The lack of vaccination has led to the resurgence and outbreak of several preventable diseases worldwide, posing significant public health challenges. Diseases such as measles, mumps, whooping cough (pertussis), and diphtheria, once largely controlled through widespread immunization, are now re-emerging in communities with low vaccination rates. For instance, measles outbreaks have spiked in regions where vaccine hesitancy or inaccessibility has reduced herd immunity, leading to severe complications and fatalities, particularly among children. Similarly, the decline in HPV vaccination has contributed to rising cases of cervical cancer and other HPV-related illnesses. The COVID-19 pandemic has further exacerbated this issue, as disruptions to routine immunization services and increased misinformation have left millions vulnerable to vaccine-preventable diseases, underscoring the critical importance of global vaccination efforts to curb these outbreaks.
| Characteristics | Values |
|---|---|
| Diseases Outbreaking | Measles, Pertussis (Whooping Cough), Mumps, Polio, Diphtheria, Tetanus |
| Primary Cause | Lack of vaccination (low vaccination rates, vaccine hesitancy) |
| Geographic Impact | Global, with hotspots in regions with low vaccine coverage |
| Populations Affected | Unvaccinated children, immunocompromised individuals, under-vaccinated communities |
| Recent Outbreaks | Measles outbreaks in Europe, Africa, and the U.S. (2022-2023) |
| Mortality Rates | Measles: ~0.2-5% fatality rate, depending on region and healthcare access |
| Preventability | All outbreaks are preventable through routine vaccination |
| Vaccine Availability | Widely available (e.g., MMR, DTaP, IPV vaccines) |
| Contributing Factors | Misinformation, lack of access to healthcare, political instability |
| Global Health Impact | Reversal of progress toward disease eradication (e.g., polio resurgence) |
Explore related products






What You'll Learn
- Measles resurgence in developed nations due to declining vaccination rates and misinformation
- Pertussis outbreaks increasing among infants and children with incomplete vaccine coverage
- Mumps cases rising in young adults despite availability of effective vaccines
- Polio reemergence in regions with low vaccination rates and poor healthcare access
- Diphtheria outbreaks in unvaccinated populations, leading to severe respiratory complications
![]()
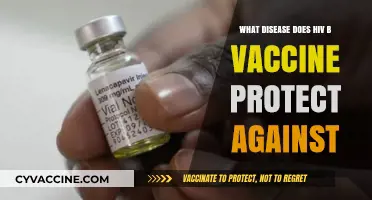
Measles resurgence in developed nations due to declining vaccination rates and misinformation
Measles, once on the brink of eradication in many developed nations, is making a dangerous comeback. This resurgence is directly linked to declining vaccination rates, fueled by the spread of misinformation and a growing distrust of vaccines. The consequences are stark: outbreaks are occurring in countries with previously high vaccination coverage, putting vulnerable populations at risk and straining healthcare systems.
Consider the 2019 measles outbreak in the United States, the largest since 1992. Over 1,200 cases were reported across 31 states, with New York City bearing the brunt. The majority of those affected were unvaccinated, many due to non-medical exemptions fueled by misinformation about vaccine safety. This outbreak highlighted the fragility of herd immunity, which requires at least 95% vaccination coverage to protect those who cannot be vaccinated due to medical reasons, such as infants under 12 months old or immunocompromised individuals. When vaccination rates drop below this threshold, even a single case can spark a widespread outbreak.
The role of misinformation cannot be overstated. False claims linking the measles, mumps, and rubella (MMR) vaccine to autism, despite being thoroughly debunked, continue to circulate on social media and other platforms. This misinformation preys on parental anxieties, leading some to delay or refuse vaccination for their children. For instance, a 2020 study found that exposure to anti-vaccine content on social media significantly decreased parents’ intentions to vaccinate their children. Combating this requires not only scientific evidence but also effective communication strategies that address concerns empathetically and build trust in healthcare institutions.
To reverse this trend, a multi-pronged approach is essential. First, healthcare providers must prioritize vaccine education during well-child visits, emphasizing the safety and efficacy of the MMR vaccine, which is typically administered in two doses: the first at 12-15 months and the second at 4-6 years. Second, policymakers should strengthen school immunization requirements, limiting non-medical exemptions to protect public health. Finally, social media platforms must take responsibility for curbing the spread of misinformation by promoting credible sources and flagging or removing false content.
The resurgence of measles is a stark reminder of the critical role vaccines play in preventing disease. By addressing the root causes of declining vaccination rates—misinformation, complacency, and access barriers—we can rebuild herd immunity and protect future generations from this entirely preventable disease. The choice is clear: act now to safeguard public health or risk a return to a pre-vaccine era where measles was a common and often deadly threat.
Switzerland's Vaccination Rules for Visitors Explained
You may want to see also
Explore related products






![]()
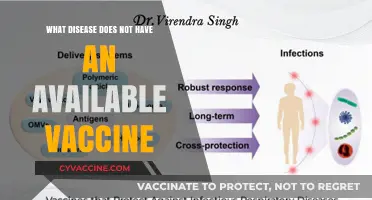
Pertussis outbreaks increasing among infants and children with incomplete vaccine coverage
Pertussis, commonly known as whooping cough, is resurging in communities with low vaccination rates, particularly among infants and young children. This highly contagious bacterial infection causes severe coughing fits, which can lead to breathing difficulties, vomiting, and exhaustion. For infants under 12 months, the disease is especially dangerous, often requiring hospitalization and sometimes resulting in death. The resurgence is directly linked to gaps in vaccine coverage, as the DTaP (Diphtheria, Tetanus, and Pertussis) vaccine series, typically administered at 2, 4, 6, and 15-18 months, followed by a booster at 4-6 years, is less effective when not completed on schedule.
The incomplete vaccine coverage among children creates pockets of vulnerability, allowing pertussis to spread rapidly. Parents may delay or skip doses due to misinformation, access barriers, or complacency, unaware that even a single missed dose significantly increases risk. For instance, a child who receives only the first two of the five recommended doses is 18 times more likely to contract pertussis than a fully vaccinated peer. This highlights the critical importance of adhering to the CDC’s immunization schedule, which is designed to build robust immunity during early childhood when the risk of severe complications is highest.
Comparing regions with high versus low vaccination rates reveals a stark contrast in outbreak frequency. In areas where DTaP coverage exceeds 90%, pertussis cases remain rare and manageable. Conversely, communities with coverage below 70% often experience recurring outbreaks, straining healthcare systems and endangering vulnerable populations. For example, a 2022 study found that counties with lower vaccination rates reported pertussis incidence rates three times higher than national averages. This data underscores the role of herd immunity in protecting infants too young to be fully vaccinated.
Practical steps can mitigate the risk of pertussis outbreaks. Parents should ensure their children receive all DTaP doses on time, with special attention to the 6-month and 15-month doses, which are crucial for building sustained immunity. Pregnant individuals should receive the Tdap vaccine between 27 and 36 weeks of gestation, as maternal antibodies provide passive protection to newborns during their first two months of life. Healthcare providers must also address vaccine hesitancy by educating families about the safety and efficacy of the DTaP vaccine, dispelling myths, and emphasizing the life-saving benefits of timely immunization.
In conclusion, the rise in pertussis cases among infants and children is a preventable crisis fueled by incomplete vaccine coverage. By adhering to recommended schedules, promoting maternal vaccination, and fostering informed decision-making, communities can reverse this trend and protect their youngest members from a highly preventable disease. The stakes are clear: vaccination is not just a personal choice but a collective responsibility to safeguard public health.
Vaccination vs. Passive/Active Immunity: Understanding the Key Differences
You may want to see also
Explore related products






![]()
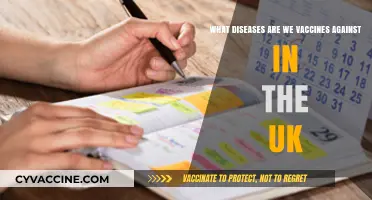
Mumps cases rising in young adults despite availability of effective vaccines
Mumps, a contagious viral infection characterized by swollen salivary glands, was once a common childhood illness. However, widespread vaccination through the Measles, Mumps, and Rubella (MMR) vaccine has drastically reduced its prevalence. Despite this, recent years have seen a concerning rise in mumps cases among young adults, a demographic that should have been protected by routine childhood immunizations. This trend raises questions about vaccine efficacy, waning immunity, and the impact of vaccination gaps.
The Resurgence: A Closer Look
Data from the Centers for Disease Control and Prevention (CDC) reveal that mumps outbreaks are increasingly occurring in colleges, universities, and other close-contact settings. Young adults aged 18–24 are particularly vulnerable, often due to incomplete vaccination histories or missed booster doses. The MMR vaccine, typically administered in two doses (the first at 12–15 months and the second at 4–6 years), provides approximately 88% effectiveness against mumps. However, immunity can wane over time, leaving individuals susceptible to infection, especially in crowded environments where the virus spreads easily through respiratory droplets.
Several factors contribute to this resurgence. First, vaccine hesitancy and misinformation have led to pockets of under-vaccinated populations, creating opportunities for the virus to circulate. Second, while the MMR vaccine is highly effective, it is not 100% protective, and outbreaks can still occur in fully vaccinated communities, particularly when immunity wanes. Third, international travel and migration can introduce the virus into regions where it had been largely eradicated. For young adults, the risk is compounded by lifestyle factors—shared living spaces, close social interactions, and lower awareness of vaccine status compared to childhood immunization records.
Practical Steps to Mitigate Risk
To combat this trend, young adults should verify their vaccination status with healthcare providers. Those who received only one dose of the MMR vaccine or are unsure of their history should get a second dose, as this significantly boosts immunity. During outbreaks, public health officials may recommend a third dose for high-risk groups. Additionally, practicing good hygiene—such as frequent handwashing, avoiding close contact with sick individuals, and covering coughs and sneezes—can reduce transmission. Institutions like colleges should implement vaccination verification policies and educate students about the importance of staying up-to-date on immunizations.
The Bigger Picture
The rise in mumps cases among young adults serves as a reminder that vaccine-preventable diseases do not discriminate by age. While the MMR vaccine remains a cornerstone of public health, its success depends on widespread adherence and ongoing research into immunity duration. Addressing this issue requires a multifaceted approach: improving vaccine access, combating misinformation, and fostering a culture of lifelong immunization. By taking proactive steps, individuals and communities can halt the resurgence of mumps and protect against other preventable diseases.
Religious Exemptions: Why Some Refuse Vaccines
You may want to see also
Explore related products






![]()
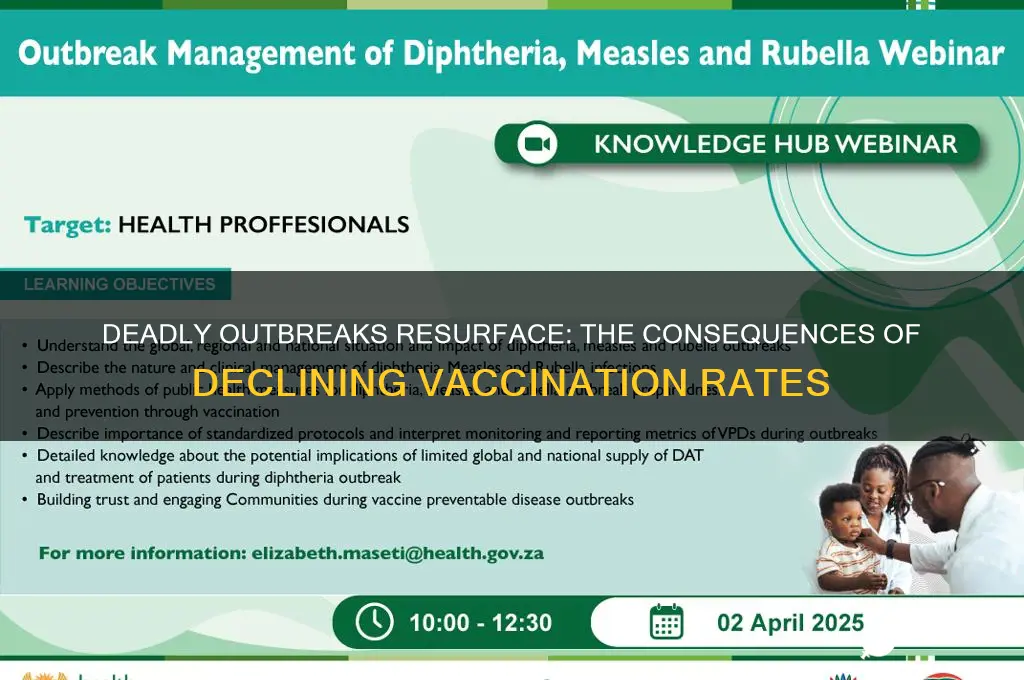
Polio reemergence in regions with low vaccination rates and poor healthcare access
Polio, a disease once on the brink of eradication, is staging a comeback in regions where vaccination rates have plummeted and healthcare systems are strained. This reemergence is not a coincidence but a direct consequence of disrupted immunization programs and limited access to medical resources. Countries like Pakistan, Afghanistan, and parts of Africa are witnessing a resurgence of this highly infectious disease, which can cause irreversible paralysis, particularly in children under five. The oral polio vaccine (OPV), requiring multiple doses to confer immunity, is often inaccessible in these areas due to logistical challenges, conflict, or misinformation, leaving vulnerable populations at risk.
Consider the mechanics of polio transmission and prevention. The virus spreads primarily through fecal-oral contact, thriving in areas with poor sanitation. The inactivated polio vaccine (IPV) and OPV are both effective, but OPV, administered orally, is more practical in low-resource settings. However, it requires a series of doses—typically four—to ensure full protection. When vaccination coverage drops below 80%, herd immunity collapses, allowing the virus to circulate freely. In regions where healthcare access is limited, even detecting outbreaks becomes a challenge, delaying response efforts and allowing the disease to spread unchecked.
The reemergence of polio is not just a health crisis but a stark reminder of the fragility of global eradication efforts. Compare this to measles, another vaccine-preventable disease, which has also seen outbreaks in under-vaccinated communities. Unlike measles, polio’s symptoms often go unnoticed in its early stages, making it harder to control. While measles outbreaks can be swiftly addressed with catch-up vaccination campaigns, polio requires sustained, multi-dose efforts. This makes it particularly devastating in regions where healthcare infrastructure is weak, and vaccination teams face threats from conflict or misinformation.
To combat polio’s resurgence, a multi-pronged approach is essential. First, strengthen routine immunization programs, ensuring that children receive all four doses of OPV by age five. Second, address misinformation through community engagement, involving local leaders to build trust in vaccines. Third, improve surveillance systems to detect cases early, even in remote areas. Practical tips include using mobile clinics to reach underserved populations and integrating polio vaccination with other health services, such as vitamin A supplementation, to maximize impact. Without these measures, polio will continue to exploit gaps in immunity, undoing decades of progress toward eradication.
Is Sputnik Vaccine Accessible in the United States? Key Facts
You may want to see also
Explore related products






![]()
Diphtheria outbreaks in unvaccinated populations, leading to severe respiratory complications
Diphtheria, a once-common childhood disease, has reemerged in unvaccinated populations, sparking outbreaks that highlight the critical role of vaccination in disease prevention. This bacterial infection, caused by *Corynebacterium diphtheriae*, primarily targets the respiratory system, leading to severe complications that can be life-threatening. The resurgence of diphtheria serves as a stark reminder of the consequences of vaccine hesitancy and the importance of maintaining high immunization rates to achieve herd immunity.
Understanding the Outbreak Dynamics
Diphtheria outbreaks in unvaccinated communities often begin with a single case introduced by an infected individual, whether through travel or local transmission. The disease spreads rapidly in areas with low vaccination coverage, as the bacteria thrive in susceptible populations. Unvaccinated children under 5 and adults over 60 are particularly vulnerable, though anyone without immunity is at risk. For instance, recent outbreaks in countries like Indonesia, India, and parts of Europe have disproportionately affected unvaccinated groups, with infection rates soaring in regions where vaccine uptake has declined.
Severe Respiratory Complications: A Grim Reality
The hallmark of diphtheria is the formation of a thick, gray pseudomembrane in the throat or nose, which can obstruct airways and lead to severe respiratory distress. Left untreated, this can progress to life-threatening complications such as myocarditis (heart muscle inflammation), neuritis (nerve damage), and respiratory failure. The toxin produced by *C. diphtheriae* is particularly insidious, causing systemic damage even in otherwise healthy individuals. In unvaccinated populations, hospitalization rates for diphtheria-related complications are significantly higher, with mortality rates reaching up to 10% in severe cases.
Prevention Through Vaccination: A Clear Solution
The diphtheria vaccine, typically administered as part of the DTaP (diphtheria, tetanus, and pertussis) or Tdap series, is highly effective in preventing infection. The CDC recommends a series of five doses for children, starting at 2 months of age, followed by a booster shot every 10 years for adults. In outbreak settings, catch-up vaccination campaigns are crucial to curb transmission. For example, during a 2017 outbreak in Yemen, rapid vaccination efforts targeting at-risk populations helped contain the spread, underscoring the vaccine’s role as a first line of defense.
Practical Steps for Protection
To prevent diphtheria outbreaks, individuals must ensure they and their families are up to date on vaccinations. Parents should adhere to the recommended immunization schedule for children, while adults should verify their booster status, especially before traveling to regions with known outbreaks. Healthcare providers play a vital role in educating communities about the risks of vaccine-preventable diseases and addressing misinformation. In outbreak scenarios, public health officials should prioritize contact tracing, antibiotic treatment for infected individuals, and widespread vaccination to halt the disease’s spread.
The Takeaway: Vaccination Saves Lives
Diphtheria outbreaks in unvaccinated populations are entirely preventable yet continue to cause severe respiratory complications and fatalities. The resurgence of this disease underscores the fragility of herd immunity and the need for sustained vaccination efforts. By prioritizing immunization, individuals not only protect themselves but also contribute to the collective health of their communities. In the fight against diphtheria, the message is clear: vaccination is not just a personal choice—it’s a public health imperative.
Hep B Vaccine: Who Should Avoid It?
You may want to see also
Frequently asked questions
Measles is a highly contagious viral disease that causes fever, rash, and can lead to severe complications like pneumonia and encephalitis. Outbreaks occur when vaccination rates drop below the herd immunity threshold (around 95%), allowing the virus to spread rapidly among unvaccinated individuals.
Pertussis is a bacterial infection causing severe coughing fits. It outbreaks due to waning immunity in vaccinated individuals and low vaccination coverage, leaving infants too young to be vaccinated and immunocompromised people at high risk.
Mumps is a viral infection causing swollen glands, fever, and potential complications like meningitis. Outbreaks occur when vaccination rates decline, as the mumps virus spreads easily in close-contact settings like schools and colleges.
Polio is a crippling and potentially fatal disease caused by the poliovirus. Despite near-eradication, it resurfaces in regions with low vaccination rates due to vaccine hesitancy, misinformation, and inadequate healthcare access, posing a risk of global re-emergence.