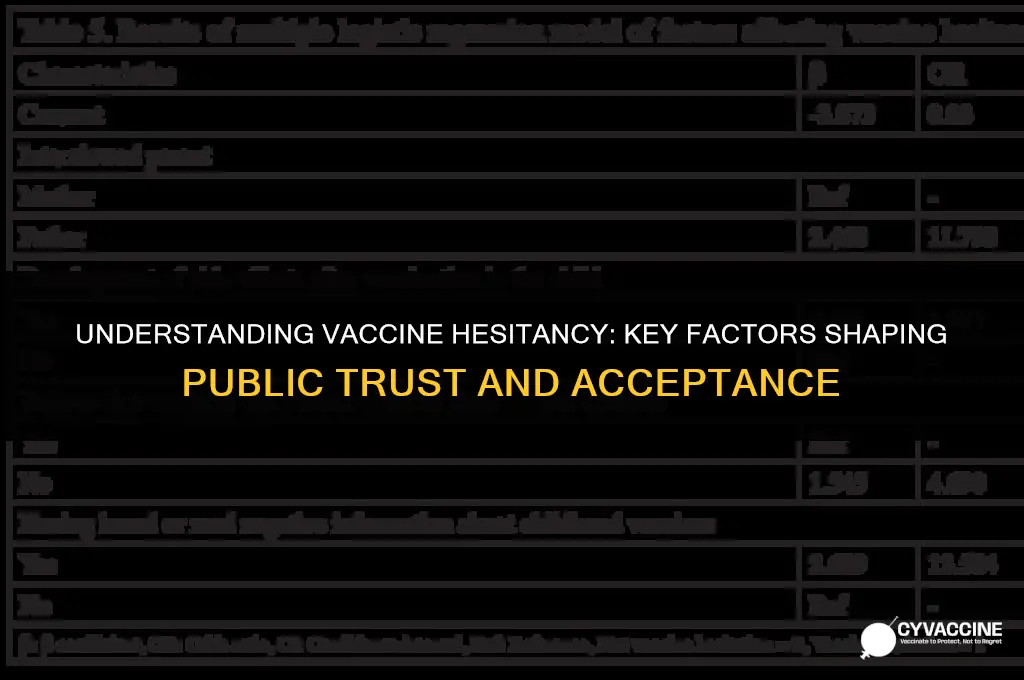
Vaccine hesitancy, the reluctance or refusal to receive vaccines despite their availability, has become a significant public health concern, influenced by a complex interplay of factors. Key contributors include misinformation and disinformation spread through social media and other platforms, eroding trust in scientific institutions and healthcare systems. Historical and cultural contexts, such as past medical injustices or religious beliefs, also play a role in shaping attitudes toward vaccines. Individual psychological factors, such as fear of side effects or perceived low risk of disease, further compound hesitancy. Additionally, systemic issues like inadequate healthcare access, political polarization, and inconsistent communication from authorities exacerbate the problem. Understanding these multifaceted influences is crucial for developing effective strategies to address vaccine hesitancy and promote widespread immunization.
| Characteristics | Values |
|---|---|
| Demographics | Age, gender, education level, socioeconomic status, geographic location. |
| Psychological Factors | Fear of side effects, mistrust of healthcare systems, conspiracy beliefs. |
| Cultural and Religious Beliefs | Perceived conflict with religious values, cultural norms, or traditions. |
| Information Sources | Reliance on social media, misinformation, lack of trusted information. |
| Historical Context | Past medical scandals, unethical experiments, or vaccine controversies. |
| Political Influence | Polarization, anti-vaccine movements, government distrust. |
| Perceived Risk vs. Benefit | Low perceived risk of disease, skepticism about vaccine efficacy. |
| Healthcare Access | Barriers to access, lack of healthcare infrastructure, cost concerns. |
| Individual Liberty | Belief in personal autonomy, resistance to mandates or coercion. |
| Previous Vaccine Experiences | Negative personal or familial experiences with vaccines. |
| Global and Local Context | Regional outbreaks, vaccine availability, and distribution challenges. |
| Educational Campaigns | Ineffective or insufficient public health messaging. |
| Social Norms | Influence of peers, family, or community attitudes toward vaccination. |
| Systemic Inequities | Historical or ongoing discrimination in healthcare systems. |
| Emerging Technologies | Skepticism about new vaccine technologies (e.g., mRNA vaccines). |
Explore related products

$26.21 $35




What You'll Learn
![]()
Misinformation and Disinformation Spread
The rapid spread of misinformation and disinformation about vaccines has become a critical factor in vaccine hesitancy, undermining public trust and health outcomes. Unlike organic myths, which may arise from misunderstandings, these falsehoods are often deliberately crafted and amplified through social media, exploiting algorithms that prioritize engagement over accuracy. A single viral post can reach millions, embedding doubts before factual corrections can catch up. For instance, the debunked claim linking the MMR vaccine to autism persists in online echo chambers, despite overwhelming scientific evidence to the contrary. This section dissects the mechanisms, impacts, and strategies to counter this insidious trend.
Consider the anatomy of a disinformation campaign: it typically begins with a kernel of truth, twisted to serve a narrative. For example, reports of rare side effects from COVID-19 vaccines were exaggerated and misrepresented to suggest widespread danger, ignoring the far greater risks of the disease itself. Such tactics prey on cognitive biases like the availability heuristic, where vivid but uncommon events overshadow statistical realities. Social media platforms, designed to maximize user interaction, inadvertently become accomplices by rewarding sensational content with greater visibility. A study by the *Journal of Experimental Psychology* found that false news spreads six times faster than factual information, partly because it triggers stronger emotional reactions.
To combat this, individuals must adopt a critical mindset when encountering vaccine-related content. Start by verifying the source: is it a reputable health organization like the WHO or CDC, or an unverified blog? Cross-reference claims with multiple credible outlets, and be wary of absolute statements or emotional appeals. For parents concerned about vaccine schedules, consult the CDC’s recommended timeline, which is rigorously tested for safety in specific age groups (e.g., the MMR vaccine is first administered at 12–15 months). Tools like fact-checking websites (e.g., PolitiFact, Snopes) can also help debunk myths in real time.
However, individual vigilance is not enough. Policymakers and tech companies must take proactive steps to curb the spread of falsehoods. Platforms like Facebook and Twitter have begun flagging misleading posts and promoting authoritative sources, but enforcement remains inconsistent. Governments can incentivize transparency by requiring social media companies to disclose the origins of viral content and penalize repeat offenders. Public health campaigns should also focus on media literacy, teaching people how to discern credible information from manipulative narratives. For instance, a program in Brazil reduced vaccine hesitancy by 20% by educating communities about disinformation tactics.
Ultimately, addressing misinformation and disinformation requires a multi-pronged approach that combines personal responsibility, technological solutions, and systemic interventions. The stakes are too high to ignore: a 5% drop in vaccination rates can lead to outbreaks of preventable diseases like measles, which saw a 30% global increase in cases between 2016 and 2019. By understanding the tactics behind false narratives and equipping ourselves with tools to counter them, we can rebuild trust in vaccines and protect public health for generations to come.
Cervical Cancer Prevention: The Role of HPV Vaccines Explained
You may want to see also
Explore related products






![]()
Historical and Cultural Mistrust in Healthcare
Historical injustices in healthcare have sown deep seeds of mistrust in marginalized communities, and these seeds continue to bear fruit in the form of vaccine hesitancy. The Tuskegee Syphilis Study, where Black men were deliberately left untreated for syphilis without their informed consent, stands as a stark example. This betrayal, spanning four decades, eroded trust in medical institutions and remains a cautionary tale. Similarly, forced sterilization programs targeting Indigenous women in North America and ethnic minorities globally have left a legacy of fear and suspicion. These historical wrongs are not mere footnotes in history books; they are living memories passed down through generations, shaping perceptions of healthcare systems and fueling skepticism towards interventions like vaccines.
Cultural beliefs and traditions often clash with Western medical paradigms, creating another layer of mistrust. In some communities, illness is viewed through a spiritual or holistic lens, where vaccines, seen as foreign substances, disrupt natural balance. For instance, in parts of Africa and Asia, rumors linking vaccines to infertility or Western population control efforts have spread, rooted in colonial histories of exploitation. These beliefs, though unfounded, are deeply held and cannot be dismissed as mere ignorance. Instead, they highlight the need for culturally sensitive communication that acknowledges these perspectives while providing accurate, context-specific information.
Addressing historical and cultural mistrust requires more than just data and facts. It demands a reckoning with the past and a commitment to rebuilding trust through transparency, inclusivity, and respect. Healthcare providers must engage with communities on their terms, involving local leaders and leveraging trusted figures to disseminate information. For example, in the rollout of the HPV vaccine in rural India, community health workers, often women from the same villages, played a pivotal role in dispelling myths and encouraging uptake. Similarly, in the U.S., initiatives like the COVID-19 Vaccine Education and Equity Initiative have partnered with Black churches to bridge the trust gap, recognizing the church’s role as a cultural and spiritual cornerstone.
Practical steps can further mitigate mistrust. First, healthcare systems must prioritize informed consent, ensuring individuals fully understand the benefits and risks of vaccination. Second, diverse representation in clinical trials and healthcare leadership can signal inclusivity and reduce perceptions of bias. Third, long-term community engagement, not just during health crises, can foster ongoing dialogue and trust. For instance, regular health fairs or workshops addressing broader health concerns, not just vaccines, can build rapport and credibility. Finally, acknowledging past wrongs openly and committing to ethical practices moving forward is essential. Without this, even the most scientifically sound vaccine campaigns risk falling on deaf ears.
The takeaway is clear: historical and cultural mistrust is not an irrational barrier but a rational response to systemic failures. Overcoming it requires humility, empathy, and a willingness to meet communities where they are. By addressing these deep-rooted issues head-on, we can pave the way for more equitable and effective public health interventions, ensuring vaccines reach those who need them most.
Locate Your Vaccination Records Easily with CVS: A Quick Guide
You may want to see also
Explore related products




![]()
Perceived Risks vs. Benefits of Vaccines
Vaccine hesitancy often hinges on the delicate balance individuals perceive between the risks and benefits of vaccination. This calculation is deeply personal, shaped by a mix of emotional, cultural, and informational factors. For instance, while clinical trials for the Pfizer-BioNTech COVID-19 vaccine demonstrated a 95% efficacy rate with minimal side effects (primarily mild to moderate fatigue or soreness), some individuals fixate on rare adverse events like anaphylaxis, which occurs in approximately 2 to 5 cases per million doses. This disparity in focus highlights how perceived risks can overshadow statistically proven benefits, even when data overwhelmingly favors vaccination.
Consider the MMR (measles, mumps, rubella) vaccine, which has been a cornerstone of pediatric immunization for decades. Despite its success in reducing measles cases by 99% globally since its introduction, misinformation linking it to autism persists, despite the original study being retracted and debunked. This illustrates how perceived risks, even when unfounded, can persist and influence decision-making. Parents weighing the decision often grapple with abstract fears versus tangible benefits, such as protecting their child from potentially life-threatening diseases. A practical tip for addressing this imbalance is to contextualize risks: compare the likelihood of vaccine side effects (e.g., a 1 in 1 million chance of severe allergic reaction) to the risks of the disease itself (e.g., a 1 in 1,000 chance of measles complications like encephalitis).
To navigate this tension effectively, healthcare providers can employ a three-step approach. First, acknowledge concerns without dismissing them. For example, if a patient expresses worry about vaccine ingredients like thimerosal, explain its purpose as a preservative and its safety in trace amounts. Second, provide tailored information that aligns with the individual’s specific fears. For instance, a pregnant woman concerned about the flu vaccine might benefit from knowing that it not only protects her but also confers immunity to her newborn for the first six months of life. Finally, frame benefits in relatable terms. Instead of citing broad statistics, share real-world examples, such as how the HPV vaccine has reduced cervical cancer rates by 88% in countries with high uptake.
A comparative analysis further underscores the importance of this balance. In countries with high vaccine confidence, such as Portugal and South Korea, public health campaigns emphasize both the collective benefits of herd immunity and the individual protection vaccines offer. Conversely, in regions with lower uptake, messaging often fails to address specific concerns or relies on fear-based tactics, which can backfire by amplifying perceived risks. For example, during the H1N1 pandemic, some campaigns focused on the severity of the disease, inadvertently heightening anxiety without providing actionable reassurance about vaccine safety.
Ultimately, bridging the gap between perceived risks and benefits requires a nuanced understanding of individual perspectives. By combining empathy, evidence-based communication, and practical context, stakeholders can help individuals make informed decisions. A key takeaway is that addressing hesitancy isn’t about overwhelming with data but about aligning information with personal values and concerns. For instance, emphasizing how vaccines protect not just the individual but also vulnerable populations, such as the elderly or immunocompromised, can reframe the decision as a communal act of responsibility rather than a solitary risk assessment.
Protocol Shift in Vaccine Manufacturing: Impact and Implications Explored
You may want to see also
Explore related products





![]()
Political and Religious Influences on Beliefs
Political and religious institutions wield significant influence over public health decisions, often shaping vaccine hesitancy through their stances and messaging. For instance, during the COVID-19 pandemic, some political leaders downplayed the severity of the virus or questioned the efficacy of vaccines, sowing doubt among their followers. This skepticism was amplified through social media and partisan news outlets, creating echo chambers where misinformation thrived. In countries with polarized political landscapes, such as the United States, vaccine uptake often correlated with political affiliation, highlighting how trust in institutions—or lack thereof—can directly impact public health behaviors.
Religious beliefs also play a pivotal role in vaccine hesitancy, particularly when vaccines are perceived to conflict with spiritual or moral principles. For example, some religious groups have opposed vaccines containing components derived from fetal cells, even when these cells were obtained decades ago and are no longer directly involved in production. In such cases, religious leaders often become gatekeepers of information, interpreting scientific data through a theological lens. Their endorsements or condemnations can sway entire communities, as seen in the measles outbreaks linked to religious exemptions in the U.S. and Europe. Engaging religious leaders in public health dialogues and providing culturally sensitive education can help bridge these divides.
A comparative analysis reveals that political and religious influences often intersect, particularly in regions where these institutions are deeply intertwined. In some African and Middle Eastern countries, political leaders leverage religious rhetoric to shape public opinion on vaccines, blending health policy with spiritual authority. Conversely, in secular societies, political ideologies alone may drive hesitancy, as seen in anti-establishment movements that view vaccines as symbols of government overreach. Understanding these dynamics is crucial for tailoring interventions: in religiously influenced areas, collaborating with faith leaders may be more effective than purely scientific messaging, while politically driven hesitancy may require rebuilding trust in public institutions.
To address these challenges, public health strategies must be context-specific and multifaceted. For politically influenced hesitancy, transparent communication from non-partisan sources, such as trusted healthcare providers or international organizations, can counter misinformation. In religious communities, involving clergy in vaccine education campaigns and ensuring vaccine formulations align with religious concerns (e.g., halal or kosher certifications) can foster acceptance. Practical steps include organizing town hall meetings with local leaders, distributing educational materials in accessible languages, and leveraging community-based organizations to disseminate accurate information. By acknowledging and respecting these influences, public health efforts can navigate the complex terrain of political and religious beliefs to promote vaccine confidence.
Vaccine Patent Ownership: CDC and Members
You may want to see also
Explore related products






![]()
Lack of Trust in Pharmaceutical Companies and Governments
Historical scandals and perceived prioritization of profit over public health have eroded trust in pharmaceutical companies, fueling vaccine hesitancy. The 1976 swine flu vaccine campaign, rushed to market under political pressure, resulted in rare but severe side effects like Guillain-Barré syndrome. This incident left a lasting legacy of skepticism, amplified by modern controversies like the Vioxx recall in 2004, where Merck & Co. was accused of downplaying cardiovascular risks. Such events create a narrative of corporate greed, making individuals question whether vaccine safety is truly paramount or secondary to financial gain.
Government involvement in vaccine development and distribution further complicates trust dynamics. During the COVID-19 pandemic, Operation Warp Speed accelerated vaccine production, raising concerns about shortcuts in safety testing. While regulatory agencies like the FDA maintained rigorous standards, the speed of approvals and political rhetoric surrounding the vaccines sowed doubt. For instance, the temporary pause of the Johnson & Johnson vaccine due to rare blood clots, though a sign of vigilant monitoring, was weaponized by skeptics as evidence of hidden dangers. This interplay between pharmaceutical companies and governments creates a feedback loop of mistrust, where actions intended to protect public health are reinterpreted as evidence of malfeasance.
To rebuild trust, transparency is non-negotiable. Pharmaceutical companies must disclose all trial data, including adverse events, in accessible formats. Governments should establish independent oversight committees to review vaccine safety data publicly. For example, publishing detailed phase III trial results for the Pfizer-BioNTech COVID-19 vaccine, which involved 43,000 participants, could demonstrate the robustness of the process. Additionally, engaging local healthcare providers as trusted messengers can bridge the gap between institutions and communities, as studies show individuals are more likely to accept vaccines recommended by their personal doctors.
A comparative analysis reveals that countries with higher trust in institutions, such as Denmark and South Korea, achieved significantly higher vaccination rates during the pandemic. In contrast, nations with historical grievances against governments, like France and Eastern European countries, faced greater hesitancy. This underscores the importance of addressing systemic distrust through consistent, ethical behavior. For instance, Denmark’s transparent communication about rare side effects of the AstraZeneca vaccine, coupled with a clear risk-benefit explanation, maintained public confidence. Emulating such strategies globally could mitigate hesitancy rooted in institutional mistrust.
Ultimately, rebuilding trust requires acknowledging past failures and committing to a new standard of accountability. Pharmaceutical companies and governments must prioritize long-term credibility over short-term gains. Practical steps include mandatory post-market surveillance for all vaccines, with real-time data sharing, and public forums for addressing concerns. For parents hesitant to vaccinate children, providing age-specific safety data—such as the 90.7% efficacy of the Pfizer vaccine in 5-11-year-olds—can alleviate fears. By treating trust as a fragile resource, institutions can begin to reverse the tide of vaccine hesitancy.
Vaccines and Vertigo: Unraveling the Potential Triggers of Dizziness
You may want to see also
Frequently asked questions
Misinformation (false information spread unintentionally) and disinformation (false information spread deliberately) are major factors in vaccine hesitancy. They often spread through social media, leading to confusion, fear, and mistrust of vaccines.
Historical events, such as unethical medical experiments on marginalized communities, and ongoing systemic inequalities in healthcare foster mistrust. This mistrust can lead individuals to question the safety and motives behind vaccines.
Political polarization can turn public health issues like vaccination into partisan debates, influencing individuals' decisions based on political affiliation rather than scientific evidence. This politicization undermines trust in vaccines and public health authorities.
Personal beliefs, including religious, philosophical, or alternative health perspectives, can shape attitudes toward vaccines. Cultural norms and traditions may also influence acceptance, particularly in communities where vaccines are perceived as conflicting with cultural values.