The selection of the correct combination of vaccine route and administration site is crucial for maximizing immunogenicity, safety, and efficacy. Different vaccines are designed to be administered via specific routes, such as intramuscular, subcutaneous, or intradermal, each targeting distinct immune responses. For instance, intramuscular injections, commonly used for vaccines like influenza or COVID-19 mRNA vaccines, deliver antigens into muscle tissue to elicit a robust systemic immune response. Subcutaneous injections, often used for vaccines like MMR or hepatitis B, deposit antigens into the fatty layer beneath the skin, stimulating both local and systemic immunity. Intradermal administration, utilized for vaccines like tuberculosis (BCG) or certain rabies vaccines, introduces antigens into the skin’s dermal layer, leveraging the skin’s dense immune cell population for enhanced immune activation. The choice of site, such as the deltoid muscle, thigh, or upper arm, further influences vaccine uptake and side effects. Understanding these combinations ensures optimal vaccine performance and minimizes adverse reactions, making it a critical consideration in immunization strategies.
Explore related products






What You'll Learn
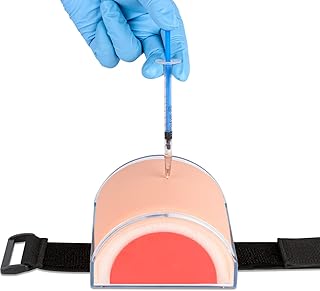
- Intramuscular (IM) Deltoid Muscle: Ideal for COVID-19, influenza vaccines, ensuring strong immune response
- Subcutaneous (SC) Upper Arm: Used for MMR, varicella, administered into fatty tissue
- Intradermal (ID) Forearm: For tuberculosis (TB) testing, injecting into skin layer
- Oral Route: Polio vaccine delivered via mouth for mucosal immunity
- Nasal Spray: Flu vaccine administered nasally for respiratory tract protection
![]()
Intramuscular (IM) Deltoid Muscle: Ideal for COVID-19, influenza vaccines, ensuring strong immune response
The deltoid muscle, located in the upper arm, is a prime target for intramuscular (IM) vaccine administration, particularly for COVID-19 and influenza vaccines. This site offers several advantages, including a robust immune response due to the muscle's rich vascular supply and the presence of numerous antigen-presenting cells. When a vaccine is injected into the deltoid, it is rapidly absorbed into the bloodstream, triggering a swift and effective immune reaction. For instance, the Pfizer-BioNTech and Moderna COVID-19 vaccines, both mRNA-based, are administered as 0.3 mL and 0.5 mL doses, respectively, directly into the deltoid muscle for individuals aged 12 and older. This precise delivery ensures optimal antigen exposure, leading to the production of high levels of neutralizing antibodies.
From an analytical perspective, the choice of the deltoid muscle for IM injections is not arbitrary. Its anatomical position minimizes the risk of injury to nerves and blood vessels, making it safer compared to other sites like the vastus lateralis (thigh) or gluteal muscles. Additionally, the deltoid’s accessibility simplifies the vaccination process, reducing the likelihood of administration errors. Studies have shown that IM deltoid injections produce a more consistent immune response across diverse populations, including the elderly, whose immune systems may be less responsive. For influenza vaccines, which are typically administered as a 0.5 mL dose, the deltoid site has been associated with fewer local adverse reactions, such as pain and swelling, compared to other routes.
Practically, administering vaccines via the IM deltoid route requires adherence to specific guidelines. The needle should be inserted at a 90-degree angle, with the skin stretched taut to ensure proper depth. For adults, a 1-inch needle is standard, while children and adolescents may require a 5/8-inch needle to avoid penetrating the bone. Healthcare providers must also ensure the patient’s arm is relaxed and positioned correctly to expose the deltoid muscle fully. A common mistake is injecting too high or too low, which can reduce vaccine efficacy or cause discomfort. Proper technique is especially critical for COVID-19 booster doses, where consistent delivery is essential to maintain immunity.
Comparatively, the IM deltoid route stands out when juxtaposed with subcutaneous (SC) or intradermal (ID) administration. While SC injections, often used for vaccines like MMR, deliver antigens into the fatty tissue beneath the skin, they generally elicit a slower immune response. ID injections, such as those used for tuberculosis testing, are limited by the small volume they can accommodate and are less practical for vaccines requiring larger doses. The deltoid’s IM route combines the benefits of rapid absorption and higher antigen load, making it ideal for vaccines like COVID-19 and influenza, which demand a strong and quick immune reaction.
In conclusion, the IM deltoid muscle is a cornerstone of effective vaccine delivery for COVID-19 and influenza, ensuring a potent immune response while minimizing risks. Its anatomical advantages, coupled with precise administration techniques, make it the preferred site for these critical vaccines. Healthcare providers should remain vigilant in their technique, ensuring proper needle placement and patient positioning to maximize efficacy. For the public, understanding the rationale behind this route can foster confidence in vaccination processes, reinforcing the importance of this simple yet powerful medical practice.
Vaccinate Your Child: Expert Advice from the National Network for Immunization
You may want to see also
Explore related products






![]()
Subcutaneous (SC) Upper Arm: Used for MMR, varicella, administered into fatty tissue
The subcutaneous (SC) route in the upper arm is a precise and effective method for administering vaccines like MMR (measles, mumps, rubella) and varicella (chickenpox). This approach targets the fatty tissue just beneath the skin, ensuring optimal immune response while minimizing discomfort. Unlike intramuscular injections, which penetrate deeper into muscle, SC injections deliver the vaccine into the subcutis, a layer rich in immune cells that facilitate antigen uptake.
For healthcare providers, the technique is straightforward yet requires attention to detail. The upper arm, specifically the fatty area between the deltoid muscle and the skin, is the recommended site. To administer, pinch a small fold of skin, insert the needle at a 45-degree angle, and inject the vaccine slowly. For MMR, the standard dose is 0.5 mL, while varicella requires 0.5 mL for children aged 12 months to 12 years and 1.0 mL for individuals 13 years and older. Always use a 5/8-inch (16 mm) needle to ensure proper delivery into the subcutaneous tissue.
Patients often prefer this route due to its relative comfort compared to intramuscular injections. However, mild side effects such as redness, swelling, or tenderness at the injection site are common and typically resolve within a few days. Applying a cool compress can alleviate discomfort, but avoid massaging the area, as this may disrupt vaccine absorption. It’s also crucial to rotate injection sites for individuals requiring multiple SC vaccinations to prevent tissue damage.
From a public health perspective, the SC upper arm route plays a vital role in vaccine distribution, particularly in pediatric populations. Its ease of administration and lower risk of adverse reactions make it ideal for mass immunization campaigns. For example, MMR and varicella vaccines are often given together, and the SC route ensures both are delivered effectively without overwhelming the injection site. This method aligns with global vaccination guidelines, emphasizing safety and efficacy in preventing infectious diseases.
In summary, the subcutaneous upper arm route is a cornerstone of vaccine administration for MMR and varicella, combining precision, patient comfort, and immune efficacy. By adhering to proper technique and dosage guidelines, healthcare providers can maximize the benefits of this method, contributing to broader public health goals. Whether in a clinic or community setting, mastering this approach ensures vaccines are delivered with both care and impact.
Vaccination Status: Can Teachers Ask?
You may want to see also
Explore related products






![]()
Intradermal (ID) Forearm: For tuberculosis (TB) testing, injecting into skin layer
The intradermal (ID) route, specifically targeting the forearm, is the gold standard for tuberculosis (TB) testing. This method involves injecting a small dose of purified protein derivative (PPD) into the dermal layer of the skin, typically using a 27-gauge needle at a 5-15 degree angle. The technique requires precision: too deep, and the antigen enters the subcutaneous tissue, potentially leading to false-negative results; too shallow, and it may not deposit correctly. The forearm is preferred due to its accessibility, thinner skin, and lower risk of interference from subcutaneous fat, ensuring accurate and reliable results.
From an analytical perspective, the ID forearm approach maximizes the immune response while minimizing discomfort. The dermal layer contains a high concentration of antigen-presenting cells, such as Langerhans cells, which efficiently capture and process the PPD. This triggers a localized delayed-type hypersensitivity reaction, measurable as induration 48–72 hours post-injection. Studies show that this method achieves a sensitivity of 80–90% in detecting TB infection, making it a critical tool in high-burden settings. However, its success hinges on proper technique, highlighting the need for trained personnel to administer the test.
For healthcare providers, mastering the ID forearm technique involves several key steps. First, clean the forearm site with alcohol and allow it to dry completely. Next, stretch the skin taut to stabilize the area and insert the needle with a quick, dart-like motion. Once the bevel is correctly positioned, inject 0.1 mL of PPD, forming a pale wheal under the skin. If the wheal is not visible, the injection may have been too deep, necessitating a repeat test. After removal, do not massage the site, as this can distort the reaction. Proper documentation of the injection technique and patient instructions are essential for accurate interpretation.
A comparative analysis reveals the ID forearm method’s advantages over alternatives. Subcutaneous injection, for instance, lacks the precision needed for TB testing, often leading to false results. Similarly, intramuscular routes are unsuitable due to the deeper tissue involvement. The ID approach, while more technically demanding, offers superior reliability and consistency. It is particularly valuable in pediatric populations, where the forearm’s thinner skin ensures better antigen delivery compared to other sites. However, it is not without limitations: individuals with dermatological conditions or those on immunosuppressive therapy may exhibit reduced reactions, requiring clinical correlation.
In practice, the ID forearm technique serves as a cornerstone of TB screening programs worldwide. Its specificity and ability to detect latent TB infection make it indispensable in both endemic and low-incidence regions. For travelers, immigrants, and healthcare workers, this method provides critical insights into infection status, guiding preventive therapy decisions. Practical tips include scheduling readings at exactly 72 hours to avoid underestimation and ensuring patients avoid covering the site with tight clothing. By adhering to these guidelines, clinicians can optimize the accuracy and utility of TB testing, ultimately contributing to global TB control efforts.
Vaccine Rules in Chicago: Proof Required?
You may want to see also
Explore related products






![]()
Oral Route: Polio vaccine delivered via mouth for mucosal immunity
The oral polio vaccine (OPV) stands as a testament to the power of mucosal immunity, a critical yet often overlooked aspect of our body's defense system. Unlike injections that target systemic immunity, OPV is administered via the mouth, directly engaging the mucosal surfaces of the gastrointestinal tract. This route mimics the natural pathway of poliovirus entry, stimulating the production of IgA antibodies in the gut, where the virus first encounters the immune system. This localized immune response not only prevents the virus from establishing infection but also reduces viral shedding, curbing community transmission.
Administering OPV is straightforward yet requires precision. The vaccine is delivered as drops, typically 0.1 mL for infants and children, directly into the mouth. For optimal absorption, it’s crucial to avoid feeding the child 30 minutes before and after vaccination, as food or drink can dilute the vaccine. The World Health Organization recommends a primary series of three doses, starting at 6 weeks of age, followed by booster doses to ensure long-term immunity. This regimen has been instrumental in the near-eradication of polio, particularly in regions with limited access to healthcare infrastructure, as OPV’s ease of administration and low cost make it ideal for mass immunization campaigns.
One of the most compelling advantages of the oral route is its ability to induce both mucosal and systemic immunity. While the primary goal is to protect the gut, OPV also triggers a systemic response, producing IgG antibodies in the bloodstream. This dual action ensures comprehensive protection against poliovirus, whether it enters the body through the mouth or other routes. However, this approach is not without challenges. Rare cases of vaccine-derived poliovirus (VDPV) have emerged, where the attenuated virus in OPV reverts to a virulent form in underimmunized populations. This risk underscores the importance of high vaccination coverage to maintain herd immunity.
Comparatively, the inactivated polio vaccine (IPV), administered via injection, offers systemic immunity but lacks the mucosal protection of OPV. This distinction highlights the strategic choice of vaccine route and site: OPV’s oral delivery is specifically tailored to combat a virus that thrives in the mucosal environment. In regions where polio remains endemic, OPV remains the vaccine of choice due to its ability to interrupt transmission. However, in polio-free countries, IPV is often preferred to eliminate the minimal risk of VDPV, illustrating how the correct combination of route and site depends on epidemiological context.
In practice, the success of OPV lies in its alignment with the biology of poliovirus and the practical realities of global health. Its oral administration eliminates the need for trained personnel to administer injections, making it accessible in remote areas. For parents and caregivers, ensuring the vaccine is administered correctly involves simple steps: confirm the child is healthy, avoid feeding around vaccination time, and follow the recommended schedule. This approach not only protects individuals but also contributes to the global effort to eradicate polio, proving that the right combination of vaccine route and site can transform public health outcomes.
Live Virus Vaccines: What's the Risk?
You may want to see also
Explore related products






![]()
Nasal Spray: Flu vaccine administered nasally for respiratory tract protection
The nasal spray flu vaccine, also known as the live attenuated influenza vaccine (LAIV), offers a needle-free alternative to traditional flu shots. Administered directly into the nostrils, it targets the respiratory tract—the primary entry point for influenza viruses. This route of delivery stimulates mucosal immunity, producing antibodies in the nose and throat to neutralize the virus before it can establish infection. Unlike injectable vaccines, which primarily induce systemic immunity, LAIV mimics the natural infection process, potentially offering better protection against respiratory transmission.
For optimal effectiveness, LAIV is typically administered as a single dose for individuals aged 2 to 49. Children aged 2 to 8 receiving the vaccine for the first time, however, require two doses spaced at least four weeks apart. The spray is delivered in a prefilled, single-use syringe with a nozzle designed for precise intranasal administration. Each dose contains live but weakened influenza viruses, which replicate in the cooler temperatures of the nasal passages but cannot survive in the warmer lung environment. This design ensures safety while triggering a robust immune response.
One of the key advantages of LAIV is its convenience, particularly for needle-averse individuals, such as young children. However, it is not suitable for everyone. Pregnant individuals, those with weakened immune systems, and people with certain chronic conditions, such as asthma or severe allergies, should avoid LAIV. Additionally, individuals with a history of severe egg allergy or those who have experienced Guillain-Barré syndrome within six weeks of a previous flu vaccine should opt for an alternative formulation.
Practical tips for administering LAIV include ensuring the recipient is in an upright position to facilitate proper delivery. If the individual sneezes immediately after administration, the dose does not need to be repeated, as sufficient vaccine is typically retained in the nasal passages. Side effects are generally mild and may include runny nose, wheezing, headache, or vomiting in children. These symptoms usually resolve within a few days and are far less disruptive than the potential complications of influenza.
In summary, the nasal spray flu vaccine provides a targeted approach to respiratory tract protection by leveraging the body’s mucosal immune system. Its ease of administration and needle-free format make it an attractive option for eligible individuals, particularly children. However, careful consideration of contraindications and adherence to dosing guidelines are essential to ensure safety and efficacy. For those who qualify, LAIV represents a valuable tool in the fight against seasonal influenza.
Antibiotics vs. Vaccines: Understanding Their Unique Roles in Medicine
You may want to see also
Frequently asked questions
The influenza vaccine is typically administered via the intramuscular (IM) route into the deltoid muscle of the upper arm for adults and older children, or the anterolateral thigh muscle for infants and young children.
The MMR vaccine is administered via the subcutaneous (SC) route, preferably into the fatty tissue over the deltoid muscle in the upper arm for adults and children.
The COVID-19 mRNA vaccine is given via the intramuscular (IM) route, typically into the deltoid muscle of the upper arm for individuals aged 12 and older.