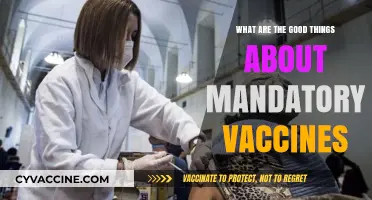
Vaccines are developed through various methods, each tailored to target specific pathogens and elicit a robust immune response. The primary approaches include live-attenuated vaccines, which use weakened forms of the virus or bacteria to stimulate immunity; inactivated vaccines, where pathogens are killed to eliminate their ability to cause disease while retaining their antigenic properties; subunit, recombinant, or conjugate vaccines, which contain specific pieces of the pathogen, such as proteins or sugars, to trigger an immune response; mRNA vaccines, a newer technology that delivers genetic material to instruct cells to produce a harmless viral protein, prompting the immune system to recognize and combat it; and viral vector vaccines, which use a modified, harmless virus to deliver genetic material encoding the pathogen’s antigen. Each method has unique advantages and applications, depending on the disease and desired immune response.
| Characteristics | Values |
|---|---|
| Live-Attenuated Vaccines | Weakened (attenuated) form of the virus or bacteria. Replicates in the body without causing disease. Examples: Measles, Mumps, Rubella (MMR), Varicella (Chickenpox). |
| Inactivated (Killed) Vaccines | Viruses or bacteria are killed using heat or chemicals. Cannot replicate. Examples: Influenza (Flu), Hepatitis A, Rabies, Polio (IPV). |
| Subunit, Recombinant, or Conjugate Vaccines | Use specific pieces of a pathogen (proteins, sugars) rather than the whole organism. Examples: Hepatitis B, Human Papillomavirus (HPV), Meningococcal, DTaP (Diphtheria, Tetanus, Pertussis). |
| mRNA Vaccines | Use messenger RNA to instruct cells to produce a protein that triggers an immune response. Examples: Pfizer-BioNTech and Moderna COVID-19 vaccines. |
| Viral Vector Vaccines | Use a modified, harmless virus (vector) to deliver genetic material encoding an antigen. Examples: Johnson & Johnson and AstraZeneca COVID-19 vaccines, Ebola (Ervebo). |
| Protein Subunit Vaccines | Contain purified pieces of the pathogen (e.g., proteins) to stimulate an immune response. Examples: Novavax COVID-19 vaccine, Shingles (Shingrix). |
| Toxoid Vaccines | Use inactivated toxins (toxoids) produced by bacteria to induce immunity. Examples: Tetanus, Diphtheria. |
| DNA Vaccines | Introduce a plasmid containing the DNA encoding an antigen. Still experimental, but in development for diseases like Zika, HIV, and certain cancers. |
| Whole-Cell Vaccines | Use entire bacteria or viruses (inactivated or attenuated). Examples: Pertussis (Whole-cell DTP), Typhoid (Ty21a). |
| Conjugate Vaccines | Combine a weak antigen (e.g., polysaccharide) with a strong antigen (e.g., protein) to enhance immune response. Examples: Pneumococcal, Meningococcal, Haemophilus influenzae type b (Hib). |
| Synthetic Vaccines | Use artificially synthesized antigens or nanoparticles to mimic pathogens. Examples: Some experimental COVID-19 and cancer vaccines. |
| Adjuvanted Vaccines | Include adjuvants (substances like aluminum salts or oil-in-water emulsions) to enhance the immune response. Examples: Hepatitis B, HPV, some influenza vaccines. |
Explore related products






What You'll Learn
- Live-attenuated vaccines: Weakened viruses/bacteria stimulate immunity without causing disease
- Inactivated vaccines: Killed pathogens trigger immune response safely
- Subunit vaccines: Use specific pathogen parts (proteins/sugars) to induce immunity
- mRNA vaccines: Deliver genetic material to teach cells to produce antigens
- Viral vector vaccines: Modified viruses deliver pathogen genes to elicit immune response
![]()
Live-attenuated vaccines: Weakened viruses/bacteria stimulate immunity without causing disease
Live-attenuated vaccines harness the power of weakened pathogens to train the immune system without causing the disease they prevent. Unlike their inactivated counterparts, these vaccines use live viruses or bacteria that have been carefully modified to reduce their virulence. This attenuation allows them to replicate within the body, albeit at a much lower rate, triggering a robust immune response. The result? Long-lasting immunity that often requires fewer doses compared to other vaccine types.
Consider the measles, mumps, and rubella (MMR) vaccine, a classic example of a live-attenuated vaccine. Administered as a single shot, typically between 12 and 15 months of age, with a booster dose around 4 to 6 years, it provides lifelong protection against three highly contagious diseases. The weakened viruses in the MMR vaccine mimic a natural infection, prompting the body to produce antibodies and memory cells that stand ready to fight off future exposure. This approach is particularly effective for diseases caused by viruses, as it closely replicates the immune response to a natural infection.
However, live-attenuated vaccines are not without limitations. Because they contain live pathogens, they are generally not recommended for individuals with compromised immune systems, such as those undergoing chemotherapy or living with HIV. Pregnant women are also advised to avoid them, as there is a theoretical risk, though small, of the attenuated virus crossing the placenta. Additionally, these vaccines require careful storage, often needing refrigeration to maintain their potency. For instance, the varicella (chickenpox) vaccine, another live-attenuated vaccine, must be stored between 2°C and 8°C (36°F and 46°F) to remain effective.
Despite these cautions, live-attenuated vaccines remain a cornerstone of public health. Their ability to confer strong, long-lasting immunity with minimal doses makes them ideal for preventing diseases like yellow fever, rotavirus, and tuberculosis. For travelers to regions where yellow fever is endemic, a single dose of the live-attenuated vaccine provides lifelong protection and is often required for entry. Similarly, the rotavirus vaccine, given orally in two or three doses starting at 6 weeks of age, has dramatically reduced hospitalizations due to severe diarrhea in infants.
In conclusion, live-attenuated vaccines represent a sophisticated balance between safety and efficacy. By using weakened pathogens, they stimulate a natural immune response without the risk of causing disease. While they require careful handling and are not suitable for everyone, their impact on global health is undeniable. From childhood immunizations to travel requirements, these vaccines continue to play a vital role in protecting individuals and communities from preventable diseases.
Post-Vaccine Arm Movement: Safe Practices and What to Avoid
You may want to see also
Explore related products






![]()
Inactivated vaccines: Killed pathogens trigger immune response safely
Pathogens, once formidable foes, can be rendered harmless yet still provoke a protective immune response. This is the essence of inactivated vaccines, a cornerstone of preventive medicine. By killing viruses or bacteria through heat, chemicals, or radiation, scientists create a safe yet potent immunological trigger. Unlike live-attenuated vaccines, which use weakened pathogens, inactivated vaccines eliminate any risk of the pathogen reverting to a disease-causing form, making them ideal for individuals with compromised immune systems or specific age groups, such as infants and the elderly.
Consider the influenza vaccine, a prime example of inactivated technology. Each year, the World Health Organization selects strains of the influenza virus most likely to circulate globally. These viruses are grown in eggs or cell cultures, then inactivated using formaldehyde. The resulting vaccine, administered as a single 0.5 mL intramuscular dose for adults and a lower volume for children, primes the immune system to recognize and combat the virus without exposing the recipient to active infection. This process highlights the precision and safety inherent in inactivated vaccines.
However, the immune response to inactivated vaccines is often less robust than that of live vaccines, necessitating adjuvants—substances like aluminum salts—to enhance immunity. For instance, the hepatitis A vaccine, an inactivated formulation, includes an adjuvant to ensure a strong and lasting immune memory. This combination of killed pathogen and adjuvant underscores the balance between safety and efficacy in vaccine design. It also explains why some inactivated vaccines require multiple doses or booster shots to maintain protection.
Practical considerations for inactivated vaccines include their stability and storage requirements. Unlike live vaccines, which often need refrigeration, inactivated vaccines are generally more heat-stable, making them suitable for distribution in resource-limited settings. For example, the inactivated polio vaccine (IPV) can be stored at 2°C to 8°C but is less susceptible to temperature fluctuations than live oral polio vaccine (OPV). This durability ensures broader accessibility, a critical factor in global immunization campaigns.
In conclusion, inactivated vaccines exemplify the ingenuity of vaccine development, transforming deadly pathogens into safe immunological tools. Their application in preventing diseases like influenza, hepatitis A, and polio demonstrates their versatility and reliability. While they may require adjuvants or multiple doses to optimize immunity, their safety profile and logistical advantages make them indispensable in public health. Understanding their mechanism and practicalities empowers individuals to make informed decisions about vaccination, reinforcing the global effort to control and eradicate infectious diseases.
Effective Tips to Reduce Lumps After Infant Vaccinations Safely
You may want to see also
Explore related products






![]()
Subunit vaccines: Use specific pathogen parts (proteins/sugars) to induce immunity
Subunit vaccines represent a precision approach in immunology, harnessing only the essential components of a pathogen to trigger a targeted immune response. Unlike whole-cell or live-attenuated vaccines, which use entire pathogens, subunit vaccines isolate specific proteins, sugars, or other antigens from the disease-causing organism. This method minimizes the risk of adverse reactions while maximizing efficacy, making it particularly suitable for vulnerable populations, such as the elderly or immunocompromised individuals. For instance, the hepatitis B vaccine contains a single protein, the hepatitis B surface antigen (HBsAg), which is sufficient to confer long-lasting immunity without exposing the recipient to the virus itself.
The development of subunit vaccines involves meticulous identification and extraction of key antigens. Scientists often use recombinant DNA technology to produce these antigens in large quantities, ensuring purity and consistency. For example, the human papillomavirus (HPV) vaccine Gardasil uses virus-like particles (VLPs) composed of the L1 protein, which self-assemble into structures resembling the virus but lack its genetic material. This design elicits a robust immune response without the risk of infection. Such precision engineering underscores the sophistication of subunit vaccines, which often require adjuvants—substances like aluminum salts—to enhance the immune response, as the isolated antigens alone may not be potent enough.
One of the standout advantages of subunit vaccines is their safety profile. By excluding unnecessary pathogen components, they eliminate the possibility of unintended immune reactions or reversion to virulence, a rare but potential risk with live-attenuated vaccines. This makes subunit vaccines ideal for widespread use, including in pediatric populations. The acellular pertussis vaccine, for instance, replaced the whole-cell version in many countries due to its reduced side effects while maintaining protection against whooping cough. However, the trade-off is that subunit vaccines often require multiple doses and booster shots to achieve and sustain immunity, as the immune response may wane over time.
Practical considerations for subunit vaccines include storage and administration. Unlike some live vaccines, which require refrigeration, many subunit vaccines are stable at room temperature, facilitating distribution in resource-limited settings. Dosage varies by vaccine; for example, the HPV vaccine is typically administered in two or three doses over 6–12 months for adolescents aged 9–14, while those aged 15–26 may require three doses. Adherence to the recommended schedule is critical, as incomplete vaccination can compromise immunity. Additionally, healthcare providers should educate recipients about potential mild side effects, such as soreness at the injection site or low-grade fever, which are generally short-lived and manageable.
In conclusion, subunit vaccines exemplify the intersection of precision science and public health, offering a safe and effective means to combat infectious diseases. Their targeted design, coupled with advancements in biotechnology, positions them as a cornerstone of modern vaccination strategies. As research continues to identify novel antigens and improve delivery methods, subunit vaccines will likely play an increasingly vital role in global health initiatives, from eradicating polio to preventing emerging infectious threats. For individuals and communities alike, understanding their mechanisms and benefits empowers informed decision-making in the pursuit of immunity.
Staying Protected: Tdap Vaccine Update Frequency Explained
You may want to see also
Explore related products






![]()
mRNA vaccines: Deliver genetic material to teach cells to produce antigens
MRNA vaccines represent a groundbreaking approach in vaccinology, leveraging the body’s own cellular machinery to mount an immune response. Unlike traditional vaccines that introduce a weakened or inactivated pathogen, mRNA vaccines deliver a genetic blueprint—a strand of messenger RNA (mRNA)—that instructs cells to produce a specific viral protein, typically the spike protein of a virus like SARS-CoV-2. This protein acts as an antigen, triggering the immune system to recognize and combat the actual pathogen if encountered later. The elegance of this method lies in its precision: it targets only the necessary component, avoiding the introduction of any live or dead virus particles.
The process begins with the injection of a lipid nanoparticle encapsulating the mRNA into the deltoid muscle. Once inside muscle cells, the mRNA enters the cytoplasm, where ribosomes read its sequence and synthesize the encoded protein. This protein is then displayed on the cell surface, prompting immune cells to identify it as foreign. B cells produce antibodies, while T cells mount a cellular defense, creating memory cells for long-term immunity. Notably, the mRNA itself does not enter the cell nucleus, ensuring it cannot alter DNA. A standard mRNA vaccine regimen, such as Pfizer-BioNTech’s COVID-19 vaccine, involves two doses of 30 micrograms each, administered 3–4 weeks apart for individuals aged 12 and older, with a lower dose for younger age groups.
One of the most compelling advantages of mRNA vaccines is their rapid development timeline. Traditional vaccines often require years of research and production, but mRNA vaccines can be designed and manufactured within weeks once the genetic sequence of a pathogen is known. This agility was pivotal during the COVID-19 pandemic, enabling vaccines to be deployed in record time. However, this speed does not compromise safety; clinical trials for mRNA vaccines still adhere to rigorous standards, including phases to assess efficacy, safety, and long-term effects.
Despite their promise, mRNA vaccines face practical challenges, particularly in storage and distribution. The mRNA molecules are fragile and degrade at room temperature, necessitating ultra-cold storage conditions (e.g., -70°C for Pfizer’s vaccine). This requirement poses logistical hurdles, especially in low-resource settings. However, ongoing innovations, such as stabilizing formulations and lyophilization (freeze-drying), aim to address these limitations. For recipients, adhering to storage guidelines at vaccination sites and maintaining the cold chain during transport are critical to ensuring vaccine efficacy.
In conclusion, mRNA vaccines exemplify the fusion of molecular biology and immunology, offering a versatile and efficient platform for combating infectious diseases. Their ability to rapidly adapt to new pathogens positions them as a cornerstone of future pandemic preparedness. While logistical challenges remain, continued research and technological advancements will likely mitigate these barriers, solidifying mRNA vaccines as a transformative tool in global health. For individuals, understanding their mechanism and following vaccination protocols ensures optimal protection, underscoring the importance of this innovative approach in modern medicine.
Who Benefits from Testing Unapproved Vaccines on Foster Children?
You may want to see also
Explore related products






![]()
Viral vector vaccines: Modified viruses deliver pathogen genes to elicit immune response
Viruses, nature’s own gene delivery systems, form the backbone of viral vector vaccines. These vaccines repurpose harmless viruses (vectors) to ferry genetic material from a target pathogen into human cells, triggering an immune response without causing disease. Unlike traditional vaccines that use weakened or inactivated pathogens, viral vectors act as molecular taxis, ensuring precise delivery of antigen blueprints directly to the cell’s protein-making machinery. This method mimics natural infection more closely than subunit or conjugate vaccines, often eliciting robust cellular and humoral immunity.
Consider the Johnson & Johnson COVID-19 vaccine, a prime example of this technology. It employs a modified adenovirus (Ad26) to deliver the SARS-CoV-2 spike protein gene. Once injected, the vector enters cells, releases the gene, and prompts the production of spike proteins. The immune system recognizes these foreign proteins, mounts a defense, and retains memory for future encounters. A single 0.5 mL dose, administered intramuscularly to individuals aged 18 and older, offers protection with fewer logistical hurdles than mRNA vaccines, as it requires standard refrigeration (2–8°C) and provides durable immunity.
However, viral vector vaccines are not without challenges. Pre-existing immunity to the vector—common with adenoviruses, which cause mild respiratory infections—can neutralize the vaccine before it delivers its payload, reducing efficacy. To mitigate this, researchers select rare serotypes (like Ad26) or engineer vectors to evade immune detection. Additionally, while rare, cases of vaccine-induced immune thrombotic thrombocytopenia (VITT) have been linked to adenovirus-based COVID-19 vaccines, prompting careful monitoring, especially in younger populations.
Despite these hurdles, viral vectors offer versatility unmatched by other platforms. They can target diverse pathogens, from Ebola to HIV, and are adaptable for gene therapies. For instance, the Ebola vaccine Ervebo uses a vesicular stomatitis virus (VSV) vector, achieving 97.5% efficacy in clinical trials. Practical tips for recipients include staying hydrated post-vaccination and monitoring for unusual symptoms like persistent headaches or bruising, which should be reported immediately.
In summary, viral vector vaccines represent a fusion of virology and immunology, leveraging nature’s tools to outsmart pathogens. Their ability to induce strong, lasting immunity with a single dose makes them invaluable, particularly in resource-limited settings. Yet, their success hinges on careful vector selection and vigilant safety monitoring. As this technology evolves, it promises to reshape not only vaccinology but also the broader landscape of genetic medicine.
California's Religious Exemption for Vaccines: What's the Law?
You may want to see also
Frequently asked questions
Traditional vaccine development methods include live-attenuated vaccines, where a weakened form of the pathogen is used, and inactivated vaccines, which use killed versions of the disease-causing organism. These methods have been employed for decades and are well-established in vaccine production.
Subunit vaccines are unique as they only contain specific pieces of the pathogen, such as proteins or sugars, instead of the entire organism. This approach allows for a more targeted immune response and is often safer, especially for individuals with weakened immune systems.
mRNA (messenger RNA) vaccines are a newer technology that introduces a piece of genetic material (mRNA) into the body, which instructs cells to produce a harmless protein unique to the virus. This triggers an immune response, preparing the body to fight the actual virus. The mRNA does not affect or interact with our DNA.
Viral vector-based vaccines utilize a modified, harmless virus (the vector) to deliver genetic instructions to our cells, similar to mRNA vaccines. This method teaches our cells to produce a protein that triggers an immune response. It is a versatile approach, allowing for the development of vaccines against various diseases.