Vaccinated and unvaccinated individuals, despite their differing choices regarding immunization, share several commonalities that often go unnoticed. Both groups are part of the same communities, workplaces, and social networks, facing similar daily challenges and responsibilities. Regardless of vaccination status, all individuals are susceptible to various health risks, environmental factors, and societal pressures. Additionally, both vaccinated and unvaccinated people contribute to the broader public health landscape, whether through healthcare utilization, economic participation, or community engagement. Understanding these shared experiences can foster empathy and dialogue, highlighting that the complexities of health decisions extend beyond vaccination alone.
Explore related products

$37.1 $39.95





What You'll Learn
- Both groups can still contract and spread diseases, though severity may differ
- Vaccinated and unvaccinated individuals share common health risks unrelated to vaccines
- Both rely on herd immunity for protection against certain infectious diseases
- Vaccinated and unvaccinated people can experience vaccine side effects or natural symptoms
- Both groups contribute to ongoing public health surveillance and data collection efforts
![]()
Both groups can still contract and spread diseases, though severity may differ
Vaccines are not an impenetrable shield against disease. Both vaccinated and unvaccinated individuals can still contract and spread pathogens, a fact often misunderstood in public discourse. This shared vulnerability stems from the complex interplay between vaccine efficacy, individual immune responses, and the evolving nature of pathogens. While vaccines significantly reduce the risk of infection and severe outcomes, they do not confer absolute immunity. For instance, the COVID-19 vaccines, depending on the type and dosage (e.g., a two-dose series of mRNA vaccines or a single-dose adenovirus vector vaccine), provide robust protection against severe illness and hospitalization but do not entirely prevent transmission, especially with the emergence of new variants.
Consider the mechanics of vaccine-induced immunity. Vaccines train the immune system to recognize and combat specific pathogens, but this process is not foolproof. Breakthrough infections occur when vaccinated individuals contract the disease, often due to waning immunity over time or exposure to highly transmissible variants. For example, studies show that six months after receiving the second dose of an mRNA COVID-19 vaccine, protection against infection may drop from 95% to around 60–70%, though protection against severe disease remains high. Similarly, unvaccinated individuals, lacking this immune priming, are more susceptible to infection but can still spread the disease, particularly if they are asymptomatic or presymptomatic.
The ability to spread disease is not solely determined by vaccination status. Viral load, the amount of virus present in an infected person, plays a critical role in transmission. Vaccinated individuals with breakthrough infections tend to have lower viral loads compared to unvaccinated individuals, reducing but not eliminating their potential to spread the disease. For instance, a study published in *The Lancet* found that vaccinated individuals with breakthrough COVID-19 infections had viral loads comparable to unvaccinated individuals in the first few days of infection, though their viral loads declined more rapidly. This highlights the importance of additional preventive measures, such as masking and testing, regardless of vaccination status.
Practical steps can mitigate the risk of transmission in both groups. For vaccinated individuals, staying up-to-date with booster doses is essential to maintain optimal immunity. For example, a COVID-19 booster shot administered 5–6 months after the initial series can restore vaccine efficacy to over 90% against severe disease and hospitalization. Unvaccinated individuals should prioritize behaviors that reduce exposure, such as avoiding crowded indoor spaces and practicing good hand hygiene. Both groups should monitor for symptoms and isolate if exposed or infected, as asymptomatic spread remains a concern. Testing, particularly with rapid antigen tests, can help identify infections early, even in vaccinated individuals who may experience milder symptoms.
In conclusion, the shared susceptibility to contracting and spreading diseases underscores the need for a nuanced approach to public health. Vaccination remains a cornerstone of disease prevention, but it is not a standalone solution. Understanding the limitations of vaccines and adopting layered preventive strategies can help protect both individuals and communities. Whether vaccinated or unvaccinated, everyone plays a role in breaking the chain of transmission, emphasizing the collective responsibility in managing infectious diseases.
Vaccinated vs. Unvaccinated Playdates: Balancing Safety and Socialization for Kids
You may want to see also
Explore related products






![]()
Vaccinated and unvaccinated individuals share common health risks unrelated to vaccines
Both vaccinated and unvaccinated individuals face a myriad of health risks that vaccines neither cause nor prevent. Consider the omnipresent threat of chronic diseases like diabetes and hypertension, which affect millions regardless of their immunization status. According to the Centers for Disease Control and Prevention (CDC), over 34 million Americans have diabetes, and nearly half of U.S. adults suffer from hypertension. These conditions stem from lifestyle factors such as poor diet, sedentary behavior, and genetic predisposition, not from vaccine choices. For instance, consuming more than 2,300 mg of sodium daily increases hypertension risk, while a diet high in processed sugars correlates with insulin resistance. Practical steps like reducing sugar intake, increasing physical activity, and monitoring blood pressure can mitigate these risks for everyone, irrespective of vaccination status.
Environmental hazards pose another shared risk, transcending the vaccinated-unvaccinated divide. Air pollution, for example, contributes to respiratory and cardiovascular diseases globally. The World Health Organization (WHO) estimates that 9 out of 10 people breathe air exceeding WHO guideline limits, leading to 7 million premature deaths annually. Fine particulate matter (PM2.5) from vehicle emissions, industrial activities, and wildfires infiltrates the lungs and bloodstream, causing inflammation and oxidative stress. Vaccines offer no protection against these pollutants. Instead, actionable measures like using air purifiers indoors, wearing masks during high pollution days, and advocating for cleaner energy policies benefit all individuals equally.
Mental health challenges, such as anxiety and depression, also affect vaccinated and unvaccinated populations alike. The National Institute of Mental Health reports that nearly 1 in 5 U.S. adults experience mental illness each year, driven by factors like stress, trauma, and socioeconomic instability. Vaccination status plays no role in these conditions. Evidence-based strategies such as cognitive-behavioral therapy, mindfulness practices, and maintaining social connections can improve mental well-being for everyone. For instance, dedicating 10–15 minutes daily to meditation or journaling has been shown to reduce stress hormone levels by up to 14%.
Infectious diseases not targeted by vaccines further highlight this common ground. Norovirus, for example, causes 19–21 million illnesses annually in the U.S., leading to severe dehydration and hospitalization, particularly in children under 5 and adults over 65. Similarly, antibiotic-resistant infections like MRSA affect over 80,000 Americans yearly, regardless of vaccination history. Prevention relies on universal hygiene practices: washing hands with soap for at least 20 seconds, disinfecting high-touch surfaces, and practicing safe food handling. These measures, not vaccines, are the primary defense against such pathogens.
Finally, occupational hazards expose both groups to health risks. Healthcare workers, for instance, face needle-stick injuries, long-term back pain from patient lifting, and burnout from high-stress environments. Construction workers encounter asbestos exposure, falls, and respiratory issues from dust inhalation. Vaccines are irrelevant in these scenarios. Employers and employees can reduce risks through ergonomic training, providing personal protective equipment (PPE), and enforcing safety protocols. For example, using lifting aids can decrease back injury rates by 60%, while N95 masks filter out 95% of airborne particles in dusty environments. Addressing these shared risks requires collective action, not individual vaccine decisions.
Effective Ways to Reduce Swollen Lymph Nodes Post-Vaccination
You may want to see also
Explore related products






![]()
Both rely on herd immunity for protection against certain infectious diseases
Herd immunity, a concept often misunderstood, is a critical shield against infectious diseases, and both vaccinated and unvaccinated individuals stand under its protection. This phenomenon occurs when a significant portion of a population becomes immune to a disease, thereby reducing the likelihood of infection for those who lack immunity. For vaccinated individuals, this means their immunization contributes to the collective defense, while the unvaccinated benefit from the reduced circulation of pathogens. Consider measles, a highly contagious disease where herd immunity requires approximately 95% vaccination coverage to protect the vulnerable.
Achieving herd immunity involves more than just individual vaccination decisions; it’s a community effort. Vaccinated individuals play a direct role by reducing the spread of disease, while the unvaccinated indirectly rely on this barrier to avoid exposure. For instance, infants too young to receive certain vaccines (under 12 months for measles) depend on herd immunity for protection. Similarly, immunocompromised individuals who cannot be vaccinated rely on the community’s immunity to safeguard them. This interdependence highlights the shared responsibility in maintaining public health.
However, herd immunity is fragile and requires consistent adherence to vaccination schedules. A single missed dose can lower immunity levels, leaving gaps for outbreaks. For example, the MMR vaccine (measles, mumps, rubella) requires two doses, with the first administered at 12–15 months and the second at 4–6 years. Skipping the second dose reduces effectiveness from 97% to 93%, insufficient for herd immunity against measles. Both vaccinated and unvaccinated populations must understand that incomplete vaccination weakens this protective barrier for everyone.
Practical steps to strengthen herd immunity include staying updated on vaccinations, especially for diseases like pertussis (whooping cough) and influenza, which require periodic boosters. Unvaccinated individuals can contribute by practicing good hygiene, avoiding crowded areas during outbreaks, and supporting public health policies that promote vaccination access. For parents, ensuring children receive vaccines on schedule is crucial, as delays increase the risk of exposure. Ultimately, whether vaccinated or not, everyone shares the responsibility of sustaining herd immunity to protect the most vulnerable among us.
Florida Vaccine Application Guide: Steps to Secure Your COVID-19 Shot
You may want to see also
Explore related products






![]()
Vaccinated and unvaccinated people can experience vaccine side effects or natural symptoms
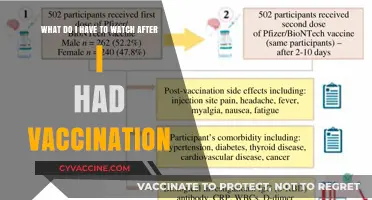
Both vaccinated and unvaccinated individuals can experience a range of symptoms that may overlap, blurring the lines between vaccine side effects and natural illness manifestations. For instance, fever, fatigue, and headaches are common responses to vaccination, particularly after receiving mRNA vaccines like Pfizer-BioNTech or Moderna, where up to 50-60% of recipients report systemic reactions after the second dose. Yet, these same symptoms are hallmark indicators of viral infections such as influenza or COVID-19, which unvaccinated individuals are more susceptible to contracting. This similarity complicates self-diagnosis, as a vaccinated person’s fever could stem from immune activation post-vaccine, while an unvaccinated person’s fever might signal an active infection.
Consider the scenario of a 35-year-old vaccinated individual who develops a sore throat and muscle aches 48 hours after their booster shot. These symptoms align with known vaccine side effects, typically peaking within 1-2 days post-vaccination and resolving within a week. Conversely, an unvaccinated 35-year-old with identical symptoms might be experiencing the onset of a respiratory virus, which could escalate to more severe complications without immune protection. Distinguishing between the two requires context—timing relative to vaccination, exposure history, and symptom duration—yet both groups share the experience of discomfort, underscoring the body’s universal response to immune challenges.
From a practical standpoint, managing these symptoms follows similar protocols regardless of vaccination status. Over-the-counter medications like acetaminophen (500-1000 mg every 4-6 hours) or ibuprofen (200-400 mg every 6 hours) can alleviate fever and pain, though vaccinated individuals should avoid preemptive dosing to ensure optimal immune response. Hydration and rest remain cornerstone remedies, while monitoring symptoms for severity (e.g., persistent high fever, difficulty breathing) is critical for both groups. For vaccinated individuals, symptoms persisting beyond 3-5 days warrant medical consultation to rule out unrelated conditions. Unvaccinated individuals, however, should seek testing for infectious diseases if symptoms align with local outbreak patterns.
The overlap in symptoms highlights a paradox: vaccination aims to prevent disease, yet its side effects mimic the very illnesses it guards against. This duality can foster skepticism among the unvaccinated, who may misinterpret vaccine reactions as evidence of harm rather than immune priming. Conversely, vaccinated individuals might mistakenly attribute new symptoms to vaccine side effects, delaying diagnosis of an unrelated illness. Addressing this requires clear communication—emphasizing that transient reactions post-vaccine are normal, while persistent or worsening symptoms demand investigation. Both groups benefit from understanding that immune activation, whether from vaccination or infection, manifests similarly, reflecting the body’s shared defense mechanisms.
Ultimately, the convergence of vaccine side effects and natural symptoms serves as a reminder of the body’s intricate immune response. Vaccinated individuals trade the risk of severe disease for temporary discomfort, while the unvaccinated face the full spectrum of infection risks. Recognizing this common ground fosters empathy and informed decision-making, shifting the narrative from division to shared human experience. Whether vaccinated or not, the body’s reaction to immune triggers—be it a vaccine or a virus—is a testament to its resilience, demanding vigilance, care, and clarity in interpretation.
Vaccinated and Battling Omicron: Understanding the Duration of Symptoms
You may want to see also
Explore related products






![]()
Both groups contribute to ongoing public health surveillance and data collection efforts
Public health surveillance relies on data from both vaccinated and unvaccinated individuals to monitor disease trends, vaccine effectiveness, and potential side effects. Vaccinated individuals provide critical insights into how well vaccines perform in real-world settings, while unvaccinated individuals help identify disease circulation and emerging variants. This dual data stream allows health authorities to make informed decisions about vaccination strategies, outbreak responses, and resource allocation. For instance, during the COVID-19 pandemic, tracking breakthrough infections in vaccinated individuals alongside infection rates in unvaccinated populations helped assess vaccine efficacy and the need for booster doses.
To contribute effectively, individuals in both groups should report symptoms, test results, and vaccination status accurately. Vaccinated individuals should document their vaccine type, dosage dates, and any adverse reactions using tools like v-safe or local health department portals. Unvaccinated individuals should report illnesses promptly, especially if they test positive for vaccine-preventable diseases. For example, a 30-year-old unvaccinated individual with measles symptoms must notify their healthcare provider immediately to prevent community spread. Accurate reporting ensures that surveillance systems capture a complete picture of disease dynamics.
A comparative analysis reveals that both groups play distinct but complementary roles in data collection. Vaccinated individuals often participate in longitudinal studies tracking antibody levels or long-term immunity, such as those monitoring COVID-19 vaccine efficacy six months post-second dose. Unvaccinated individuals, particularly in controlled studies, help establish baseline disease rates and natural immunity patterns. For instance, a study comparing flu infection rates between vaccinated and unvaccinated groups aged 65+ highlighted the vaccine’s 40-60% effectiveness in preventing severe illness. Such comparisons are essential for refining vaccine formulations and public health messaging.
Practical tips for participation include staying informed about local surveillance programs and using digital health apps to log symptoms or vaccine responses. Parents of unvaccinated children under 5, for example, should enroll in pediatric disease monitoring programs to track illnesses like whooping cough or rotavirus. Vaccinated individuals can join booster trial cohorts to evaluate new formulations, such as the bivalent COVID-19 boosters targeting Omicron variants. By actively engaging in these efforts, both groups ensure that public health strategies remain evidence-based and responsive to evolving challenges.
Ultimately, the collective data from vaccinated and unvaccinated individuals strengthens global health systems. It enables rapid detection of vaccine-resistant strains, informs policy adjustments, and fosters trust in immunization programs. For example, surveillance data from both groups during the 2009 H1N1 pandemic guided vaccine distribution and prioritization for high-risk populations. This collaborative approach underscores the shared responsibility of all individuals in safeguarding public health, regardless of their vaccination status.
Vaccinations: Essential for Entry into China
You may want to see also
Frequently asked questions
Both vaccinated and unvaccinated individuals can still contract COVID-19, though vaccinated individuals generally experience milder symptoms and are less likely to be hospitalized or die from the virus.
Both groups can develop natural immunity after exposure to the virus, though vaccinated individuals gain immunity through the vaccine, which is safer and more predictable than infection.
Both groups can contribute to the spread of the virus, especially in the absence of preventive measures like masking and social distancing, though vaccinated individuals are less likely to transmit the virus.