Vaccines against viruses are a cornerstone of modern medicine, designed to stimulate the immune system to recognize and combat specific viral pathogens. Created through rigorous scientific processes, these vaccines often utilize weakened or inactivated forms of the virus, genetic material like mRNA, or viral proteins to trigger an immune response without causing the disease. Platforms like Course Hero provide valuable educational resources that explain the principles behind vaccine development, including how they are tailored to target viruses such as influenza, measles, or COVID-19. Understanding these mechanisms is crucial for appreciating the role of vaccines in preventing outbreaks, reducing disease severity, and saving lives globally.
Explore related products






What You'll Learn
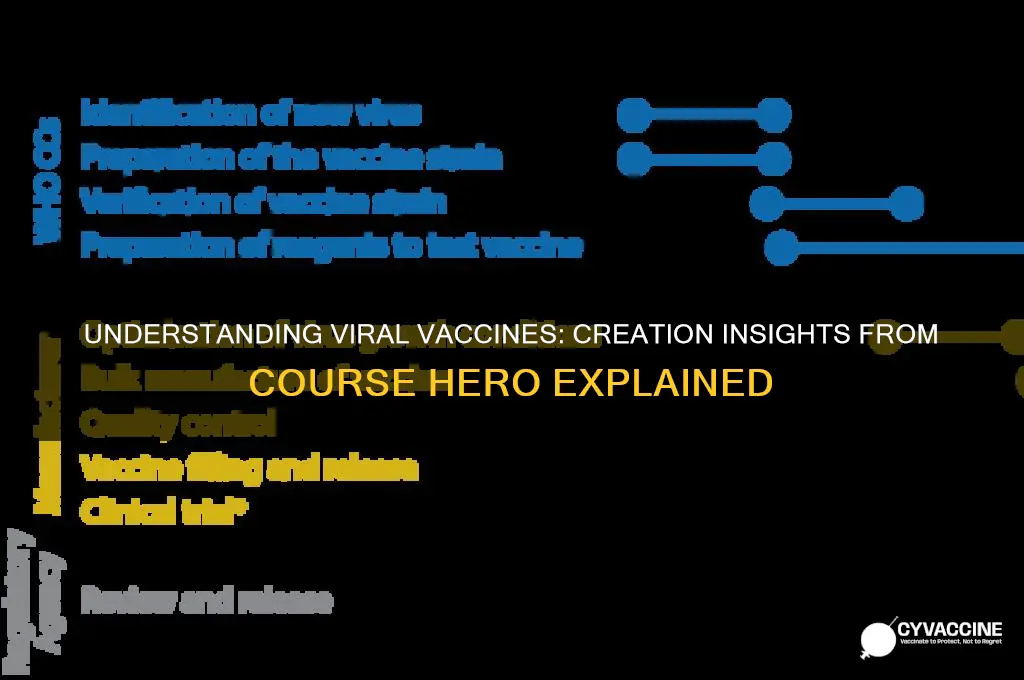
- Vaccine Development Process: Steps from virus identification to clinical trials and approval
- Types of Viral Vaccines: Live-attenuated, inactivated, mRNA, and viral vector vaccines explained
- Immune Response Mechanisms: How vaccines trigger immunity against viral infections effectively
- Common Viral Vaccines: Examples like measles, influenza, and COVID-19 vaccines detailed
- Challenges in Vaccine Creation: Issues like mutations, distribution, and public hesitancy addressed
![]()
Vaccine Development Process: Steps from virus identification to clinical trials and approval
Vaccine development is a meticulous, multi-stage process that begins long before a vial reaches a clinic. It starts with virus identification, where scientists isolate and characterize the pathogen causing disease. For instance, during the COVID-19 pandemic, the SARS-CoV-2 virus was sequenced within weeks of its discovery, enabling rapid vaccine development. This step is critical because understanding the virus’s genetic makeup and behavior informs the type of vaccine—whether mRNA, viral vector, or protein subunit—that will be most effective. Without precise identification, the entire process falters.
Once the virus is identified, preclinical development begins. Here, researchers test potential vaccine candidates in lab settings, often using cell cultures and animal models. For example, mRNA vaccines like Pfizer-BioNTech’s require synthesizing genetic material that instructs cells to produce viral proteins, triggering an immune response. This phase also involves determining dosage levels; for instance, the Moderna COVID-19 vaccine uses a 100-microgram dose for adults, while Pfizer’s is 30 micrograms. Safety and efficacy data from this stage must be robust enough to justify advancing to human trials.
The transition to clinical trials is a pivotal moment, divided into three phases. Phase 1 focuses on safety, testing the vaccine on a small group (20–100 volunteers) to identify side effects and immune responses. Phase 2 expands to hundreds of participants, refining dosage and gathering more safety data. Phase 3 involves thousands of people, assessing efficacy by comparing vaccinated groups to placebos. For instance, the Pfizer COVID-19 vaccine’s Phase 3 trial included 44,000 participants, demonstrating 95% efficacy. Each phase must meet strict regulatory criteria before proceeding, ensuring public safety.
After successful clinical trials, regulatory approval is sought. In the U.S., the FDA reviews all data, often granting Emergency Use Authorization (EUA) during crises, as seen with COVID-19 vaccines. Full approval follows further long-term studies. Post-approval, phase 4 monitoring tracks the vaccine’s performance in the general population, identifying rare side effects. For example, the rare link between the Johnson & Johnson vaccine and blood clots was detected during this phase. This ongoing surveillance ensures vaccines remain safe and effective for all age groups, from children (e.g., Pfizer’s 10-microgram dose for 5–11-year-olds) to seniors.
Practical tips for the public include staying informed about vaccine schedules, reporting side effects to healthcare providers, and following dosage instructions precisely. For instance, mRNA vaccines typically require two doses spaced 3–4 weeks apart, while viral vector vaccines like AstraZeneca’s may need a single dose or a longer interval. Understanding this process fosters trust and highlights the rigor behind vaccine development, from lab to arm.
Norovirus Vaccine Progress: How Close Are We to Prevention?
You may want to see also
Explore related products






![]()
Types of Viral Vaccines: Live-attenuated, inactivated, mRNA, and viral vector vaccines explained
Vaccines are humanity’s most powerful tool against viral infections, each type designed to trigger immunity without causing disease. Among the arsenal, four stand out: live-attenuated, inactivated, mRNA, and viral vector vaccines. Each harnesses distinct mechanisms to prepare the immune system for future threats, tailored to the virus’s nature and the population’s needs. Understanding these types reveals how science adapts to outsmart pathogens.
Live-attenuated vaccines use weakened viruses that still replicate but don’t cause illness in healthy individuals. Examples include the measles, mumps, and rubella (MMR) vaccine and the oral polio vaccine. These vaccines mimic natural infection, prompting a robust immune response with just one or two doses. However, they’re contraindicated for immunocompromised individuals, as the attenuated virus could revert to a virulent form. Storage requires refrigeration (2–8°C), and they’re typically administered to children over 12 months old, though the MMR is given as early as 12 months. Their longevity is a key advantage, often conferring lifelong immunity after a booster.
Inactivated vaccines, in contrast, use viruses killed by chemicals, heat, or radiation. The flu shot and the injected polio vaccine are prime examples. While safer for immunocompromised individuals, they elicit a weaker immune response, necessitating multiple doses (e.g., two doses of the flu vaccine for children under 9) and periodic boosters. These vaccines are stable at room temperature for short periods but are typically stored refrigerated. Their simplicity in production and safety profile make them ideal for rapid deployment during outbreaks, though their efficacy often wanes faster than live-attenuated counterparts.
MRNA vaccines, a breakthrough in vaccinology, deliver genetic instructions for cells to produce a viral protein, triggering an immune response. Pfizer-BioNTech and Moderna’s COVID-19 vaccines are pioneering examples. Administered in two doses (3–4 weeks apart for adults), they require ultra-cold storage (-70°C for Pfizer, -20°C for Moderna) initially, though thawed vials can be refrigerated for up to 30 days. Their rapid development and high efficacy (90–95%) highlight their potential for future pandemics. However, their novelty means long-term effects are still under study, and they’re currently approved for ages 6 months and up.
Viral vector vaccines use a harmless virus (e.g., adenovirus) to deliver genetic material encoding a viral antigen. Johnson & Johnson’s COVID-19 vaccine and AstraZeneca’s Vaxzevria are notable examples. A single dose is often sufficient, making them logistically simpler, though rare side effects like thrombosis with thrombocytopenia syndrome (TTS) have limited their use in younger populations. Stored at 2–8°C, they’re stable and cost-effective, ideal for low-resource settings. Their versatility allows adaptation to emerging variants, though immune responses may be less durable than mRNA vaccines.
Each vaccine type balances efficacy, safety, and practicality. Live-attenuated vaccines offer robust immunity but pose risks for vulnerable groups. Inactivated vaccines prioritize safety but require boosters. mRNA vaccines revolutionize speed and efficacy but demand stringent storage. Viral vector vaccines combine simplicity and adaptability but carry rare risks. Choosing the right type depends on the virus, population, and infrastructure—a testament to science’s ingenuity in safeguarding global health.
Disney's Vaccination Rules: Proof Required?
You may want to see also
Explore related products






![]()
Immune Response Mechanisms: How vaccines trigger immunity against viral infections effectively
Vaccines are not just biological products; they are precision tools designed to harness the immune system’s memory. At their core, they introduce a harmless piece of a virus—such as a protein fragment or inactivated pathogen—to trigger an immune response without causing disease. For instance, the mRNA vaccines against SARS-CoV-2 encode the virus’s spike protein, prompting cells to produce it temporarily. This process mimics a natural infection, but with a critical difference: the immune system learns to recognize and neutralize the threat without facing the virus’s full virulence. The key lies in antigen presentation, where dendritic cells engulf the vaccine’s components and display them to T cells, initiating a cascade of immune activation.
Consider the step-by-step mechanism of how vaccines activate immunity. First, the vaccine is administered, often via intramuscular injection, delivering the antigen directly to muscle tissue. Within hours, dendritic cells migrate to the injection site, engulf the antigen, and travel to lymph nodes. Here, they present the antigen to naïve T cells, which differentiate into helper T cells and cytotoxic T cells. Helper T cells secrete cytokines, amplifying the immune response, while cytotoxic T cells target and destroy infected cells. Simultaneously, B cells activated by the antigen mature into plasma cells, producing antibodies specific to the virus. This dual response—cellular and humoral—ensures both immediate and long-term protection. For optimal efficacy, most vaccines require multiple doses, such as the two-dose regimen for Pfizer-BioNTech’s COVID-19 vaccine, spaced 3–4 weeks apart, to reinforce immune memory.
A critical yet often overlooked aspect is the role of adjuvants in enhancing vaccine efficacy. Adjuvants, such as aluminum salts (alum) or lipid nanoparticles, are added to vaccines to bolster the immune response. They create localized inflammation, attracting immune cells to the injection site and prolonging antigen exposure. For example, the HPV vaccine uses alum to increase antibody production, while mRNA vaccines rely on lipid nanoparticles to protect and deliver genetic material. However, adjuvants must be carefully calibrated; excessive inflammation can lead to adverse reactions. Practical tip: If experiencing mild swelling or pain at the injection site, apply a cold compress for 10–15 minutes to reduce discomfort, but avoid anti-inflammatory medications like ibuprofen, as they may dampen the immune response.
Comparing vaccine types reveals distinct immune activation strategies. Live-attenuated vaccines, like the measles-mumps-rubella (MMR) vaccine, use weakened viruses to elicit a robust, long-lasting immune response, often requiring only one or two doses. In contrast, inactivated vaccines, such as the injectable flu shot, contain killed viruses and typically necessitate annual boosters due to waning immunity. Subunit vaccines, like the hepatitis B vaccine, use isolated viral proteins and often include adjuvants to compensate for reduced immunogenicity. Each type leverages different immune pathways, highlighting the importance of tailoring vaccine design to the target virus. For parents, ensuring children receive the full MMR series (first dose at 12–15 months, second at 4–6 years) is crucial for herd immunity against highly contagious diseases.
The ultimate takeaway is that vaccines are not just preventive measures; they are educators of the immune system. By mimicking infection without causing harm, they train the body to mount a swift, effective response upon future exposure. This mechanism relies on precise antigen delivery, immune cell activation, and memory formation. Practical advice: Keep a vaccination record for all family members, noting dates, types, and doses, to ensure timely boosters and compliance with age-specific recommendations. For adults, consider the Tdap vaccine (tetanus, diphtheria, pertussis) every 10 years and annual flu shots, especially for those over 65 or with chronic conditions. Understanding these mechanisms empowers individuals to make informed decisions, transforming passive recipients into active participants in their health.
Tractor Supply Pet Vaccinations: Do They Include Health Certificates?
You may want to see also
Explore related products






![]()
Common Viral Vaccines: Examples like measles, influenza, and COVID-19 vaccines detailed
Vaccines against viruses are meticulously designed to mimic infection, triggering immune responses without causing disease. Among the most impactful are those targeting measles, influenza, and COVID-19. Each vaccine type employs distinct strategies—live-attenuated, inactivated, or mRNA-based—to protect against viral threats. Understanding their mechanisms, dosages, and administration protocols is essential for maximizing their efficacy and public health impact.
Consider the measles vaccine, a cornerstone of childhood immunization. Administered as part of the MMR (measles, mumps, rubella) vaccine, it uses live-attenuated viruses to stimulate lifelong immunity. The CDC recommends the first dose at 12–15 months and the second at 4–6 years. This two-dose regimen achieves 97% effectiveness, nearly eradicating a disease once responsible for millions of annual deaths. Notably, the vaccine’s success hinges on high community uptake to maintain herd immunity, protecting vulnerable populations like infants too young to be vaccinated.
In contrast, influenza vaccines exemplify the challenge of combating a rapidly mutating virus. Seasonal flu shots contain inactivated virus strains selected annually by the WHO based on global surveillance data. Adults require a single dose yearly, while children under 9 may need two doses in their first vaccination year. Despite moderate efficacy (40–60%), these vaccines reduce severe illness, hospitalizations, and deaths. Practical tips include getting vaccinated by October to ensure peak immunity during flu season and pairing vaccination with hygiene practices like handwashing.
The COVID-19 vaccines mark a revolutionary leap in vaccine technology, with mRNA platforms (Pfizer-BioNTech, Moderna) and viral vector approaches (Johnson & Johnson) leading the charge. mRNA vaccines encode for the SARS-CoV-2 spike protein, prompting immune cells to produce antibodies. The primary series involves two doses spaced 3–4 weeks apart for Pfizer and 4 weeks for Moderna, followed by boosters every 6–12 months to counter waning immunity and emerging variants. The J&J vaccine offers a single-dose option but requires a booster for enhanced protection. These vaccines have dramatically reduced severe outcomes, with real-world data showing over 90% efficacy against hospitalization and death.
Comparing these vaccines highlights the diversity of vaccine design and administration. Measles relies on lifelong immunity from a stable virus, influenza demands annual updates for mutating strains, and COVID-19 leverages cutting-edge technology for rapid response. Each underscores the importance of tailored strategies in viral prevention. For instance, while measles vaccination is a one-time commitment for most, influenza and COVID-19 require ongoing engagement with evolving public health guidelines. Practical takeaways include adhering to age-specific schedules, staying informed about booster recommendations, and recognizing that no vaccine is 100% effective—layering protections like masking during outbreaks remains crucial.
Ultimately, these vaccines exemplify humanity’s ability to adapt scientific innovation to combat viral threats. Their success depends not only on biological mechanisms but also on public trust, accessibility, and adherence to protocols. Whether protecting against a centuries-old scourge like measles or a novel pathogen like SARS-CoV-2, vaccines remain our most powerful tool in the fight against viral diseases.
Puppy Fatigue Post-Vaccination: Understanding Normal Tiredness After Shots
You may want to see also
Explore related products






![]()
Challenges in Vaccine Creation: Issues like mutations, distribution, and public hesitancy addressed
Vaccine development is a complex process, and creating effective vaccines against viruses presents unique challenges. One of the primary obstacles is the rapid mutation rate of viruses, which can render vaccines less effective over time. For instance, the influenza virus mutates frequently, necessitating annual updates to the flu vaccine. This constant evolution requires scientists to predict dominant strains months in advance, a task that is both intricate and uncertain. Such unpredictability highlights the need for innovative approaches, like universal vaccines targeting conserved viral regions, to stay ahead of these mutations.
Distribution of vaccines is another critical challenge, particularly in low-resource settings. The COVID-19 pandemic exposed global disparities in access to vaccines, with wealthier nations securing doses while others struggled. Cold chain requirements further complicate distribution, as many vaccines, like the Pfizer-BioNTech COVID-19 vaccine, require ultra-low temperatures (-70°C). To address this, organizations are exploring thermostable formulations and decentralized production models. For example, the World Health Organization’s COVID-19 Technology Access Pool aims to share vaccine technology with manufacturers in developing countries, ensuring equitable access.
Public hesitancy poses a significant barrier to vaccine uptake, fueled by misinformation and historical mistrust. Surveys show that vaccine confidence varies widely, with some regions reporting acceptance rates below 50%. Addressing this requires tailored communication strategies. Health professionals should engage communities through trusted messengers, such as local leaders or religious figures, and provide clear, culturally relevant information. For instance, debunking myths about vaccine ingredients or side effects can alleviate concerns. Additionally, transparent reporting of clinical trial data and post-vaccination monitoring can build trust.
Balancing speed and safety in vaccine development is a delicate challenge, as seen during the COVID-19 pandemic. While expedited approvals were necessary to curb the crisis, they sparked skepticism about safety. Regulatory bodies like the FDA and EMA implemented rigorous protocols, including large-scale trials and ongoing surveillance, to ensure vaccine efficacy and safety. For example, the mRNA vaccines underwent phase III trials with tens of thousands of participants, demonstrating high efficacy and minimal severe side effects. Communicating these processes to the public is essential to counter misinformation and foster confidence.
In conclusion, overcoming challenges in vaccine creation demands a multifaceted approach. From tackling viral mutations to ensuring equitable distribution and addressing public hesitancy, each issue requires innovative solutions and collaboration. By leveraging scientific advancements, improving global infrastructure, and fostering trust through transparent communication, we can enhance the effectiveness and reach of vaccines, ultimately saving lives and preventing future pandemics.
Vaccines' Lifesaving Impact: Estimating Lives Saved Globally Through Immunization
You may want to see also
Frequently asked questions
Vaccines against viruses are biological preparations that provide active, acquired immunity to specific viral infections. They work by introducing a harmless form of the virus (or its components) to the immune system, prompting it to produce antibodies and memory cells. This prepares the body to recognize and fight the virus if exposed in the future.
Vaccines against viruses are created using various methods, including live-attenuated vaccines (weakened virus), inactivated vaccines (killed virus), subunit vaccines (specific viral proteins), mRNA vaccines (genetic material encoding viral proteins), and viral vector vaccines (using another virus to deliver viral genes). Each method is chosen based on the virus and desired immune response.
Yes, vaccines against viruses are rigorously tested for safety and efficacy before approval. They are highly effective in preventing or reducing the severity of viral infections, protecting individuals and communities through herd immunity. Benefits include saving lives, reducing healthcare costs, and preventing outbreaks of diseases like measles, influenza, and COVID-19.