Vaccine-related injuries, though rare, are a topic of significant interest and concern for both the public and healthcare professionals. While vaccines are widely recognized as one of the most effective tools in preventing infectious diseases, no medical intervention is entirely without risk. The most common vaccine-related injuries typically include mild to moderate side effects such as soreness at the injection site, fever, fatigue, and headaches, which are generally short-lived and resolve on their own. More serious but extremely rare adverse events, such as anaphylaxis, shoulder injury related to vaccine administration (SIRVA), or conditions like Guillain-Barré syndrome, have been documented but occur at very low rates. Understanding these potential risks is crucial for informed decision-making and maintaining public trust in vaccination programs.
Explore related products






What You'll Learn
![]()
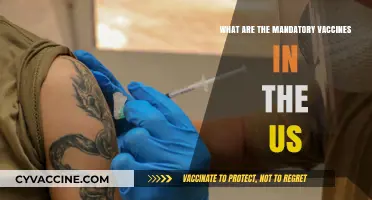
Shoulder Injuries Related to Vaccine Administration (SIRVA)
Vaccine administration, while generally safe, can occasionally lead to specific injuries, one of the most recognized being Shoulder Injury Related to Vaccine Administration (SIRVA). This condition arises not from the vaccine itself but from improper injection technique, typically involving the deltoid muscle. SIRVA occurs when a vaccine is injected too high or too deep in the arm, causing inflammation of the bursa, tendons, or other structures in the shoulder. Symptoms often include persistent pain, limited range of motion, and weakness, which can manifest within 48 hours of vaccination and may worsen over time if untreated.
To prevent SIRVA, healthcare providers must adhere to precise injection guidelines. The deltoid muscle, located in the lateral upper arm, is the recommended site for most vaccines, including influenza, COVID-19, and tetanus. The needle should be inserted at a 90-degree angle, with the length varying by patient age and size: 5/8 inch for adults and adolescents, and 3/8 to 5/8 inch for children, depending on their arm circumference. Avoiding the upper third of the arm and ensuring the needle does not penetrate too deeply are critical steps to minimize risk. Patients should also be educated to report any unusual shoulder pain post-vaccination promptly.
Diagnosing SIRVA involves ruling out other causes of shoulder pain, such as rotator cuff injuries or arthritis. Imaging studies like MRI or ultrasound may reveal inflammation or fluid accumulation in the shoulder joint. Treatment typically includes physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), and corticosteroid injections. In severe cases, surgical intervention may be necessary to repair damaged tissues. Early intervention is key to recovery, as prolonged inflammation can lead to chronic pain and disability.
While SIRVA is rare, its impact on quality of life can be significant, particularly for individuals who rely on their shoulder function for work or daily activities. Awareness and proper training for vaccinators are essential to reduce incidence rates. Patients should also be proactive in monitoring their symptoms and seeking care if shoulder pain persists beyond the typical post-vaccination soreness, which usually resolves within a few days. By addressing SIRVA promptly, individuals can avoid long-term complications and maintain their mobility and comfort.
Is Polio Still a Standard Vaccine in the US?
You may want to see also
Explore related products

$20.41 $21.95





![]()
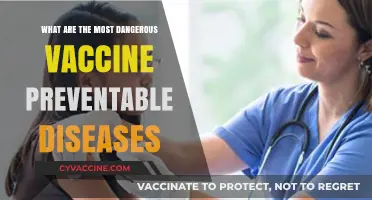
Anaphylaxis and Severe Allergic Reactions Post-Vaccination
Anaphylaxis, a severe and potentially life-threatening allergic reaction, is a rare but critical concern following vaccination. While vaccines are rigorously tested for safety, a small subset of individuals may experience this rapid onset reaction, typically within minutes to hours post-inoculation. The Centers for Disease Control and Prevention (CDC) reports an incidence rate of approximately 1.31 cases per million vaccine doses administered, highlighting its rarity but underscoring the need for vigilance. Common vaccines associated with anaphylaxis include influenza, COVID-19 mRNA vaccines, and childhood immunizations like MMR. Recognizing symptoms—such as hives, swelling of the face or throat, difficulty breathing, rapid heartbeat, and dizziness—is crucial for immediate intervention.
The mechanism behind vaccine-induced anaphylaxis often involves hypersensitivity to specific components, such as polyethylene glycol (PEG) in mRNA vaccines or gelatin in certain flu vaccines. For instance, the Pfizer-BioNTech and Moderna COVID-19 vaccines contain PEG, a known allergen, which has been linked to severe reactions in sensitive individuals. Healthcare providers typically screen for such allergies pre-vaccination, but some cases may go undetected. Individuals with a history of severe allergies, particularly to vaccine components, should discuss risks with their healthcare provider and be monitored for 15–30 minutes post-vaccination, as per CDC guidelines.
Managing anaphylaxis requires prompt administration of epinephrine, the first-line treatment. Healthcare facilities and vaccination sites are equipped with auto-injectors (e.g., EpiPen) for immediate use. If symptoms occur at home, individuals should seek emergency care without delay. Long-term strategies include allergen avoidance and consultation with an allergist for comprehensive testing. Notably, the benefits of vaccination in preventing serious diseases far outweigh the risks of anaphylaxis, but informed decision-making and preparedness are essential.
Comparatively, while anaphylaxis is rare, its severity demands attention. Unlike milder reactions like soreness or fever, anaphylaxis requires immediate medical intervention. Public awareness campaigns and healthcare provider training can improve outcomes. For example, the CDC’s Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) monitor such reactions, ensuring ongoing safety evaluations. Parents and caregivers should remain vigilant, especially when vaccinating children, as timely response can be lifesaving.
In conclusion, while anaphylaxis post-vaccination is uncommon, its potential impact necessitates awareness and preparedness. Understanding risk factors, recognizing symptoms, and knowing how to respond are critical steps in mitigating harm. Vaccines remain a cornerstone of public health, and addressing rare adverse events transparently fosters trust in immunization programs. For those at higher risk, personalized medical advice and post-vaccination monitoring are invaluable tools in ensuring safety while reaping the protective benefits of vaccines.
Can You Test for Past Vaccination? Exploring Methods and Limitations
You may want to see also
Explore related products






![]()
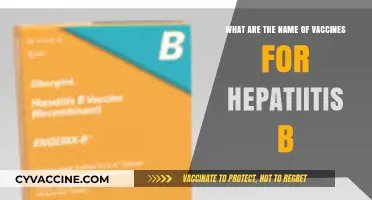
Guillain-Barré Syndrome (GBS) Linked to Certain Vaccines
Guillain-Barré Syndrome (GBS) is a rare but serious autoimmune disorder where the body’s immune system mistakenly attacks the peripheral nervous system, leading to muscle weakness, numbness, and sometimes paralysis. While its exact cause remains unclear, certain vaccines have been statistically linked to a small increased risk of GBS, most notably the 1976 swine flu vaccine and, more recently, some COVID-19 vaccines. The risk is exceptionally low—approximately 1 to 2 cases per 100,000 vaccinated individuals—but understanding this connection is critical for informed decision-making.
Consider the 1976 swine flu vaccination campaign, where GBS occurred in about 1 additional person per 100,000 vaccinated, compared to the baseline risk of 1 to 2 cases per 100,000 people annually. This historical example highlights how vaccine-related GBS, though rare, can emerge as a significant concern during mass immunization efforts. Modern surveillance systems, such as the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD), now play a crucial role in detecting and investigating such patterns, ensuring swift responses to potential risks.
For COVID-19 vaccines, specifically the Janssen (Johnson & Johnson) vaccine, data from the Centers for Disease Control and Prevention (CDC) identified 15 confirmed GBS cases among 12.5 million recipients, translating to a risk of approximately 7.5 cases per million doses. In contrast, the Pfizer-BioNTech and Moderna mRNA vaccines have shown no significant association with GBS. This disparity underscores the importance of vaccine-specific risk assessments and the need for healthcare providers to discuss these nuances with patients, particularly those with a history of GBS or other neurological conditions.
If you suspect GBS post-vaccination, immediate medical attention is essential. Symptoms typically begin with tingling or weakness in the legs, progressing upward, and may include difficulty breathing or swallowing in severe cases. Treatment options, such as intravenous immunoglobulin (IVIG) or plasmapheresis, can help manage symptoms and speed recovery. While most individuals recover fully, some may experience lingering weakness or fatigue, emphasizing the need for early intervention.
In weighing the risks, it’s vital to contextualize GBS against the diseases vaccines prevent. For instance, COVID-19 itself carries a higher risk of neurological complications, including GBS, than the vaccines designed to combat it. The CDC and World Health Organization (WHO) maintain that the benefits of vaccination far outweigh the rare risks of GBS, particularly for vulnerable populations. By staying informed and consulting healthcare professionals, individuals can make choices that balance protection against both infectious diseases and potential vaccine-related adverse events.
Unvaccinated Autism Cases: Exploring the Link and Dispelling Myths
You may want to see also
Explore related products






![]()
Vasovagal Syncope (Fainting) After Immunization
Vasovagal syncope, commonly known as fainting, is a transient loss of consciousness triggered by a sudden drop in blood pressure and heart rate. Among vaccine-related injuries, it stands out as a well-documented yet often misunderstood phenomenon, particularly following immunization. This reaction is not an allergic response or a direct injury from the vaccine itself but rather a reflexive physiological event. It typically occurs within minutes to an hour after vaccination, most frequently in adolescents and young adults, though it can affect individuals of any age. The sight of a needle, pain, or even the anxiety surrounding the procedure can activate the vasovagal response, leading to dizziness, nausea, and ultimately, fainting.
Understanding the mechanism behind vasovagal syncope is crucial for both healthcare providers and recipients. When the body perceives stress or pain, the vagus nerve stimulates a decrease in heart rate and blood pressure, diverting blood flow away from the brain. This can result in temporary unconsciousness. In the context of immunization, the event is often exacerbated by factors such as dehydration, lack of food, or a history of similar episodes. For instance, a 16-year-old receiving the HPV vaccine might faint if they skipped breakfast or were anxious about the injection. While alarming, vasovagal syncope is generally benign and resolves quickly with proper positioning and care.
Prevention and management are key to minimizing the risk of fainting after immunization. Healthcare providers should encourage patients to eat a light meal and stay hydrated before their appointment. Sitting or lying down during the procedure can also help maintain blood flow to the brain. If a patient feels lightheaded or nauseous, they should be immediately placed in a supine position with their legs elevated to restore circulation. For those with a known history of fainting, vaccination should be administered while the individual is reclined, and they should remain seated for at least 15 minutes post-injection. These simple measures can significantly reduce the likelihood of syncope.
Comparatively, vasovagal syncope is far more common than severe vaccine-related injuries, such as anaphylaxis, which occurs in approximately 1.3 cases per million doses. Its transient nature and lack of long-term consequences make it a manageable side effect rather than a cause for alarm. However, the psychological impact of fainting should not be overlooked, as it can deter individuals from completing their vaccination schedules. Educating patients about the possibility of vasovagal syncope and reassuring them of its harmless nature can alleviate anxiety and foster trust in immunization programs.
In conclusion, vasovagal syncope after immunization is a predictable and preventable event rooted in the body’s natural response to stress or pain. By recognizing its triggers, implementing simple precautions, and providing immediate care when necessary, healthcare providers can ensure a safer vaccination experience. For patients, understanding that fainting is a temporary and non-life-threatening reaction can reduce fear and encourage compliance with recommended immunizations. With proper awareness and preparation, vasovagal syncope need not be a barrier to protecting public health through vaccination.
Massachusetts Vaccination Requirements: What You Need to Know
You may want to see also
Explore related products






![]()
Thrombosis with Thrombocytopenia Syndrome (TTS) Post-Vaccination
Thrombosis with Thrombocytopenia Syndrome (TTS) is a rare but serious condition that has been linked to certain adenovirus vector-based COVID-19 vaccines, such as the Johnson & Johnson (Janssen) vaccine. This syndrome is characterized by the formation of blood clots, often in unusual locations like the brain (cerebral venous sinus thrombosis), combined with low platelet counts (thrombocytopenia). The incidence rate is approximately 7 per 1 million vaccinated individuals, predominantly affecting women under 50 years of age. Recognizing symptoms early—such as severe headache, abdominal pain, leg swelling, or easy bruising—is critical, as prompt treatment can significantly improve outcomes.
The mechanism behind TTS involves an abnormal immune response triggered by the vaccine, leading to the production of antibodies that activate platelets and promote clotting. Unlike typical blood clots, TTS requires specific management: standard blood thinners like heparin can worsen the condition, so alternative anticoagulants such as argatroban or fondaparinux are recommended. Corticosteroids may also be used to suppress the immune response. Healthcare providers must be aware of this distinction to avoid exacerbating the syndrome during treatment.
Prevention and risk mitigation are key when considering adenovirus vector vaccines. For individuals at higher risk—particularly younger women—mRNA vaccines (Pfizer-BioNTech or Moderna) are often preferred due to their lower association with TTS. If an adenovirus vector vaccine is administered, recipients should be educated about symptoms to monitor for up to three weeks post-vaccination. Public health messaging must balance transparency about risks with the broader benefits of vaccination, ensuring informed decision-making without fueling hesitancy.
From a comparative perspective, TTS stands out among vaccine-related injuries due to its unique pathophysiology and treatment requirements. While anaphylaxis and shoulder injuries (e.g., SIRVA) are more commonly discussed, TTS demands specialized clinical management and heightened vigilance. Its rarity underscores the importance of robust pharmacovigilance systems to detect and respond to such adverse events swiftly. This syndrome serves as a reminder that even rare complications require targeted strategies to protect public health effectively.
Post-Vaccination Cat Behavior: Understanding Aggression After Shots
You may want to see also
Frequently asked questions
The most common vaccine-related injuries include soreness, redness, or swelling at the injection site, mild fever, fatigue, headache, and muscle or joint pain. These are typically mild and resolve within a few days.
Serious vaccine-related injuries are rare but can include severe allergic reactions (anaphylaxis), shoulder injury related to vaccine administration (SIRVA), or, in very rare cases, conditions like Guillain-Barré syndrome (GBS) or thrombosis with thrombocytopenia syndrome (TTS).
Long-term health issues from vaccine-related injuries are extremely rare. Most reactions are temporary, and serious complications are monitored through systems like the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) to ensure ongoing safety.