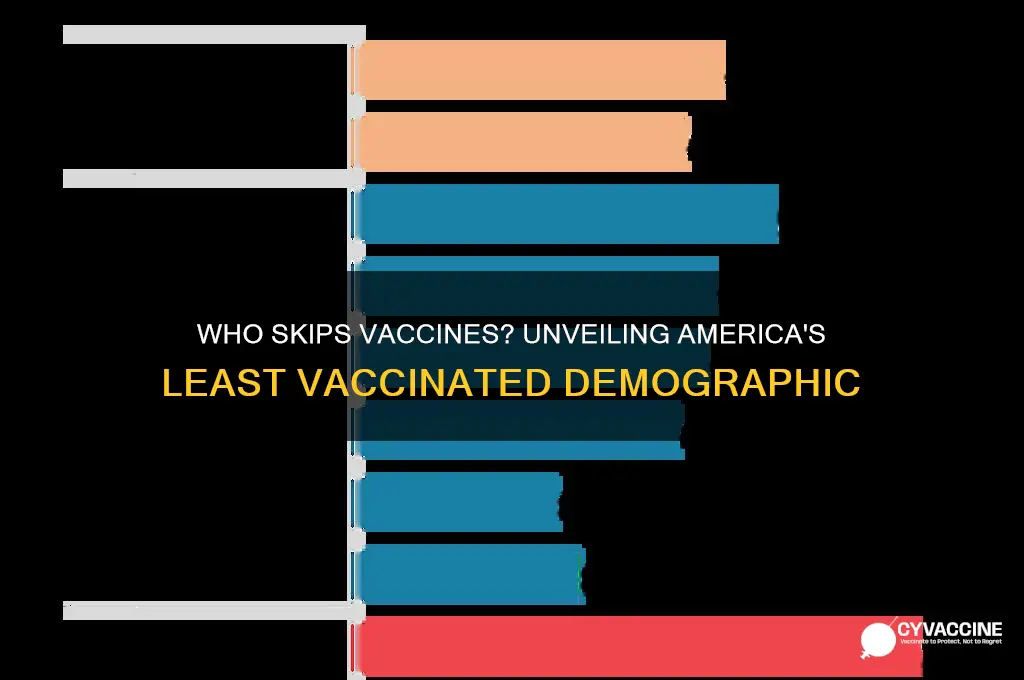
The question of which demographic in America is less likely to vaccinate is a complex and multifaceted issue, influenced by a variety of socioeconomic, cultural, and geographic factors. Research indicates that certain groups, such as younger adults, individuals with lower levels of education, and those living in rural or conservative-leaning areas, tend to exhibit higher vaccine hesitancy. Additionally, communities of color, particularly Black and Hispanic populations, have historically shown lower vaccination rates, often due to systemic barriers, mistrust in healthcare institutions, and disparities in access to information and resources. Understanding these disparities is crucial for developing targeted public health strategies to address vaccine hesitancy and ensure equitable health outcomes across all demographics.
| Characteristics | Values |
|---|---|
| Political Affiliation | Republicans (45% unvaccinated as of Dec 2021) |
| Region | Southern states (e.g., Mississippi, Alabama, Louisiana) |
| Education Level | Lower education attainment (high school or less) |
| Age Group | Younger adults (18-29 years old) |
| Race/Ethnicity | White Americans (though disparities exist across all groups) |
| Rural vs. Urban | Rural residents |
| Income Level | Lower-income households |
| Health Insurance Status | Uninsured individuals |
| Parental Status | Parents hesitant to vaccinate children |
| Religious Beliefs | Some religious groups with exemptions |
| Historical Medical Mistrust | Communities with historical mistrust of medical institutions (e.g., African American communities due to Tuskegee Syphilis Study) |
| Information Sources | Reliance on social media or non-scientific sources for health information |
Explore related products






What You'll Learn
- Educational Attainment: Lower vaccination rates among those with less formal education
- Political Affiliation: Conservatives and libertarians often report higher vaccine hesitancy
- Rural Residents: Limited access and misinformation contribute to lower rural vaccination rates
- Young Adults: Skepticism and perceived low risk reduce vaccination in younger demographics
- Religious Beliefs: Some religious groups oppose vaccines due to moral or faith-based concerns
![]()
Educational Attainment: Lower vaccination rates among those with less formal education
A stark disparity emerges when examining vaccination rates through the lens of educational attainment. Individuals with lower levels of formal education consistently exhibit lower vaccination rates across various demographics. This trend is not merely a coincidence but a complex interplay of socioeconomic factors, access to information, and systemic barriers.
Consider the following scenario: a community health worker organizes a vaccination drive in a low-income neighborhood. Despite the availability of free vaccines, turnout is disappointingly low. Upon closer inspection, it becomes evident that many residents lack access to reliable information about vaccine safety and efficacy. Misinformation spreads through word-of-mouth, fueled by mistrust of institutions and a lack of health literacy. This example illustrates how limited educational opportunities can perpetuate vaccine hesitancy, creating a cycle of vulnerability to preventable diseases.
To address this issue, targeted interventions must prioritize health education and community engagement. For instance, implementing vaccine education programs in schools and community centers can empower individuals with the knowledge to make informed decisions. These programs should be culturally sensitive, addressing specific concerns and misconceptions prevalent in underserved communities. Additionally, leveraging trusted community leaders, such as religious figures or local healthcare providers, can help bridge the gap between public health initiatives and hesitant populations.
A comparative analysis reveals that regions with higher educational attainment often have robust public health infrastructure, facilitating easier access to vaccines and accurate information. In contrast, areas with lower educational levels frequently face challenges like limited healthcare facilities, transportation barriers, and language obstacles. Policymakers must allocate resources to improve healthcare accessibility in these regions, ensuring that vaccination services are not only available but also culturally and logistically accessible.
In conclusion, the correlation between educational attainment and vaccination rates underscores the need for multifaceted strategies. By combining education, community engagement, and systemic improvements, we can work toward reducing disparities and protecting public health. Practical steps include offering multilingual vaccine information, providing transportation assistance to vaccination sites, and integrating health literacy into adult education programs. Addressing this issue requires a commitment to equity, ensuring that all individuals, regardless of educational background, have the opportunity to safeguard their health through vaccination.
Vaccines and Autism: Debunking Myths and Understanding the Science
You may want to see also
Explore related products






![]()
Political Affiliation: Conservatives and libertarians often report higher vaccine hesitancy
Political affiliation plays a significant role in vaccine hesitancy, with conservatives and libertarians consistently reporting higher levels of skepticism compared to their liberal counterparts. This trend is not merely anecdotal; it is supported by numerous studies and surveys. For instance, a 2021 Pew Research Center poll found that 45% of Republicans and Republican-leaning independents said they would probably or definitely not get a COVID-19 vaccine, compared to just 6% of Democrats and Democratic-leaning independents. This stark divide underscores the influence of political ideology on health decisions.
To understand this phenomenon, consider the core values often associated with conservatism and libertarianism: individual liberty, skepticism of government intervention, and a preference for personal choice over collective mandates. These principles can clash with public health measures like vaccination campaigns, which inherently require widespread participation to achieve herd immunity. For example, libertarians may view vaccine mandates as an infringement on their freedom to make personal health decisions, even if those decisions pose risks to community health. This ideological stance often translates into practical behavior, such as refusing or delaying vaccinations for themselves and their children.
Addressing vaccine hesitancy among conservatives and libertarians requires a tailored approach that respects their values while emphasizing the benefits of vaccination. One effective strategy is to frame vaccination as an act of personal responsibility rather than a government directive. For instance, highlighting how getting vaccinated protects not only the individual but also vulnerable family members or community members can resonate with conservative values of family and community protection. Additionally, using trusted messengers, such as local doctors or religious leaders who share similar political leanings, can help bridge the credibility gap.
A comparative analysis reveals that while conservatives and libertarians are more likely to express vaccine hesitancy, their concerns are not monolithic. Some may worry about the speed of vaccine development, while others may distrust pharmaceutical companies or government health agencies. Understanding these specific concerns allows for more targeted interventions. For example, providing transparent information about vaccine safety trials or offering data on long-term efficacy can address fears about rushed development. Similarly, emphasizing the voluntary nature of vaccination (where mandates do not exist) can align with libertarian principles of choice.
In practical terms, public health campaigns aimed at this demographic should avoid confrontational or authoritarian tones, which can reinforce resistance. Instead, focus on shared goals, such as protecting loved ones or restoring normalcy to daily life. For parents hesitant to vaccinate their children, providing age-specific dosage information and explaining the rigorous testing vaccines undergo for different age groups can alleviate concerns. For example, the COVID-19 vaccine dosage for children aged 5–11 is one-third the size of the adult dose, reflecting careful consideration of safety and efficacy for younger age groups.
Ultimately, bridging the political divide in vaccine hesitancy requires empathy, clear communication, and a willingness to meet people where they are. By acknowledging the legitimate concerns of conservatives and libertarians while presenting vaccination as a tool for individual and collective well-being, public health efforts can make meaningful strides in increasing vaccine uptake across the political spectrum.
School Staff Vaccination: Mandatory or Optional? Exploring the Debate
You may want to see also
Explore related products






![]()
Rural Residents: Limited access and misinformation contribute to lower rural vaccination rates
Rural residents in America face unique challenges when it comes to vaccination, and these challenges are deeply intertwined with issues of access and information. Unlike their urban counterparts, who often live within a short drive of multiple healthcare facilities, rural Americans may need to travel significant distances—sometimes over an hour—to reach the nearest vaccination site. This logistical hurdle is compounded by limited public transportation options, making it difficult for those without personal vehicles to attend vaccination appointments. For instance, in states like Montana and Wyoming, where vast distances separate communities, the mere act of traveling to a clinic can deter individuals from seeking vaccines, particularly for multi-dose regimens such as the COVID-19 or HPV vaccines.
Misinformation also plays a critical role in shaping vaccination attitudes in rural areas. Studies have shown that rural populations are more likely to encounter and believe vaccine-related myths, often disseminated through social media or word-of-mouth networks. The lack of reliable, localized healthcare information exacerbates this issue. While urban residents can easily consult multiple healthcare providers or attend community health fairs, rural residents may rely on a single, overburdened clinic or pharmacist for medical advice. This scarcity of trusted sources leaves a void that misinformation can readily fill, leading to skepticism about vaccine safety and efficacy. For example, false claims about COVID-19 vaccines causing infertility or altering DNA have gained traction in rural communities, despite scientific evidence to the contrary.
Addressing these disparities requires tailored solutions that consider the unique needs of rural populations. One practical step is to bring vaccination services directly to these communities through mobile clinics or pop-up vaccination events. These initiatives can reduce travel burdens and increase convenience, particularly for older adults or families with young children. For instance, during the COVID-19 vaccine rollout, states like Iowa and Kentucky deployed mobile units to rural areas, successfully administering thousands of doses to those who might otherwise have been left behind. Additionally, partnering with local trusted figures—such as farmers, teachers, or religious leaders—to disseminate accurate vaccine information can help counteract misinformation and build confidence in immunization programs.
Another critical strategy is to leverage technology to bridge the information gap. Telehealth services, for example, can connect rural residents with healthcare providers who can address concerns and provide personalized advice about vaccines. Social media campaigns tailored to rural audiences, using relatable language and local success stories, can also help dispel myths and encourage vaccination. For instance, a campaign highlighting how a flu vaccine prevented severe illness in a well-known community member could resonate more strongly than generic public health messaging. By combining accessibility with targeted communication, these efforts can begin to close the vaccination gap in rural America.
Ultimately, the lower vaccination rates among rural residents are not solely a matter of personal choice but a reflection of systemic barriers that require proactive intervention. Policymakers, healthcare providers, and community leaders must collaborate to ensure that rural Americans have the same opportunities to protect their health as their urban peers. This includes investing in infrastructure to improve access, fostering partnerships to combat misinformation, and designing programs that respect the unique cultural and logistical realities of rural life. Without such concerted efforts, the vaccination divide will persist, leaving rural communities disproportionately vulnerable to preventable diseases.
Post-Vaccine Arm Exercises: Safe or Risky? Expert Advice Revealed
You may want to see also
Explore related products






![]()
Young Adults: Skepticism and perceived low risk reduce vaccination in younger demographics
Young adults, particularly those aged 18 to 29, are among the least likely demographics in America to receive vaccinations, including those for COVID-19, influenza, and other preventable diseases. This trend is driven by a combination of skepticism toward vaccine efficacy and safety, coupled with a perceived low personal risk of severe illness. Surveys show that nearly 30% of unvaccinated individuals in this age group cite concerns about side effects or long-term health impacts, while another 25% believe they are healthy enough to fend off infections without vaccines. This mindset, however, overlooks the broader public health implications of low vaccination rates, such as prolonged community transmission and the emergence of new variants.
To address skepticism, public health campaigns must focus on transparent communication about vaccine development, testing, and side effects. For instance, explaining that mRNA vaccines, like those for COVID-19, do not alter DNA and have been rigorously tested in trials involving tens of thousands of participants can alleviate unfounded fears. Additionally, emphasizing that common side effects, such as soreness or fatigue, are signs the immune system is responding appropriately—not indicators of harm—can reframe these experiences positively. Young adults are more likely to trust information from peers or social media influencers, so leveraging these channels with accurate, relatable messaging could be effective.
The perception of low risk among young adults is another critical barrier. While it’s true that younger individuals are less likely to experience severe illness from diseases like COVID-19 or influenza, they are not immune to complications. For example, up to 20% of young adults hospitalized with COVID-19 require intensive care, and long COVID symptoms, such as fatigue and brain fog, can persist for months. Similarly, influenza can lead to pneumonia or worsen underlying conditions like asthma. Highlighting these risks in a way that resonates with this demographic—such as emphasizing the impact on academic performance, career goals, or social life—can shift their perspective.
Practical steps can also encourage vaccination among young adults. Making vaccines easily accessible through on-campus clinics, workplaces, or pop-up sites at popular venues removes logistical barriers. Offering incentives, such as discounts, gift cards, or entries into prize drawings, has proven effective in boosting participation. For example, during the COVID-19 vaccine rollout, states like Ohio saw a 28% increase in vaccinations among 18- to 29-year-olds after introducing a lottery program. Pairing these strategies with clear, concise information about the benefits of vaccination can help bridge the gap between skepticism and action.
Ultimately, addressing vaccine hesitancy in young adults requires a multi-faceted approach that acknowledges their concerns while providing actionable, evidence-based solutions. By combining education, accessibility, and incentives, public health efforts can empower this demographic to make informed decisions that protect not only themselves but also their communities. The goal is not to dismiss their skepticism but to engage it constructively, fostering trust and promoting a culture of prevention.
Vaccine Safety: Age-Related Risks and Realities
You may want to see also
Explore related products




![]()
Religious Beliefs: Some religious groups oppose vaccines due to moral or faith-based concerns
Religious beliefs have historically influenced health decisions, and vaccination is no exception. Certain faith-based communities in America exhibit lower vaccination rates due to moral or theological concerns tied to vaccine development, ingredients, or perceived interference with divine will. For instance, some Christian Scientists, adhering to their reliance on spiritual healing, may avoid medical interventions like vaccines altogether. Similarly, specific interpretations of Islamic teachings have led to skepticism about vaccines containing porcine-derived gelatin, though many Islamic scholars now endorse alternatives or deem them permissible under necessity. These examples underscore how deeply held religious convictions can shape public health behaviors.
Analyzing the root of this opposition reveals a complex interplay between faith and science. Many religious groups express concerns about vaccines derived from cell lines originating in the 1960s from aborted fetal tissue, such as those used in rubella and chickenpox vaccines. For instance, some Catholic and evangelical communities have raised ethical objections, though the Vatican and many Protestant leaders have clarified that receiving such vaccines is morally acceptable when alternatives are unavailable. This tension highlights the challenge of reconciling modern medical practices with religious doctrines that prioritize sanctity of life from conception.
Persuading these communities to vaccinate requires culturally sensitive approaches. Public health campaigns must engage religious leaders as trusted messengers to bridge the gap between faith and science. For example, during the COVID-19 pandemic, partnerships with imams, pastors, and rabbis helped disseminate accurate vaccine information and address misconceptions within their congregations. Practical steps include hosting vaccine clinics at places of worship, providing educational materials aligned with religious values, and offering vaccines free of contentious ingredients where possible. Such strategies demonstrate respect for religious beliefs while promoting community health.
Comparatively, historical precedents offer lessons for addressing vaccine hesitancy in religious groups. The 1990s measles outbreak among Amish communities in Pennsylvania was mitigated through collaboration with local bishops, who endorsed vaccination after understanding its benefits. Similarly, in Orthodox Jewish communities, rabbis have issued *psak halacha* (religious rulings) permitting vaccines, even during holidays, when medical necessity arises. These successes illustrate that when public health initiatives align with religious authority and cultural norms, compliance improves significantly.
In conclusion, addressing vaccine hesitancy rooted in religious beliefs demands empathy, education, and collaboration. By acknowledging faith-based concerns, engaging trusted leaders, and offering tailored solutions, public health efforts can foster trust and increase vaccination rates in these communities. The goal is not to challenge religious convictions but to demonstrate how vaccination aligns with shared values of protecting life and community well-being. This approach not only safeguards individual health but also strengthens societal resilience against preventable diseases.
When Should You Get the Pneumonia Vaccine? Age Guidelines Explained
You may want to see also
Frequently asked questions
Younger adults, particularly those aged 18-29, are often less likely to vaccinate compared to older age groups, due to factors like lower perceived risk and vaccine hesitancy.
Black and Hispanic communities in the U.S. have historically reported lower vaccination rates, often influenced by systemic barriers, mistrust in healthcare systems, and limited access to vaccines.
Individuals identifying with conservative or Republican political views are generally less likely to vaccinate, influenced by political polarization, misinformation, and skepticism toward public health mandates.