A vaccine with 95% efficacy means that in clinical trials, it reduced the risk of developing the targeted disease by 95% among vaccinated individuals compared to those who received a placebo. This high efficacy rate indicates strong protection, though it doesn't guarantee complete immunity for every individual. Factors like age, underlying health conditions, and virus variants can influence real-world effectiveness. Even with 95% efficacy, some vaccinated people may still contract the disease, but they are likely to experience milder symptoms. This level of protection is crucial for reducing hospitalizations, deaths, and overall disease transmission in populations.
| Characteristics | Values |
|---|---|
| Definition of 95% Efficacy | A vaccine with 95% efficacy reduces the risk of disease by 95% in vaccinated individuals compared to unvaccinated individuals. |
| Clinical Trial Context | Typically based on large-scale Phase 3 clinical trials involving thousands of participants. |
| Reduction in Disease Cases | For every 100 unvaccinated people who get the disease, only 5 vaccinated people would get it. |
| Protection Against Severe Disease | Often provides even higher protection against severe illness, hospitalization, and death. |
| Duration of Protection | Efficacy may wane over time, requiring booster doses for sustained immunity. |
| Real-World Effectiveness | Real-world effectiveness may vary due to factors like virus variants, population behavior, and vaccine uptake. |
| Comparison to Other Vaccines | Among the highest efficacy rates; for example, flu vaccines typically have 40-60% efficacy. |
| Examples of 95% Efficacy Vaccines | Pfizer-BioNTech and Moderna COVID-19 vaccines initially reported ~95% efficacy in trials. |
| Public Health Impact | Significantly reduces disease burden, hospitalizations, and deaths at a population level. |
| Limitations | Does not mean 100% protection; breakthrough infections can still occur. |
Explore related products






What You'll Learn
![]()
Understanding Vaccine Efficacy Rates
Vaccine efficacy rates, often expressed as a percentage, measure how well a vaccine prevents disease in a clinical trial setting. When a vaccine is said to have 95% efficacy, it means that in the study, vaccinated individuals were 95% less likely to develop the disease compared to those who received a placebo. This doesn’t imply perfection—5% of vaccinated participants still contracted the disease—but it underscores a high level of protection. For context, the flu vaccine typically ranges from 40% to 60% efficacy, making 95% a remarkable achievement. Understanding this metric is crucial for interpreting vaccine performance and setting public health expectations.
Consider the COVID-19 vaccines, where 95% efficacy was reported for both the Pfizer-BioNTech and Moderna mRNA vaccines. This rate was calculated by comparing infection rates between vaccinated and unvaccinated groups in trials involving tens of thousands of participants. Importantly, efficacy can vary by population. For instance, older adults or immunocompromised individuals might experience slightly lower protection due to reduced immune responses. Dosage also plays a role: both vaccines require two doses, spaced 3–4 weeks apart for Pfizer and 4 weeks apart for Moderna, to achieve this level of efficacy. Partial vaccination (one dose) offers significantly less protection, emphasizing the need for completing the series.
Efficacy rates aren’t static; they can change based on real-world conditions. For example, the emergence of new variants like Delta or Omicron may reduce a vaccine’s effectiveness against infection, though protection against severe disease often remains robust. This distinction is critical: a vaccine with 95% efficacy against symptomatic illness might still be 90% effective against hospitalization. Public health strategies must account for these nuances, such as recommending booster shots to restore waning immunity or adapting vaccines to target specific variants.
To put efficacy into practical terms, consider a hypothetical community of 10,000 people. Without vaccination, if 2,000 were expected to contract the disease, a 95% efficacious vaccine would reduce that number to 100. This dramatic reduction not only protects individuals but also slows disease spread, a concept known as herd immunity. However, achieving this outcome requires high vaccination rates—typically 70% to 80% of the population, depending on the disease’s contagiousness. For parents, healthcare workers, or policymakers, this underscores the importance of widespread vaccination, even with a highly efficacious vaccine.
Finally, while 95% efficacy is impressive, it’s just one piece of the vaccine evaluation puzzle. Safety, durability of protection, and ease of distribution are equally important. For instance, the Pfizer vaccine’s storage requirement at ultra-cold temperatures initially posed logistical challenges, whereas Moderna’s could be stored in standard refrigerators. When evaluating vaccines, consider efficacy as a starting point, but factor in real-world applicability to make informed decisions. After all, the best vaccine is the one that works effectively and can be widely administered.
New COVID-19 Strain: Vaccine Resistance Concerns and Facts
You may want to see also
Explore related products






![]()
How 95% Efficacy is Measured
A vaccine's 95% efficacy doesn't mean it prevents disease in 95 out of 100 people who receive it. Instead, it's a statistical measure derived from clinical trials comparing vaccinated and unvaccinated groups. Imagine a trial where 20,000 participants receive the vaccine and 20,000 get a placebo. If 100 vaccinated people and 2,000 unvaccinated people contract the disease, the vaccine's efficacy is calculated as (2000 - 100) / 2000 = 95%. This means vaccinated individuals are 95% less likely to develop the disease than those unvaccinated.
Measuring efficacy involves rigorous protocols. Trials typically enroll diverse participants across age groups (e.g., 16–85 years) and health statuses. Participants are randomly assigned to vaccine or placebo groups, often double-blinded to eliminate bias. Researchers monitor both groups for a set period (e.g., 6 months) to track disease incidence. For example, the Pfizer-BioNTech COVID-19 vaccine trial analyzed data after participants received two 30-μg doses, 21 days apart, and were monitored for at least 7 days post-second dose.
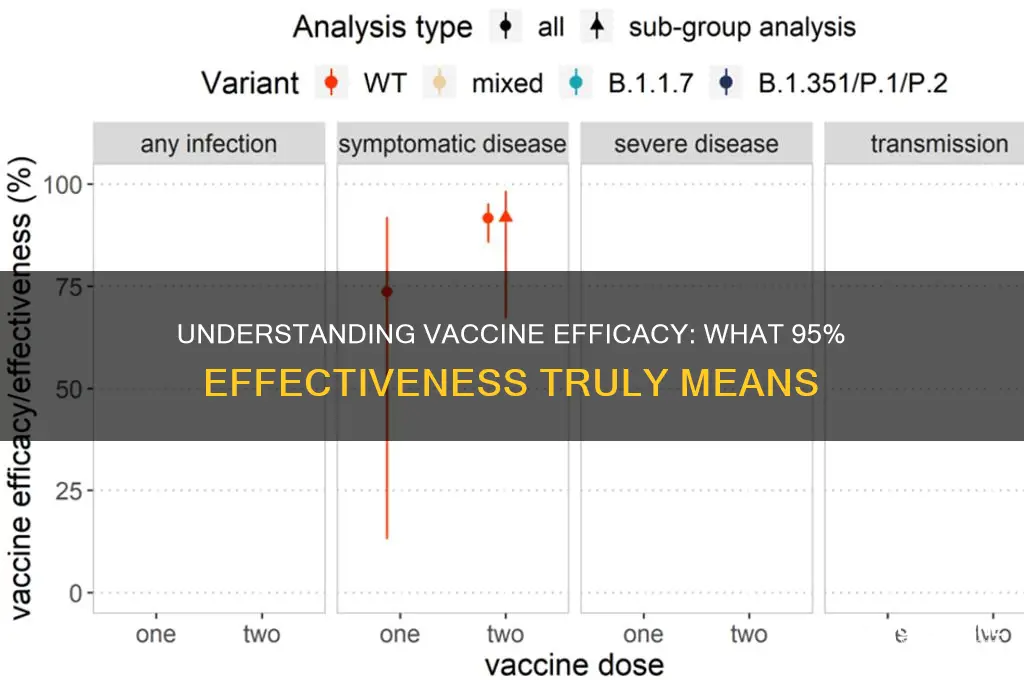
One critical aspect is defining the disease endpoint. For COVID-19 vaccines, efficacy was measured against symptomatic infection, not just any infection. This means the 95% figure refers to preventing illness severe enough to cause symptoms, not asymptomatic cases. Additionally, trials often exclude participants who don’t complete the full dosage regimen or follow-up period, ensuring data accuracy.
Practical tips for understanding efficacy: Look for trial details like sample size, participant demographics, and follow-up duration. Larger, more diverse trials provide stronger evidence. Also, note that real-world efficacy may differ due to factors like variant emergence or inconsistent dosing (e.g., delayed second doses). For instance, while the Moderna vaccine showed 94.1% efficacy in trials, real-world studies reported slightly lower rates due to Delta variant spread.
In summary, 95% efficacy is a snapshot of a vaccine’s performance under controlled conditions, not a guarantee of individual protection. It’s a powerful metric, but interpreting it requires understanding trial design, endpoints, and limitations. Always consult healthcare providers for personalized advice, especially if you’re in a high-risk age group (e.g., over 65) or have underlying conditions.
Ice Skating Rinks: Vaccination Requirements and Rules
You may want to see also
Explore related products






![]()
Real-World vs. Clinical Trial Results
Vaccine efficacy rates, like 95%, are often celebrated as groundbreaking achievements, but these numbers stem from tightly controlled clinical trials. In these studies, participants are carefully selected, often excluding those with comorbidities or extreme ages, and adherence to protocols is meticulously monitored. For instance, the Pfizer-BioNTech COVID-19 vaccine’s 95% efficacy was determined in a trial where participants received two doses, 21 days apart, and were followed for specific endpoints like symptomatic infection. However, real-world conditions introduce variables that trials cannot replicate, such as varying adherence to dosing schedules, diverse population health statuses, and inconsistent healthcare access. This disparity raises a critical question: how do clinical trial results translate—or fail to translate—into real-world effectiveness?
Consider the rollout of the HPV vaccine, which showed over 90% efficacy in trials but faced real-world challenges like incomplete dosing series. Clinical trials typically assume 100% adherence, but in practice, only 54% of U.S. adolescents complete the recommended two-dose regimen within the advised 5-12 month window. Similarly, the influenza vaccine’s efficacy in trials often hovers around 60-70%, yet real-world effectiveness drops to 40-60% due to factors like viral strain mismatches and variable immune responses in older adults. These examples illustrate that while clinical trials provide a benchmark, real-world effectiveness is a dynamic measure influenced by human behavior, environmental factors, and healthcare infrastructure.
To bridge this gap, public health strategies must account for real-world complexities. For instance, extending dosing intervals for certain vaccines, as seen with the AstraZeneca COVID-19 vaccine, can improve accessibility without significantly compromising efficacy. Additionally, targeted education campaigns can address hesitancy and improve adherence, particularly in underserved communities. For example, text message reminders have been shown to increase second-dose uptake by 15% in low-income populations. Practitioners should also emphasize the importance of completing full vaccine series, as partial immunity can lead to suboptimal protection and potential variant emergence.
Ultimately, the 95% efficacy figure is a starting point, not a guarantee. Real-world effectiveness requires ongoing surveillance, adaptive strategies, and a nuanced understanding of population-specific barriers. While clinical trials provide a controlled snapshot of potential, it is the real-world application—shaped by policy, behavior, and biology—that determines a vaccine’s true impact. By acknowledging this distinction, stakeholders can better align expectations, optimize deployment, and maximize public health outcomes.
ACIP Guidelines: Meningitis B Vaccination Recommendations and Key Insights
You may want to see also
Explore related products






![]()
Impact on Transmission Reduction
A vaccine with 95% efficacy doesn’t just protect individuals—it disrupts the chain of infection. This level of effectiveness means that out of every 100 vaccinated people exposed to the virus, only 5 might contract the disease. But the real power lies in how this reduction in individual susceptibility translates to community-wide transmission. When a vaccine prevents 95 out of 100 potential infections, it significantly lowers the number of people who can spread the virus, effectively starving the pathogen of new hosts. This is particularly critical for diseases like COVID-19, where asymptomatic carriers play a major role in transmission.
Consider the practical implications: if a vaccine reduces symptomatic cases by 95%, it also slashes the pool of individuals shedding the virus. For instance, in a population of 1,000 vaccinated people, only 50 might become infected instead of 1,000 without vaccination. Fewer infections mean fewer opportunities for the virus to mutate, reducing the risk of new variants emerging. This is why high-efficacy vaccines like Pfizer-BioNTech (95% efficacy in clinical trials) or Moderna (94.1%) have been game-changers in controlling pandemics. However, achieving this impact requires high vaccination rates—typically 70–85% of the population—to create herd immunity and further suppress transmission.
To maximize transmission reduction, timing and dosage matter. For mRNA vaccines, a two-dose regimen spaced 3–4 weeks apart is essential to achieve peak efficacy. For example, Pfizer’s efficacy jumps from 52% after one dose to 95% after the second. Booster shots, administered 6–12 months later, maintain this protection, especially against waning immunity or new variants. Age also plays a role: while efficacy is consistently high across adults, it may vary in older populations or immunocompromised individuals, requiring tailored strategies like additional doses or adjuvanted vaccines.
One caution: even a 95% effective vaccine isn’t a guarantee of zero transmission. Breakthrough infections, though rare, can still occur, and vaccinated individuals might carry and spread the virus, albeit at lower viral loads. This underscores the need for complementary measures like masking and testing, especially in high-risk settings. For instance, healthcare workers or those in crowded environments should continue precautions until community transmission is minimal.
In conclusion, a 95% efficacious vaccine is a powerful tool for transmission reduction, but its success hinges on widespread uptake, proper dosing, and layered prevention strategies. It’s not just about protecting oneself—it’s about breaking the virus’s path through the population. By understanding this dynamic, individuals and policymakers can make informed decisions to turn high efficacy into real-world impact.
Inoculation vs. Vaccine: Understanding the Key Differences and Similarities
You may want to see also
Explore related products






![]()
Limitations of High Efficacy Vaccines
A 95% efficacy rate for a vaccine sounds impressive, but it doesn't guarantee universal protection. This figure means that in a controlled trial, 95% of vaccinated individuals were protected from the disease compared to those who received a placebo. However, real-world scenarios introduce variables that can diminish this effectiveness. For instance, the Pfizer-BioNTech COVID-19 vaccine showed 95% efficacy in trials, yet breakthrough infections still occurred, particularly as new variants emerged and immunity waned over time. This highlights the first limitation: efficacy is a snapshot, not a guarantee, and it’s influenced by factors like viral evolution and individual immune responses.
Consider the role of population variability in vaccine efficacy. A 95% efficacy rate is an average, meaning some groups may experience lower protection. For example, older adults or immunocompromised individuals often mount weaker immune responses, even to highly effective vaccines. The shingles vaccine, Shingrix, boasts over 90% efficacy in clinical trials but is less effective in those over 70 due to age-related immune decline. Similarly, the influenza vaccine’s efficacy varies annually, typically ranging from 40–60%, because it must be reformulated to match circulating strains. This variability underscores the importance of tailoring vaccination strategies to specific demographics and health conditions.
Another limitation lies in logistical and behavioral factors. Even a vaccine with 95% efficacy can falter if not administered correctly or if coverage is insufficient. For instance, the two-dose regimen of the Moderna COVID-19 vaccine requires a 28-day interval for optimal efficacy. Deviating from this schedule can reduce effectiveness. Additionally, herd immunity—critical for protecting vulnerable populations—relies on high vaccination rates. If only 70% of a population receives a 95% effective vaccine, the overall protection drops significantly, leaving room for outbreaks. This demonstrates that efficacy alone cannot compensate for gaps in distribution, adherence, or uptake.
Finally, efficacy versus effectiveness reveals a critical limitation. Efficacy is measured under ideal conditions, while effectiveness reflects real-world performance. The rotavirus vaccine, Rotarix, showed 95% efficacy in trials but had lower effectiveness in low-income countries due to factors like malnutrition and concurrent infections. Similarly, the HPV vaccine’s efficacy in preventing cervical cancer is high, but its real-world impact depends on vaccination rates and screening practices. Bridging this gap requires addressing systemic barriers, such as access, education, and infrastructure, to ensure vaccines perform as intended outside controlled settings.
In summary, while a 95% efficacy rate is a remarkable achievement, it’s not without limitations. Population variability, logistical challenges, and the difference between controlled trials and real-world conditions all play a role in reducing a vaccine’s impact. Understanding these constraints is crucial for setting realistic expectations and designing strategies that maximize the benefits of high-efficacy vaccines. Practical steps, such as adhering to dosing schedules, targeting vulnerable groups, and improving global access, can help mitigate these limitations and ensure vaccines fulfill their potential.
Celiac Disease, Autoimmunity, and Vaccines: Unraveling the Complex Connection
You may want to see also
Frequently asked questions
A vaccine with 95% efficacy means that in clinical trials, it reduced the risk of developing the disease by 95% among vaccinated individuals compared to those who received a placebo.
No, it means that overall, the vaccine reduces the risk of disease by 95% across the entire vaccinated population, not that it works perfectly for 95% of people and not at all for the remaining 5%.
Yes, while the vaccine significantly reduces the risk, it does not eliminate it entirely. A small percentage of vaccinated individuals may still contract the disease, but their symptoms are often milder.
Efficacy rates are typically based on the dominant strain(s) during clinical trials. The vaccine’s effectiveness against new variants may vary, and ongoing research is needed to determine its performance against emerging strains.
A 95% efficacy rate is exceptionally high compared to many other vaccines, such as the flu vaccine, which typically ranges from 40% to 60% efficacy depending on the season and strain match.