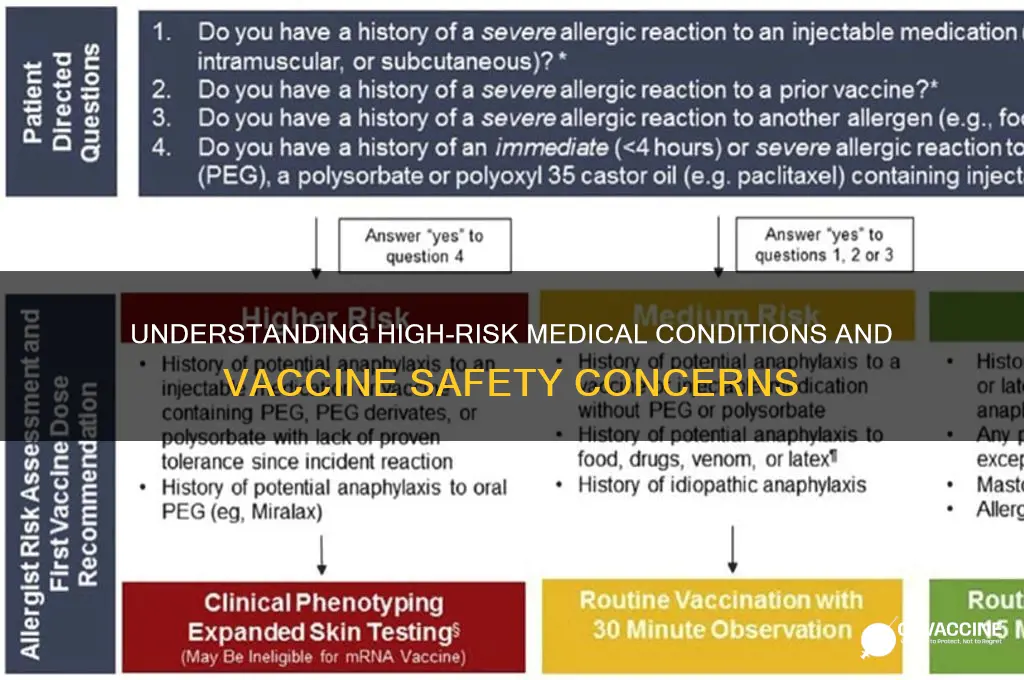
A high-risk medical condition for vaccination refers to underlying health issues that may increase an individual's susceptibility to severe complications from vaccine-preventable diseases or, in some cases, pose challenges when receiving certain vaccines. These conditions can include chronic illnesses such as heart disease, diabetes, lung disease, and weakened immune systems due to conditions like HIV/AIDS, cancer treatments, or organ transplants. Individuals with high-risk medical conditions often require careful consideration and consultation with healthcare providers to determine the most appropriate vaccination schedule and type, ensuring both safety and efficacy. Understanding these conditions is crucial for public health strategies, as it helps prioritize vaccine distribution and tailor immunization programs to protect vulnerable populations effectively.
Explore related products

$19.95 $19.95





What You'll Learn
- Immunocompromised States: Conditions like HIV/AIDS, organ transplants, or cancer treatments weaken immune responses
- Chronic Lung Diseases: Asthma, COPD, or cystic fibrosis increase vaccine complication risks
- Heart Conditions: Severe cardiovascular diseases may elevate risks during vaccination
- Diabetes Complications: Uncontrolled diabetes can worsen vaccine side effects or efficacy
- Neurological Disorders: Conditions like epilepsy or multiple sclerosis require cautious vaccine consideration
![]()
Immunocompromised States: Conditions like HIV/AIDS, organ transplants, or cancer treatments weaken immune responses
Certain medical conditions can significantly impair the body’s immune system, rendering vaccines less effective or even risky. Among these, HIV/AIDS, organ transplants, and cancer treatments stand out as prime examples of immunocompromised states. Individuals living with HIV/AIDS, for instance, often experience a weakened immune system due to the virus’s direct attack on CD4 cells, which are crucial for fighting infections. Similarly, organ transplant recipients must take immunosuppressive medications to prevent organ rejection, but these drugs also suppress the immune response needed for vaccines to work optimally. Cancer treatments, such as chemotherapy and radiation, further exemplify this category, as they target rapidly dividing cells, including those of the immune system, leaving patients vulnerable to infections and less responsive to vaccination.
For those in immunocompromised states, vaccine strategies must be tailored to maximize protection while minimizing risks. For example, individuals with HIV/AIDS may require higher doses or additional booster shots of certain vaccines, such as the influenza or pneumococcal vaccine, to achieve adequate immunity. Transplant recipients often need to time their vaccinations carefully, avoiding live vaccines like the MMR (measles, mumps, rubella) or shingles vaccine, which could pose a risk of infection in their weakened state. Cancer patients undergoing treatment should consult their oncologist to determine the safest window for vaccination, typically after completing chemotherapy or radiation but before immune function declines too severely. Practical tips include keeping a detailed vaccination record and communicating openly with healthcare providers to ensure all necessary precautions are taken.
The interplay between immunocompromised states and vaccine efficacy highlights the need for personalized medical approaches. Studies show that HIV-positive individuals with higher CD4 counts respond better to vaccines, emphasizing the importance of managing the underlying condition before vaccination. For transplant recipients, the type and dosage of immunosuppressive medications can influence vaccine effectiveness, making it essential to monitor these factors closely. Cancer patients, particularly those with hematologic malignancies, may benefit from vaccines administered during remission phases when immune function is relatively stronger. These nuances underscore why a one-size-fits-all vaccine strategy falls short for this population, necessitating individualized care plans.
Despite the challenges, advancements in medical science offer hope for improving vaccine outcomes in immunocompromised individuals. Novel approaches, such as mRNA vaccines, have shown promise in eliciting stronger immune responses even in those with weakened systems. Additionally, adjuvanted vaccines, which include substances to enhance the immune response, are being explored for this population. For instance, the recombinant shingles vaccine (Shingrix) has been found to be safe and effective for immunocompromised adults, including transplant recipients, offering a critical tool in preventing severe complications. As research progresses, healthcare providers must stay informed about these developments to optimize vaccine strategies for their most vulnerable patients.
In practical terms, individuals with immunocompromised states should take proactive steps to protect themselves and those around them. This includes staying up-to-date on recommended vaccines, such as the annual flu shot and COVID-19 boosters, while avoiding unnecessary exposure to illnesses. Household members and close contacts should also be vaccinated to create a protective cocoon, reducing the risk of transmission. Simple measures like frequent handwashing, wearing masks in crowded settings, and avoiding sick individuals can further mitigate risks. By combining medical interventions with everyday precautions, those with weakened immune systems can navigate a world of vaccines more safely and effectively.
Garth Brooks Concert: Vaccination Requirements and Protocols
You may want to see also
Explore related products





![]()
Chronic Lung Diseases: Asthma, COPD, or cystic fibrosis increase vaccine complication risks
Chronic lung diseases such as asthma, chronic obstructive pulmonary disease (COPD), and cystic fibrosis (CF) are not just daily challenges for those who live with them; they also significantly elevate the risk of complications following vaccination. These conditions compromise the respiratory system, making individuals more susceptible to infections and adverse reactions. For instance, during the COVID-19 pandemic, people with these diseases were prioritized for vaccination due to their heightened vulnerability to severe illness, yet the interplay between their lung health and vaccine responses required careful consideration.
Consider asthma, a condition affecting over 25 million Americans, where inflammation and airway hyperresponsiveness can be triggered by various factors, including vaccines. While vaccines are generally safe for asthmatics, certain formulations, such as the influenza vaccine, have been associated with mild exacerbations in a small subset of patients. A 2018 study in the *Journal of Allergy and Clinical Immunology* found that asthmatics experienced a 1.3-fold increased risk of asthma-related hospitalizations within 30 days of flu vaccination, though the overall benefits still outweighed the risks. To mitigate this, healthcare providers often recommend monitoring peak flow rates post-vaccination and having rescue inhalers readily available.
COPD, a progressive disease affecting over 16 million Americans, presents a different set of challenges. The impaired lung function in COPD patients makes them more prone to respiratory infections, and vaccines like the pneumococcal conjugate vaccine (PCV13) and the annual flu shot are critical for prevention. However, these individuals may experience heightened systemic reactions, such as fever or fatigue, due to their compromised immune systems. A 2021 review in *Chest Journal* suggested that COPD patients should receive vaccines in a controlled setting, with follow-up appointments to monitor for exacerbations. Additionally, ensuring proper hydration and rest post-vaccination can help minimize discomfort.
Cystic fibrosis, a genetic disorder affecting roughly 30,000 Americans, further complicates the vaccine landscape. CF patients often have chronic lung infections and are at higher risk of complications from vaccine-preventable diseases. For example, the live attenuated influenza vaccine (LAIV) is contraindicated in CF patients due to the theoretical risk of vaccine-strain virus infection in immunocompromised individuals. Instead, the inactivated influenza vaccine (IIV) is recommended. Moreover, CF patients should adhere to a strict vaccination schedule, including annual flu shots, pneumococcal vaccines (both PCV13 and PPSV23), and COVID-19 vaccines, with careful monitoring for adverse reactions.
Practical tips for managing vaccine risks in chronic lung disease patients include scheduling vaccinations during periods of stable lung function, consulting pulmonologists before receiving live vaccines, and keeping a symptom diary post-vaccination to track any changes. For children with CF, caregivers should ensure vaccines are administered in a pediatric setting with access to emergency care. While vaccines remain a cornerstone of preventive care, tailored approaches are essential for this high-risk population to maximize benefits while minimizing complications.
Hepatitis B Vaccine: Lifelong Protection or Periodic Booster Needed?
You may want to see also
Explore related products





![]()
Heart Conditions: Severe cardiovascular diseases may elevate risks during vaccination
Severe cardiovascular diseases, such as congestive heart failure, coronary artery disease, and cardiomyopathies, can significantly alter the body’s response to vaccines. These conditions often involve compromised immune function, chronic inflammation, or reliance on immunosuppressive medications, which may reduce vaccine efficacy or trigger adverse reactions. For instance, patients with advanced heart failure frequently take medications like beta-blockers or ACE inhibitors, which, while life-saving, can interact with the immune response post-vaccination. Understanding this interplay is critical for healthcare providers when assessing vaccination risks in this population.
Consider the COVID-19 vaccines as a case study. Clinical trials often excluded individuals with severe cardiovascular diseases, leaving a gap in data-driven guidance. However, post-authorization studies suggest that while these vaccines are generally safe for heart patients, certain subgroups, such as those with recent myocardial infarction or unstable angina, may face elevated risks of myocarditis or thromboembolic events. For example, mRNA vaccines (Pfizer-BioNTech, Moderna) have been associated with rare cases of myocarditis, particularly in younger males, though the risk is substantially lower than that posed by COVID-19 infection itself. This highlights the need for individualized risk-benefit analysis.
Practical steps can mitigate risks for heart patients. First, ensure cardiovascular stability before vaccination; postpone if acute decompensation or recent cardiac events (e.g., within 3–6 months) are present. Second, monitor for symptoms like chest pain, shortness of breath, or irregular heartbeat post-vaccination, especially within the first 48 hours. Third, collaborate with cardiologists to adjust medications temporarily if needed, though this should be done cautiously to avoid destabilization. For example, holding anticoagulants briefly before an intramuscular injection might reduce bleeding risk, but this must be weighed against thrombotic risks.
Comparatively, inactivated vaccines (e.g., Sinovac, Sinopharm) may pose fewer risks for heart patients due to their non-replicating nature, but their efficacy is generally lower, requiring additional doses or boosters. Conversely, viral vector vaccines (e.g., AstraZeneca, J&J) carry a rare but serious risk of vaccine-induced immune thrombotic thrombocytopenia (VITT), which is particularly concerning for patients with pre-existing hypercoagulability or atherosclerosis. This underscores the importance of selecting the most appropriate vaccine type based on individual cardiovascular profiles.
The takeaway is clear: severe cardiovascular diseases do not universally contraindicate vaccination, but they necessitate tailored strategies. Healthcare providers should balance the protective benefits of vaccines against potential risks, leveraging patient-specific factors like disease severity, medication regimens, and comorbidities. For instance, a 65-year-old with well-managed hypertension and no recent cardiac events may proceed with standard vaccination protocols, while a 55-year-old with recent heart transplant and ongoing immunosuppression may require reduced doses or alternative vaccine types. Proactive communication and shared decision-making are essential to optimize outcomes for this vulnerable population.
Honest Vaccine Debate: Separating Facts from Fiction in Immunization Discussions
You may want to see also
Explore related products




$18.5 $21.95


![]()
Diabetes Complications: Uncontrolled diabetes can worsen vaccine side effects or efficacy
Uncontrolled diabetes, marked by persistently high blood sugar levels, compromises the immune system’s ability to respond effectively to vaccines. This condition weakens immune cells, reducing their capacity to recognize and combat pathogens. As a result, individuals with poorly managed diabetes may experience diminished vaccine efficacy, leaving them more vulnerable to infections despite vaccination. For example, studies show that flu vaccine effectiveness can drop by up to 20% in people with uncontrolled diabetes compared to those with stable glucose levels. This highlights the critical interplay between glycemic control and immune function.
Beyond reduced efficacy, uncontrolled diabetes can amplify vaccine side effects. Elevated blood sugar levels create a pro-inflammatory state, which may intensify reactions such as fever, fatigue, or injection site pain. For instance, a person with an HbA1c above 9% might experience prolonged soreness or swelling after a COVID-19 vaccine, whereas someone with an HbA1c under 7% typically reports milder symptoms. This heightened sensitivity underscores the importance of managing diabetes before and after vaccination to minimize discomfort and ensure a smoother recovery.
Practical steps can mitigate these risks. First, aim for an HbA1c level below 7% through consistent monitoring, medication adherence, and lifestyle adjustments. Second, consult a healthcare provider to determine the optimal timing for vaccination, ideally during a period of stable glucose control. Third, stay hydrated and monitor blood sugar closely for 48 hours post-vaccination, as stress responses can temporarily elevate glucose levels. For those on insulin, adjust dosages as needed under medical guidance to avoid hypoglycemia or hyperglycemia during this period.
Comparatively, individuals with well-controlled diabetes face fewer vaccine-related challenges. Their immune systems function more robustly, producing adequate antibodies and minimizing adverse reactions. This contrast emphasizes that diabetes itself is not the primary risk factor—it’s the lack of control that exacerbates complications. By prioritizing glycemic management, people with diabetes can align their vaccine outcomes with those of the general population, ensuring both safety and effectiveness.
In conclusion, uncontrolled diabetes poses a dual threat to vaccination: weakened immunity and heightened side effects. However, this risk is manageable through proactive measures. By stabilizing blood sugar levels, staying informed, and collaborating with healthcare providers, individuals with diabetes can optimize their vaccine responses. This approach not only protects personal health but also contributes to broader community immunity, making it a vital strategy for high-risk populations.
San Francisco Vaccine Verification: Easy Steps to Show Proof
You may want to see also
Explore related products



$141.25 $299.99



![]()
Neurological Disorders: Conditions like epilepsy or multiple sclerosis require cautious vaccine consideration
Neurological disorders, such as epilepsy and multiple sclerosis (MS), present unique challenges when it comes to vaccination. These conditions often involve complex immune system interactions and delicate neurological balances, making vaccine decisions a nuanced process. For instance, individuals with epilepsy must consider how vaccine-induced fevers might trigger seizures, while those with MS may worry about potential immune system activation exacerbating their condition. This delicate interplay demands a tailored approach, balancing the protective benefits of vaccines against the risk of adverse reactions.
Analyzing the Risks and Benefits
Vaccines are generally safe and effective, but for those with neurological disorders, the calculus shifts. Epilepsy patients, for example, may experience breakthrough seizures if a vaccine causes a fever, particularly in children under 5 or those with poorly controlled seizures. Similarly, MS patients face concerns about vaccines potentially triggering disease relapses due to immune system stimulation. However, the risk of complications from vaccine-preventable diseases often outweighs these concerns. For instance, influenza can lead to severe complications in MS patients, making annual flu vaccination crucial, though often requiring consultation with a neurologist.
Practical Considerations and Precautions
When vaccinating individuals with neurological disorders, timing and monitoring are critical. For epilepsy patients, administering antipyretics like acetaminophen 30 minutes before vaccination can reduce fever risk. MS patients should avoid live-attenuated vaccines (e.g., MMR, yellow fever) during active relapses but can safely receive inactivated vaccines like the flu shot or COVID-19 mRNA vaccines. Pediatric patients with epilepsy should be closely monitored post-vaccination, particularly after the MMR vaccine, which has a slight association with febrile seizures in young children.
Collaborative Decision-Making
Vaccine decisions for neurological disorders should involve a multidisciplinary approach. Neurologists, primary care providers, and immunologists must collaborate to assess individual risk factors, such as disease severity, medication regimens, and previous vaccine reactions. For MS patients on disease-modifying therapies like ocrelizumab or rituximab, vaccination timing is crucial—ideally before starting treatment or during periods of lower immune suppression. Shared decision-making ensures patients understand the risks and benefits, fostering trust and adherence.
Empowering Patients with Knowledge
Education is key to navigating vaccine decisions for neurological disorders. Patients should be informed about potential side effects, such as temporary seizure activity or MS symptom flare-ups, and how to manage them. For example, keeping a seizure diary post-vaccination can help epilepsy patients track changes. MS patients should be aware of symptoms like increased fatigue or weakness, which may warrant medical attention. Armed with this knowledge, individuals can actively participate in their care, ensuring vaccines are administered safely and effectively.
In conclusion, while neurological disorders require cautious vaccine consideration, they are not contraindications to vaccination. With careful planning, monitoring, and collaboration, individuals with conditions like epilepsy or MS can safely benefit from vaccines, reducing their risk of preventable diseases and associated complications.
Oregon's Vaccine Verification: A Simple Guide to Show Proof
You may want to see also
Frequently asked questions
High-risk medical conditions for vaccines typically include severe allergies (e.g., anaphylaxis), immunocompromised states (e.g., HIV, cancer treatment, organ transplants), certain chronic illnesses (e.g., heart disease, diabetes), and neurological disorders. Always consult a healthcare provider for personalized advice.
Pregnant individuals are not inherently high-risk for vaccines, but certain vaccines (e.g., live attenuated vaccines) may be contraindicated. However, vaccines like the flu shot and Tdap are recommended during pregnancy. Consult a healthcare provider for specific guidance.
Yes, children with asthma can and should be vaccinated, as vaccines do not worsen asthma and can prevent complications from vaccine-preventable diseases. However, those with severe asthma may need extra monitoring during vaccination.
Autoimmune diseases (e.g., rheumatoid arthritis, lupus) are not always high-risk, but individuals with these conditions may need to avoid live vaccines if they are immunocompromised. Consult a healthcare provider to determine the best vaccination plan.