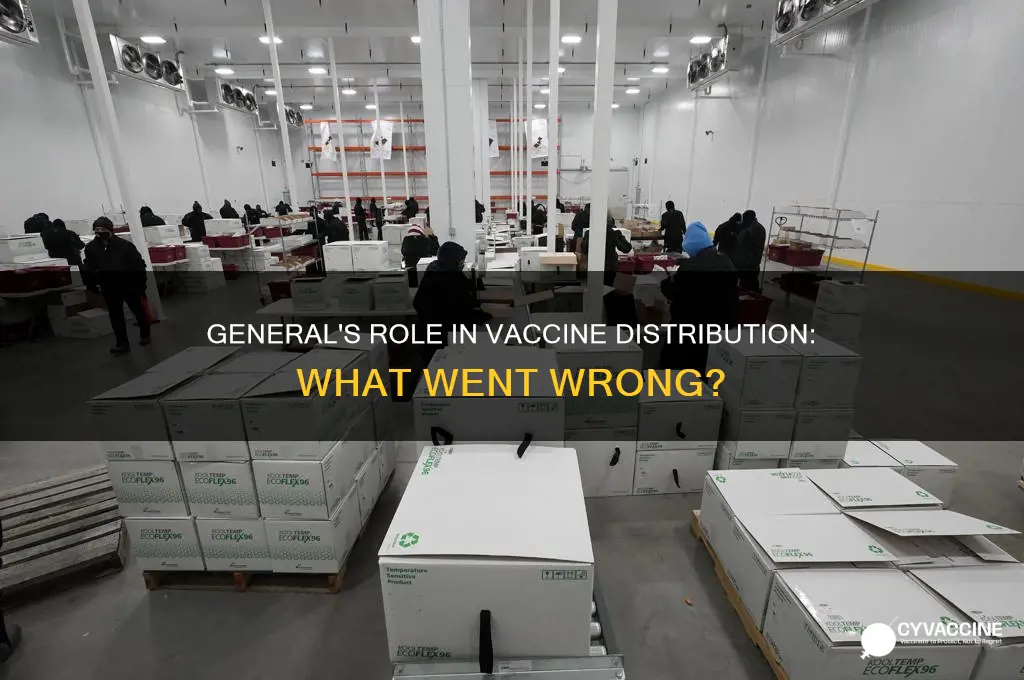
The distribution of the COVID-19 vaccine was a monumental global effort, but it faced significant challenges, particularly in ensuring equitable access and efficient logistics. General distribution strategies varied widely across countries, influenced by factors such as infrastructure, political will, and resource availability. In many nations, governments partnered with pharmaceutical companies, healthcare providers, and international organizations like the World Health Organization (WHO) and COVAX to streamline the process. However, disparities emerged, with wealthier countries securing larger vaccine supplies while low-income nations struggled to access doses. Additionally, logistical hurdles, including cold chain requirements, transportation, and public hesitancy, further complicated the rollout. The role of military and emergency management agencies, often referred to as generals in a metaphorical sense, was crucial in coordinating large-scale vaccination campaigns, ensuring vaccines reached remote areas, and maintaining order at distribution sites. Despite these efforts, the uneven distribution highlighted systemic inequalities, prompting calls for global cooperation and innovative solutions to address the crisis.
Explore related products






What You'll Learn
- Logistical Challenges: Transportation, storage, and distribution networks faced unprecedented hurdles in delivering vaccines globally
- Equity Concerns: Wealthy nations prioritized their populations, leaving poorer countries with limited access
- Supply Chain Issues: Manufacturing delays and raw material shortages slowed vaccine production and distribution
- Public Hesitancy: Misinformation and distrust hindered widespread acceptance and uptake of vaccines
- Government Coordination: Varying policies and strategies among countries impacted global vaccine distribution efficiency
![]()
Logistical Challenges: Transportation, storage, and distribution networks faced unprecedented hurdles in delivering vaccines globally
The COVID-19 vaccine rollout exposed a harsh reality: our global logistics systems, while impressive, were ill-prepared for the unprecedented scale and specificity of this task. Imagine a relay race where the baton is a temperature-sensitive, time-critical cargo, and the runners span continents, each with unique terrain and infrastructure. This was the challenge faced by transportation, storage, and distribution networks tasked with delivering billions of vaccine doses worldwide.
One major hurdle was the "cold chain" requirement. Many COVID-19 vaccines, like Pfizer-BioNTech's, needed ultra-cold storage at -70°C, a temperature unheard of in traditional vaccine distribution. This demanded specialized equipment like dry ice-packed containers and ultra-low temperature freezers, which were in short supply, particularly in low-resource settings.
Consider the logistical ballet required: doses manufactured in Europe needed to reach remote villages in Africa, traversing continents, oceans, and often unreliable road networks. This required meticulous planning, real-time tracking, and coordination between governments, airlines, trucking companies, and healthcare providers.
Every link in this chain was a potential weak point. Delays at customs, power outages disrupting cold storage, or even road closures due to weather could render entire batches of vaccines unusable.
The solution wasn't just about throwing money at the problem. It required innovative approaches. Some countries utilized drones to deliver vaccines to remote areas, while others repurposed existing cold chain infrastructure used for food distribution. COVAX, a global vaccine-sharing initiative, played a crucial role in ensuring equitable access, but even this faced challenges in securing enough doses and navigating complex distribution logistics.
The COVID-19 vaccine rollout was a crash course in global logistics under extreme pressure. It exposed vulnerabilities but also showcased human ingenuity and collaboration. The lessons learned will be invaluable for future pandemics, where the ability to rapidly and equitably distribute life-saving vaccines will be paramount.
Global Vaccine Inequality: Which Nations Lack Access to Life-Saving Doses?
You may want to see also
Explore related products






![]()
Equity Concerns: Wealthy nations prioritized their populations, leaving poorer countries with limited access
The COVID-19 vaccine rollout exposed a stark divide between wealthy and poorer nations, with high-income countries securing the lion’s share of doses early on. By mid-2021, the World Health Organization (WHO) reported that over 80% of vaccines had gone to just three groups: G7 nations, the European Union, and a handful of other wealthy countries. This hoarding left low-income nations scrambling, with some receiving fewer than 10 doses per 100 people even as richer countries administered third and fourth booster shots. The disparity wasn’t just a moral failure—it prolonged the pandemic globally, allowing variants like Delta and Omicron to emerge in under-vaccinated regions and spread worldwide.
Consider the mechanics of this inequity: Wealthy nations pre-purchased billions of doses through advance market commitments, effectively cornering the market before vaccines were even approved. For instance, Canada secured enough doses to vaccinate its population five times over, while many African countries received less than 20% of the doses needed to cover even their most vulnerable populations. COVAX, the global initiative aimed at equitable distribution, was underfunded and outbid by richer nations, delivering only a fraction of its promised doses in 2021. This system prioritized profit and national interest over global health, leaving poorer nations dependent on trickle-down donations of expiring doses.
To address this imbalance, practical steps are needed. Wealthy nations must stop stockpiling excess doses and redirect them to low-income countries immediately. Waiving intellectual property rights for vaccines, as proposed by India and South Africa, could enable local production in poorer regions. Additionally, funding mechanisms like the Pandemic Fund at the World Bank should be scaled up to support infrastructure for vaccine delivery in low-resource settings. For individuals in wealthy nations, advocating for equitable distribution isn’t just altruistic—it’s self-preservation. Until the virus is controlled globally, no one is truly safe.
A comparative analysis highlights the consequences of this inequity. While the U.S. and U.K. achieved over 70% vaccination rates by late 2021, many African countries struggled to reach 10%. This gap wasn’t just about supply—it was about power dynamics. Wealthy nations resisted sharing technology and resources, fearing loss of control over a multi-billion-dollar industry. Meanwhile, the human cost in poorer countries was devastating: higher mortality rates, overwhelmed healthcare systems, and prolonged economic hardship. The lesson is clear: global health crises require global solutions, not fragmented national responses.
Finally, a persuasive argument: Equity in vaccine distribution isn’t a charity act—it’s a strategic imperative. Every unvaccinated person is a potential incubator for new variants, which can render existing vaccines less effective. For example, the Omicron variant, first detected in South Africa, spread rapidly due to low vaccination rates and inadequate global surveillance. Wealthy nations must shift from a zero-sum mindset to a collaborative approach, investing in global vaccination as a public good. Until they do, the pandemic will continue to disrupt lives, economies, and supply chains worldwide, proving that no nation can truly recover alone.
Does Your PPO Cover Vaccines? A Quick Guide to Check
You may want to see also
Explore related products






![]()
Supply Chain Issues: Manufacturing delays and raw material shortages slowed vaccine production and distribution
The COVID-19 pandemic exposed vulnerabilities in global supply chains, and vaccine distribution was no exception. Manufacturing delays and raw material shortages emerged as critical bottlenecks, slowing the production and delivery of life-saving doses. For instance, the lipid nanoparticles essential for encapsulating mRNA in vaccines like Pfizer-BioNTech’s required specialized components, such as ALC-0315 and ALC-0159, which were in limited supply. A single batch of these lipids could take weeks to produce, and any disruption in sourcing these materials from suppliers in countries like Germany or the U.S. halted production lines. This ripple effect meant that even a minor delay in raw material delivery could postpone vaccine shipments by weeks, leaving millions waiting for their doses.
Consider the logistical nightmare of scaling up production for billions of doses. Vaccine manufacturers faced unprecedented demand, requiring them to expand facilities, hire and train staff, and secure additional machinery. For example, Moderna’s initial production capacity was only a fraction of what was needed, and retrofitting their facilities to meet global demand took months. Meanwhile, countries like India, a major producer of vaccines through the Serum Institute, struggled with export bans on critical materials like filters and cell culture media. These delays weren’t just about time—they translated into lives lost, as countries with lower vaccination rates remained vulnerable to outbreaks and new variants.
To address these challenges, governments and companies adopted innovative strategies. The U.S. invoked the Defense Production Act to prioritize raw material production for vaccine makers, ensuring suppliers shifted focus to critical components. Similarly, the European Union established a "Vaccine Export Transparency Mechanism" to monitor and control exports of doses and raw materials, preventing hoarding and ensuring equitable distribution. For individuals, understanding these supply chain complexities highlights the importance of patience and flexibility. If your second dose appointment is delayed, for instance, follow public health guidelines like masking and distancing until you’re fully vaccinated.
A comparative analysis reveals that countries with robust domestic manufacturing capabilities, like the U.S. and China, fared better in securing vaccine supplies. In contrast, low-income nations reliant on imports through COVAX faced prolonged shortages due to export restrictions and prioritization of wealthier countries. This disparity underscores the need for global cooperation in building resilient supply chains. For instance, investing in regional manufacturing hubs in Africa or Southeast Asia could reduce dependency on a few major producers and ensure faster distribution during future crises.
In practical terms, individuals can contribute by staying informed about vaccine availability and being prepared for potential delays. If you’re in a high-risk category (e.g., over 65 or immunocompromised), inquire about booster doses and additional precautions. For parents, ensure children aged 5 and older receive their age-appropriate dosage (typically 10 micrograms for Pfizer, compared to 30 micrograms for adults). Finally, advocate for policies that strengthen global supply chains—whether through funding research, supporting local manufacturing, or promoting equitable distribution. The lessons from these delays are clear: a vaccine’s effectiveness depends not just on its science, but on the systems that deliver it.
Unvaccinated Threats: Diseases Still Lacking Preventive Vaccines Today
You may want to see also
Explore related products






![]()
Public Hesitancy: Misinformation and distrust hindered widespread acceptance and uptake of vaccines
Misinformation spread like a virus during the COVID-19 pandemic, infecting public trust in vaccines. False claims about microchips, infertility, and government control flooded social media, preying on existing anxieties and creating new ones. A single viral post could outweigh years of scientific research in the minds of those already skeptical. For instance, a widely shared myth that the vaccine could alter DNA persisted despite clear evidence that mRNA vaccines never enter the cell nucleus. This misinformation wasn’t just harmless chatter—it directly contributed to delayed vaccinations, particularly among younger age groups (18-39) who were more likely to encounter and share such content online.
Distrust in institutions deepened the divide. Historical injustices, like the Tuskegee Syphilis Study, cast a long shadow over communities of color, where vaccine hesitancy was often rooted in systemic betrayal. In the U.S., Black and Hispanic populations initially lagged in vaccination rates, not due to lack of interest, but because of justified skepticism toward a healthcare system that had repeatedly failed them. Even when vaccines became widely available, many waited months before getting their first dose, often requiring targeted outreach from trusted community leaders to bridge the gap.
Practical barriers exacerbated the issue. Conflicting guidance from health authorities—such as the initial recommendation against vaccinating pregnant individuals, later reversed—sowed confusion. For parents, the lack of immediate approval for children under 12 left families in limbo, with many delaying their own vaccinations until their kids were eligible. Even dosage instructions became a point of contention; the Pfizer vaccine’s two-shot regimen, with a 3-week gap, was harder for some to commit to than the single-dose Johnson & Johnson option, despite its lower efficacy.
To combat hesitancy, strategies had to evolve. Fact-checking alone wasn’t enough; emotional appeals and local testimonials proved more effective. In rural areas, pop-up clinics at churches or farms reached those who wouldn’t visit a hospital. Incentives like gift cards or lottery entries nudged the hesitant, though critics argued this undermined the seriousness of the decision. Ultimately, the lesson is clear: addressing public hesitancy requires understanding its roots—whether historical, logistical, or psychological—and tailoring solutions with empathy and precision.
FIV in Cats: Exploring Vaccination Options and Prevention Strategies
You may want to see also
Explore related products






![]()
Government Coordination: Varying policies and strategies among countries impacted global vaccine distribution efficiency
The COVID-19 pandemic exposed a critical truth: global health crises demand global coordination, yet vaccine distribution became a patchwork of national policies and strategies. This lack of uniformity significantly hindered efficiency, leaving some countries awash in doses while others struggled to secure even a fraction of their needs.
Wealthy nations, prioritizing their own populations, engaged in "vaccine nationalism," stockpiling doses and negotiating exclusive deals with manufacturers. This hoarding delayed access for lower-income countries, exacerbating existing health disparities. For instance, while Canada secured enough doses to vaccinate its population five times over, many African nations received less than 5% of the vaccines needed to reach even 10% coverage.
Consider the contrasting approaches of the European Union and India. The EU, aiming for collective bargaining power, negotiated jointly for vaccines, ensuring a more equitable distribution among member states. India, initially focused on domestic production and export, faced a devastating second wave due to vaccine shortages. This highlights the trade-offs between self-sufficiency and global solidarity.
The COVAX initiative, a global vaccine-sharing mechanism, aimed to address these inequities. However, it faced challenges due to funding shortfalls and vaccine supply constraints. Wealthier nations, having already secured their own doses, were slow to contribute, leaving COVAX struggling to meet its ambitious targets. This underscores the need for binding commitments and transparent mechanisms to ensure fair and timely distribution during future pandemics.
Moving forward, a more coordinated approach is essential. This includes strengthening global health institutions, establishing clear frameworks for vaccine allocation, and fostering international cooperation. Lessons learned from COVID-19 must inform a more equitable and efficient system, where vaccine access is determined by need, not wealth or geopolitical power.
Was Dr. Martin Gore's Death Linked to Vaccines? Facts Revealed
You may want to see also
Frequently asked questions
The general distribution plan for the COVID-19 vaccine involved phased rollouts prioritized by risk groups, such as healthcare workers, the elderly, and those with underlying conditions, followed by the general public as supply increased.
Challenges included supply chain issues, logistical hurdles, vaccine hesitancy, and inequitable access, particularly in low-income countries.
In the U.S., the Centers for Disease Control and Prevention (CDC) and state health departments oversaw distribution, while globally, organizations like the World Health Organization (WHO) and COVAX played key roles.
Delays were caused by manufacturing bottlenecks, transportation issues, cold chain requirements for certain vaccines, and bureaucratic inefficiencies.
The general distribution highlighted disparities, as wealthy nations secured large vaccine supplies while many low-income countries struggled to access doses, leading to initiatives like COVAX to address inequity.