storing the vaccine in its original packaging and protecting it from light. For example, the hepatitis A vaccine should be stored between 2°C and 8°C but can be kept at room temperature for up to 24 hours if necessary. Adhering to these recommendations ensures the vaccine remains safe and effective for the intended population, often children as young as 12 months or adults at risk of exposure.
In summary, the storage and stability of vaccines are pivotal factors in their global accessibility and effectiveness. Live vaccines, with their refrigeration requirements, pose logistical hurdles but offer robust immunity when handled correctly. Dead vaccines, with their greater stability, provide a practical alternative, particularly in settings where cold chains are challenging to maintain. Understanding these differences empowers healthcare providers and policymakers to make informed decisions, ensuring vaccines reach those who need them most, regardless of geographic or infrastructural constraints.
Understanding Vaccine Sensitivity: Causes, Symptoms, and What It Means for You
You may want to see also
Explore related products






![]()
Examples: Live (MMR, varicella), Dead (flu shot, polio IPV, hepatitis B)
Live vaccines, such as the MMR (measles, mumps, rubella) and varicella (chickenpox) vaccines, contain weakened forms of the virus that trigger a robust immune response without causing the disease. For instance, the MMR vaccine is typically administered in two doses: the first at 12–15 months and the second at 4–6 years. This schedule ensures lifelong immunity for most recipients, with effectiveness rates exceeding 95%. Similarly, the varicella vaccine, given in two doses starting at 12–15 months, reduces the risk of severe chickenpox complications like pneumonia or encephalitis. These vaccines are highly effective but should not be given to immunocompromised individuals, as the live virus could pose a risk.
In contrast, dead vaccines, such as the flu shot, polio IPV (inactivated poliovirus), and hepatitis B vaccine, use killed or inactivated pathogens to stimulate immunity. The flu shot, for example, is reformulated annually to match circulating strains and is recommended for everyone aged 6 months and older, with a single dose each year. Polio IPV, administered in four doses starting at 2 months, has been instrumental in nearly eradicating polio globally, offering 99% protection after the full series. The hepatitis B vaccine, given in three doses over 6 months, is particularly crucial for newborns, as it prevents chronic liver disease and cancer later in life. These dead vaccines are safer for immunocompromised individuals but may require booster shots to maintain immunity.
Comparing live and dead vaccines highlights their distinct advantages and limitations. Live vaccines, like MMR and varicella, often provide stronger, longer-lasting immunity with fewer doses but carry a small risk for those with weakened immune systems. Dead vaccines, such as the flu shot and polio IPV, are safer for broader populations but may require more frequent administration. For example, the flu shot’s annual reformulation contrasts with the MMR’s lifelong protection after two doses. Understanding these differences helps healthcare providers tailor vaccination plans to individual needs, balancing efficacy and safety.
Practical considerations for these vaccines include storage and administration. Live vaccines, such as MMR and varicella, require refrigeration to maintain potency, while dead vaccines like the flu shot and hepatitis B are more stable. Parents should ensure their children receive vaccines on schedule, as delays can leave them vulnerable to preventable diseases. For adults, staying updated with flu shots and hepatitis B boosters is essential, especially for those in high-risk occupations or with chronic conditions. Always consult a healthcare provider for personalized advice, as factors like allergies, pregnancy, or underlying health issues may influence vaccine suitability.
In summary, live vaccines like MMR and varicella offer powerful, long-term protection but require careful consideration for immunocompromised individuals. Dead vaccines, including the flu shot and polio IPV, provide safer alternatives with broader applicability, though they may demand more frequent doses. By understanding these examples, individuals can make informed decisions about their health and contribute to community immunity. Whether live or dead, these vaccines are cornerstone tools in preventing disease and saving lives.
Ensuring Vaccine Safety: How Often to Check Expiration Dates
You may want to see also
Frequently asked questions
A live vaccine uses a weakened (attenuated) form of the virus or bacteria that causes a disease. It replicates in the body, triggering a strong immune response without causing the actual disease.
A dead vaccine, also known as an inactivated vaccine, uses a killed version of the virus or bacteria. It cannot replicate in the body but still prompts the immune system to recognize and respond to the pathogen.
Live vaccines generally provide longer-lasting immunity and often require fewer doses, but they may not be suitable for people with weakened immune systems. Dead vaccines are safer for immunocompromised individuals but may require booster shots for continued protection.
Live vaccines are designed to be safe, but in rare cases, they can cause mild symptoms similar to the disease. However, they do not cause the full-blown disease in healthy individuals.