A vaccine that contains a dead or inactivated virus is commonly referred to as an inactivated vaccine. Unlike live-attenuated vaccines, which use a weakened form of the virus, inactivated vaccines use a version of the virus that has been killed through chemical or physical processes, rendering it unable to replicate or cause disease. This type of vaccine still triggers an immune response, allowing the body to recognize and develop antibodies against the virus, thereby providing protection against future infections. Examples of inactivated vaccines include those for polio, hepatitis A, and rabies. Their safety profile makes them suitable for individuals with weakened immune systems, as there is no risk of the virus reverting to a disease-causing form.
Explore related products






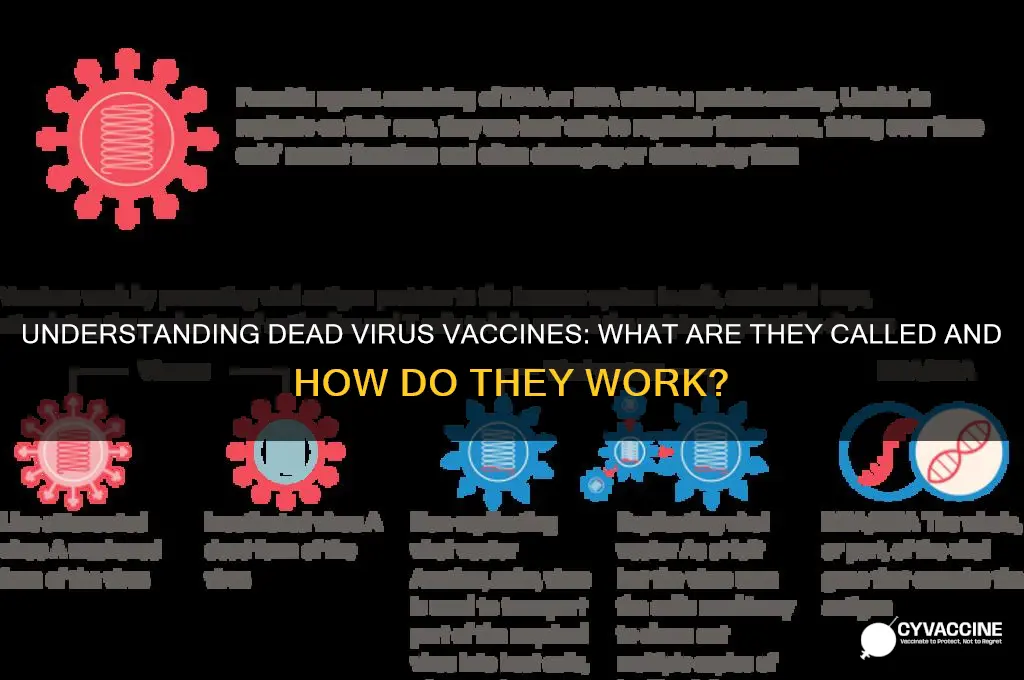
What You'll Learn
- Inactivated Vaccines: Contain killed pathogens, unable to replicate, but trigger immune response safely
- Examples: Polio (IPV), Hepatitis A, Rabies vaccines use dead viruses effectively
- Safety: Stable, cannot cause disease, ideal for immunocompromised individuals
- Efficacy: Requires multiple doses or adjuvants to boost immune response
- Storage: Often more stable, less stringent refrigeration requirements compared to live vaccines
![]()
Inactivated Vaccines: Contain killed pathogens, unable to replicate, but trigger immune response safely
Inactivated vaccines, often referred to as "killed vaccines," are a cornerstone of modern immunization strategies. Unlike live-attenuated vaccines, which use weakened but still active pathogens, inactivated vaccines contain pathogens that have been completely destroyed, rendering them incapable of replicating within the body. This key difference makes them an ideal choice for individuals with compromised immune systems or those at higher risk of adverse reactions. For instance, the inactivated polio vaccine (IPV) has been instrumental in nearly eradicating polio worldwide, offering a safer alternative to the oral polio vaccine (OPV), which uses a live virus.
The process of creating inactivated vaccines involves treating pathogens—such as viruses or bacteria—with chemicals, heat, or radiation to destroy their ability to cause disease. Despite being "dead," these pathogens retain their antigenic properties, allowing them to trigger a robust immune response. This response includes the production of antibodies and the activation of immune cells, which prepare the body to recognize and combat the actual pathogen if exposed in the future. For example, the influenza vaccine, often administered annually, is typically an inactivated vaccine that protects against specific strains of the flu virus.
One of the most significant advantages of inactivated vaccines is their safety profile. Because the pathogens are dead, there is no risk of the vaccine causing the disease it aims to prevent. This makes them suitable for a wide range of populations, including infants, the elderly, and immunocompromised individuals. For instance, the hepatitis A vaccine, an inactivated vaccine, is recommended for children starting at 12 months of age and for adults at risk of exposure. However, inactivated vaccines often require multiple doses to achieve full immunity, as the initial immune response may not be as strong as that triggered by live vaccines.
Despite their safety, inactivated vaccines are not without limitations. Their inability to replicate means they may not stimulate the same level of cellular immunity as live vaccines, which can limit their effectiveness against certain diseases. Additionally, adjuvants—substances added to enhance the immune response—are often required to improve their efficacy. For example, the COVID-19 vaccines developed by Sinovac and Sinopharm are inactivated vaccines that use aluminum hydroxide as an adjuvant to boost immune response. Practical tips for recipients include staying hydrated, monitoring for mild side effects like soreness at the injection site, and adhering to the recommended dosing schedule, typically two doses administered 2–4 weeks apart.
In summary, inactivated vaccines offer a safe and effective means of protection against numerous diseases by using killed pathogens to stimulate immunity without the risk of infection. Their broad applicability, particularly for vulnerable populations, makes them a vital tool in public health. While they may require multiple doses and adjuvants to optimize their effectiveness, their proven track record in preventing diseases like polio, hepatitis A, and influenza underscores their importance in global vaccination efforts. Understanding their mechanism and limitations empowers individuals to make informed decisions about their health and vaccination choices.
Vaccinated and a Carrier: Is It Possible?
You may want to see also
Explore related products




![USA Air Force 43Rd Airlift Wing Inactivated March 2011 Pope Field [Af-039]](https://m.media-amazon.com/images/I/81OZmUgo7BL._AC_UY218_.jpg)
![]()
Examples: Polio (IPV), Hepatitis A, Rabies vaccines use dead viruses effectively
Vaccines with dead viruses, known as inactivated vaccines, have been pivotal in preventing severe diseases by using pathogens rendered non-infectious through chemical or physical methods. Among the most successful examples are the Polio (IPV), Hepatitis A, and Rabies vaccines, each demonstrating the effectiveness of this approach in different contexts. These vaccines not only protect individuals but also contribute to global health by reducing disease prevalence and supporting herd immunity.
Consider the Polio (IPV) vaccine, a cornerstone of eradication efforts. Administered as an injection, IPV contains three types of inactivated poliovirus, offering robust protection against all strains. The CDC recommends a four-dose series starting at 2 months of age, with doses given at 2, 4, 6–18 months, and 4–6 years. Unlike the oral polio vaccine (OPV), IPV eliminates the rare risk of vaccine-derived poliovirus cases, making it safer for routine immunization. Its success is evident in the near-global eradication of polio, with cases dropping by over 99% since 1988.
The Hepatitis A vaccine is another prime example, using inactivated virus to provide long-term immunity against this liver infection. Typically given in a two-dose series, 6–12 months apart, it is recommended for children over 12 months, travelers to endemic areas, and individuals with chronic liver disease. A single dose provides up to 94% protection within a month, rising to nearly 100% after the second dose. This vaccine has drastically reduced Hepatitis A cases in countries with widespread immunization programs, such as the U.S., where incidence has fallen by 95% since the 1990s.
For Rabies, a nearly 100% fatal disease, the inactivated vaccine is a lifesaver. It is administered in a series of three doses over 28 days for pre-exposure prophylaxis, primarily for veterinarians, travelers, and lab workers. Post-exposure treatment combines the vaccine with rabies immunoglobulin for immediate protection. Unlike other vaccines, Rabies immunization is uniquely effective even after exposure, provided it is administered promptly. This highlights the versatility of inactivated vaccines in both prevention and emergency response.
Practical tips for maximizing the benefits of these vaccines include adhering to recommended schedules, storing vaccines properly (typically refrigerated), and monitoring for rare side effects like soreness at the injection site. For travelers, consulting a healthcare provider 4–6 weeks before departure ensures timely vaccination. These examples underscore the reliability and adaptability of inactivated vaccines in combating diverse diseases, making them indispensable tools in public health.
Air Travel and Vaccination: What's the Connection?
You may want to see also
Explore related products


![]()
Safety: Stable, cannot cause disease, ideal for immunocompromised individuals
A vaccine containing a dead virus, often referred to as an inactivated vaccine, offers a unique safety profile that sets it apart from other vaccine types. The key advantage lies in its stability and inability to revert to a disease-causing form. This characteristic makes it an ideal choice for individuals with compromised immune systems, who are often at higher risk of adverse reactions from other vaccine types.
From an analytical perspective, the safety of inactivated vaccines stems from the process of virus inactivation, typically achieved through chemical or physical methods. This ensures the virus particles are destroyed and cannot replicate, eliminating the risk of infection. For instance, the inactivated polio vaccine (IPV) has been widely used since the 1980s, providing a safe and effective alternative to the live oral polio vaccine, particularly for immunocompromised individuals. A standard IPV dose contains 40 D-antigen units of each poliovirus type, administered intramuscularly or subcutaneously, often as part of a combination vaccine.
When considering the practical application, it’s essential to follow specific guidelines for administering inactivated vaccines to immunocompromised patients. These individuals, including those with HIV, cancer, or organ transplants, may have reduced immune responses but still require protection against vaccine-preventable diseases. For example, the influenza vaccine, available in inactivated forms such as the flu shot, is recommended annually for this population. The standard dose for adults is 0.5 mL, while children aged 6 months to 3 years receive 0.25 mL per dose, with a two-dose series for first-time recipients.
A comparative analysis highlights the advantages of inactivated vaccines over live-attenuated vaccines for immunocompromised individuals. Live vaccines, such as the measles-mumps-rubella (MMR) vaccine, carry a small risk of causing disease in those with weakened immunity. In contrast, inactivated vaccines like the hepatitis A vaccine (Havrix or Vaqta) provide a safer alternative, with a typical adult dose of 1 mL administered intramuscularly in a two-dose series. This makes inactivated vaccines a preferred choice for high-risk populations, ensuring protection without the risk of vaccine-induced illness.
In conclusion, the stability and safety of inactivated vaccines make them indispensable for immunocompromised individuals. By understanding their unique properties and following specific dosing guidelines, healthcare providers can effectively protect vulnerable populations against infectious diseases. Practical tips include ensuring timely vaccination, monitoring for mild side effects (e.g., soreness at the injection site), and consulting with specialists for personalized vaccine schedules. This approach maximizes safety while providing essential immunity to those who need it most.
The Truth About Luke Perry's Death and Pneumonia Vaccine
You may want to see also
![]()
Efficacy: Requires multiple doses or adjuvants to boost immune response
A vaccine containing a dead virus, often referred to as an inactivated vaccine, relies on a pathogen that has been killed or rendered non-infectious through chemical or physical processes. While this approach ensures safety by eliminating the risk of the virus replicating in the body, it often presents a challenge: the immune system may not respond as robustly to the dead virus as it would to a live, attenuated one. This diminished response necessitates strategies to enhance efficacy, such as administering multiple doses or incorporating adjuvants.
Consider the inactivated polio vaccine (IPV), a prime example of this category. Unlike the oral polio vaccine (OPV), which uses a weakened live virus, IPV requires a series of doses to build sufficient immunity. The Centers for Disease Control and Prevention (CDC) recommends a four-dose schedule for children: at 2 months, 4 months, 6–18 months, and 4–6 years. This repeated exposure ensures the immune system encounters the antigen multiple times, gradually mounting a stronger defense. Adults traveling to polio-endemic regions may also require a booster dose, underscoring the need for multiple administrations to maintain protection.
Adjuvants play a critical role in amplifying the immune response to inactivated vaccines. These substances, such as aluminum salts (alum), are added to the vaccine formulation to stimulate the immune system more effectively. For instance, the hepatitis A vaccine, an inactivated virus vaccine, often includes alum to enhance its efficacy. Studies show that adjuvanted vaccines can reduce the number of required doses while achieving comparable immunity. However, the choice of adjuvant must be carefully considered, as some may cause localized reactions, such as redness or swelling at the injection site.
Practical considerations for administering inactivated vaccines with multiple doses or adjuvants include adherence to the recommended schedule and monitoring for adverse effects. For parents, maintaining a vaccination record and setting reminders for follow-up doses are essential steps to ensure full protection. Healthcare providers should educate patients about the importance of completing the series, as partial vaccination may leave individuals vulnerable. Additionally, storing vaccines properly—typically between 2°C and 8°C—is critical to preserving their efficacy, especially for adjuvanted formulations.
In conclusion, while inactivated vaccines offer a safe alternative to live vaccines, their efficacy often hinges on strategic interventions like multiple doses or adjuvants. Understanding these mechanisms empowers individuals and healthcare providers to optimize immunization outcomes. Whether it’s the polio vaccine’s four-dose regimen or the adjuvanted hepatitis A vaccine, these approaches highlight the balance between safety and immune stimulation in modern vaccinology.
Lyme Disease Vaccination for Pets: Optimal Frequency and Timing Explained
You may want to see also
![]()
Storage: Often more stable, less stringent refrigeration requirements compared to live vaccines
Dead or inactivated vaccines, such as those for polio, rabies, and hepatitis A, offer a distinct advantage in storage and handling. Unlike live attenuated vaccines, which require a continuous cold chain to maintain efficacy, inactivated vaccines are more robust. This stability stems from the fact that the viruses are no longer viable, reducing the risk of degradation at higher temperatures. For instance, the inactivated polio vaccine (IPV) can be stored between 2°C and 8°C, similar to a standard refrigerator, whereas live oral polio vaccine (OPV) demands stricter temperature control to prevent potency loss.
This leniency in storage requirements translates to practical benefits, especially in resource-limited settings. Health workers can transport and store inactivated vaccines without the constant worry of temperature excursions, which can render live vaccines ineffective. For example, the hepatitis A vaccine, Havrix, remains stable for up to 24 months when refrigerated, allowing for flexible distribution schedules. In contrast, live vaccines like the measles, mumps, and rubella (MMR) vaccine must be kept frozen until reconstitution, complicating logistics and increasing costs.
Consider the implications for vaccination campaigns in remote areas. Inactivated vaccines can be pre-positioned in basic storage facilities, reducing the need for expensive cold chain infrastructure. This is particularly critical for rabies vaccines, which are often administered post-exposure in rural settings. A single dose of the inactivated rabies vaccine, stored properly, can be a lifesaver without the logistical hurdles of live vaccines. However, it’s essential to follow manufacturer guidelines—even inactivated vaccines have limits, and exposure to extreme temperatures can still compromise their effectiveness.
For healthcare providers, understanding these storage differences can streamline operations. Inactivated vaccines often come in multi-dose vials, which, once opened, can remain viable for weeks if stored correctly. For example, the influenza vaccine, often inactivated, can be kept in a refrigerator for up to 30 days after the first dose is drawn. This reduces waste and ensures more patients can be vaccinated from a single vial. In contrast, live vaccines like the varicella vaccine typically require immediate use or discard after reconstitution, increasing the pressure on vaccination schedules.
In summary, the stability of inactivated vaccines simplifies storage and distribution, making them a reliable choice for global health initiatives. By requiring less stringent refrigeration, these vaccines reduce the logistical burden on healthcare systems, particularly in challenging environments. Whether for routine immunization or emergency response, understanding and leveraging this advantage can enhance vaccine accessibility and efficacy. Always consult specific product guidelines, but rest assured: inactivated vaccines offer a practical edge in the fight against disease.
Ohio's COVID-19 Vaccination Progress: How Many Residents Are Protected?
You may want to see also
Frequently asked questions
A vaccine with a dead virus is called an inactivated vaccine.
An inactivated vaccine uses a killed version of the virus to stimulate the immune system to produce antibodies without causing the disease.
Yes, inactivated vaccines are generally considered safe because the virus is dead and cannot cause the disease it protects against.
Examples include the polio (IPV), hepatitis A, and rabies vaccines.