In the past, the age at which children received vaccinations varied significantly depending on the specific vaccine, public health policies, and medical advancements of the time. For instance, during the mid-20th century, vaccines like smallpox and diphtheria were often administered in early childhood, sometimes as early as 2 months old, while others, such as the polio vaccine, became widely available in the 1950s and were typically given to children around 5 to 7 years old. The introduction of combination vaccines in the late 20th century streamlined schedules, allowing multiple immunizations to be given during infancy and early childhood. Historical vaccination practices also reflected societal priorities and the availability of medical resources, with some regions prioritizing certain vaccines over others based on local disease prevalence. Understanding these past practices provides valuable context for appreciating the evolution of modern immunization schedules and their role in preventing childhood diseases.
Explore related products






What You'll Learn
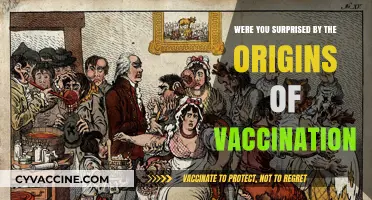
- s-1940s: Smallpox vaccine given at infancy, other vaccines unavailable
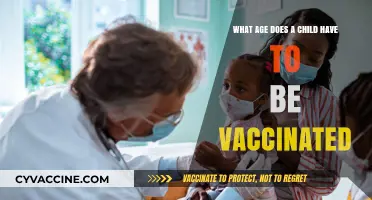
- s: Polio vaccine introduced, children vaccinated around age 5-6
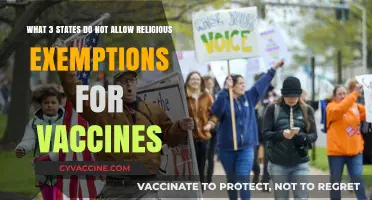
- s: MMR vaccine started, typically given to kids aged 12-15 months
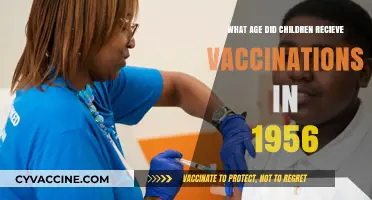
- s-1980s: DTaP vaccine routine, administered to infants at 2, 4, 6 months
- s: Hepatitis B vaccine added, first dose given at birth or 2 months
![]()
1900s-1940s: Smallpox vaccine given at infancy, other vaccines unavailable
In the early 1900s to 1940s, childhood vaccinations were limited in scope compared to modern immunization schedules. The most widely administered vaccine during this period was the smallpox vaccine, which was typically given during infancy. Smallpox, a devastating and often fatal disease, had plagued humanity for centuries, and the vaccine developed by Edward Jenner in the late 18th century remained the primary tool for prevention. Parents were strongly encouraged to have their infants vaccinated shortly after birth to protect them from this highly contagious and deadly virus. This practice was particularly crucial in urban areas where overcrowding and poor sanitation increased the risk of smallpox outbreaks.
The smallpox vaccine was often administered within the first few months of life, usually between 2 and 9 months of age. This early vaccination was essential because smallpox posed a significant threat to young children, who were more likely to suffer severe complications or death if infected. The vaccine was delivered using a bifurcated needle, which was dipped into the vaccine solution and then used to prick the skin, typically on the upper arm. This method, known as scarification, left a distinctive scar that served as a lifelong marker of vaccination. Despite its effectiveness, the smallpox vaccine was not without risks, including localized infections or more severe adverse reactions, though these were rare.
During this era, other vaccines that are now routine in childhood immunization schedules were either unavailable or in the early stages of development. Vaccines for diseases such as diphtheria, tetanus, pertussis, and polio did not become widely accessible until the mid-20th century. As a result, children in the 1900s to 1940s were left vulnerable to these illnesses, which often caused widespread morbidity and mortality. Public health efforts focused primarily on smallpox eradication, with other preventable diseases receiving less attention due to the lack of available vaccines.
The limited availability of vaccines during this period meant that childhood immunization was a far simpler process than it is today. Parents did not have to navigate complex schedules or multiple doses of various vaccines. Instead, their primary concern was ensuring their child received the smallpox vaccine during infancy. This singular focus reflected the medical and scientific limitations of the time, as well as the urgent need to combat smallpox, which remained a significant global health threat until its eventual eradication in 1980.
In summary, the 1900s to 1940s were characterized by the widespread administration of the smallpox vaccine to infants, while other vaccines remained unavailable. This period highlights the evolution of childhood immunization practices and the critical role of early vaccination efforts in combating deadly diseases. The smallpox vaccine's success laid the groundwork for future advancements in vaccine development and public health strategies, ultimately leading to the comprehensive immunization programs we rely on today.
Healthcare Workers in Oregon: Mandatory Vaccination Status
You may want to see also
Explore related products






![]()
1950s: Polio vaccine introduced, children vaccinated around age 5-6
In the 1950s, the introduction of the polio vaccine marked a significant milestone in public health, particularly for children. Developed by Dr. Jonas Salk, the inactivated polio vaccine (IPV) was first made available in 1955, following extensive clinical trials. This breakthrough came at a critical time when polio outbreaks were a widespread fear, causing paralysis and even death, especially among young children. The vaccine's arrival was met with widespread relief and enthusiasm, as it promised to curb the devastating impact of the disease. At this time, the recommended age for children to receive the polio vaccine was around 5 to 6 years old, a decision based on the age group most vulnerable to severe polio infections.
The vaccination process in the 1950s was a communal effort, often conducted in schools or public health clinics. Parents were encouraged to bring their children in for the vaccine, which was typically administered in a series of injections. The age of 5 to 6 was chosen because it coincided with children entering formal schooling, making it logistically easier to vaccinate a large number of children in a controlled setting. Additionally, by this age, children’s immune systems were considered mature enough to respond effectively to the vaccine, providing robust protection against the poliovirus. This age-specific approach ensured that the most at-risk group was prioritized.
Health campaigns during this era played a crucial role in educating parents about the importance of vaccinating their children. Public service announcements, community meetings, and school programs emphasized the life-saving benefits of the polio vaccine. The fear of polio was so pervasive that vaccination rates were high, with many parents eager to protect their children. The success of these campaigns, combined with the vaccine's effectiveness, led to a dramatic decline in polio cases within just a few years of its introduction. By targeting children around the age of 5 to 6, health authorities were able to interrupt the chain of transmission and reduce the disease's prevalence.
The 1950s polio vaccination program also set a precedent for future immunization schedules. It demonstrated the feasibility and importance of vaccinating children at specific ages to maximize protection. The age of 5 to 6 became a benchmark for other vaccines, as it balanced the developmental stage of the child with the urgency of disease prevention. This approach not only saved countless lives but also paved the way for the development and distribution of other childhood vaccines in subsequent decades. The polio vaccine's introduction remains a testament to the power of scientific innovation and public health initiatives.
In retrospect, the decision to vaccinate children around the age of 5 to 6 in the 1950s was a strategic and effective response to the polio epidemic. It reflected an understanding of the disease's epidemiology and the practicalities of mass vaccination. The success of this program not only eradicated polio as a major public health threat in many parts of the world but also established a framework for childhood immunization that continues to protect generations of children. The legacy of the 1950s polio vaccine underscores the importance of timely and targeted vaccination efforts in safeguarding public health.
Virginia's Vaccination Laws: Philosophical Exemptions Allowed or Not?
You may want to see also
Explore related products






![]()
1960s: MMR vaccine started, typically given to kids aged 12-15 months
The 1960s marked a significant milestone in pediatric vaccination with the introduction of the Measles, Mumps, and Rubella (MMR) vaccine. This combination vaccine was developed to protect children against three highly contagious diseases that were once common and often severe. The MMR vaccine was a groundbreaking advancement, as it streamlined the immunization process by combining protection against multiple diseases into a single shot. This innovation not only simplified vaccination schedules but also improved compliance, ensuring more children received timely protection.
During the 1960s, the MMR vaccine was typically administered to children between the ages of 12 and 15 months. This age range was chosen based on medical research indicating that a child’s immune system is sufficiently developed by this time to mount an effective response to the vaccine. Additionally, this age window minimized the risk of interference from maternal antibodies, which could reduce the vaccine’s efficacy if given too early. The 12- to 15-month mark also aligned with other routine childhood vaccinations, making it a practical and efficient time for parents to bring their children in for immunizations.
The introduction of the MMR vaccine had a profound impact on public health. Measles, mumps, and rubella were once widespread and could lead to serious complications, including encephalitis, deafness, and birth defects if contracted during pregnancy. By vaccinating children at 12 to 15 months, health authorities aimed to create herd immunity and reduce the overall prevalence of these diseases. This strategy proved highly effective, leading to a dramatic decline in cases and hospitalizations related to these illnesses.
Parents in the 1960s were encouraged to adhere to the recommended vaccination schedule, which included the MMR vaccine as a critical component. Pediatricians played a key role in educating families about the importance of timely immunization and addressing any concerns about vaccine safety. The success of the MMR vaccine during this period laid the foundation for modern vaccination practices and highlighted the importance of early childhood immunizations in preventing disease.
By the end of the 1960s, the MMR vaccine had become a standard part of childhood vaccination programs in many countries. Its introduction at 12 to 15 months of age was a testament to the progress of medical science and its commitment to protecting children from preventable diseases. This era not only transformed pediatric healthcare but also set a precedent for the development and implementation of future combination vaccines, further simplifying and enhancing childhood immunization efforts.
Experimental Drugs in Vaccines: Government Conspiracy or Myth?
You may want to see also
Explore related products






![]()
1970s-1980s: DTaP vaccine routine, administered to infants at 2, 4, 6 months
In the 1970s and 1980s, the DTaP vaccine, which protects against diphtheria, tetanus, and pertussis (whooping cough), became a cornerstone of childhood immunization schedules. This period marked a significant shift in public health strategies, as medical professionals and health organizations emphasized the importance of early vaccination to prevent these potentially life-threatening diseases. The routine administration of the DTaP vaccine to infants at 2, 4, and 6 months of age was a standard practice during this time, ensuring that children received critical protection during their most vulnerable early months. This schedule was designed to build immunity gradually, with each dose reinforcing the immune response to provide robust protection.
The choice of administering the DTaP vaccine at 2, 4, and 6 months was based on scientific research and clinical trials that demonstrated the safety and efficacy of this timing. Infants at these ages were found to respond well to the vaccine, developing sufficient antibodies to combat the targeted diseases. The 2-month dose served as the initial introduction of the antigens, the 4-month dose boosted the immune response, and the 6-month dose provided long-lasting immunity. This staggered approach allowed the infant’s immature immune system to process the vaccine effectively while minimizing the risk of adverse reactions.
Parents in the 1970s and 1980s were encouraged to adhere strictly to this vaccination schedule, as deviations could compromise the effectiveness of the immunization. Pediatricians and public health campaigns played a crucial role in educating families about the importance of timely vaccinations. The DTaP vaccine was typically administered during routine well-baby visits, which also allowed healthcare providers to monitor the child’s overall growth and development. This integration of vaccination into regular pediatric care ensured high compliance rates and contributed to the decline of diphtheria, tetanus, and pertussis cases in many regions.
Despite its success, the DTaP vaccine schedule of the 1970s and 1980s was not without challenges. Some parents had concerns about vaccine safety, and misconceptions about potential side effects occasionally led to hesitancy. However, extensive data from this period consistently showed that the benefits of vaccination far outweighed the risks. Mild side effects, such as fever or soreness at the injection site, were common but transient, and severe reactions were extremely rare. Public health initiatives worked to address these concerns through transparent communication and evidence-based information.
By the end of the 1980s, the DTaP vaccine routine had become a well-established practice, significantly reducing the incidence of diphtheria, tetanus, and pertussis in childhood populations. This era laid the groundwork for modern vaccination schedules, which continue to prioritize early immunization to protect infants from preventable diseases. The success of the DTaP vaccine during this time underscores the importance of consistent, evidence-based public health strategies in safeguarding community health.
Puppy Vaccination Schedule: Essential Months for Your Pup's Health
You may want to see also
Explore related products






![]()
1990s: Hepatitis B vaccine added, first dose given at birth or 2 months
In the 1990s, a significant shift occurred in childhood vaccination schedules with the introduction of the Hepatitis B vaccine, marking a crucial step in preventing a potentially life-threatening liver infection. This decade saw the implementation of a new strategy to protect infants from Hepatitis B, a disease primarily transmitted through infected bodily fluids, including blood and semen. The recommendation was clear: administer the first dose of the Hepatitis B vaccine at birth or within the first two months of life. This early intervention was a proactive measure to ensure newborns were safeguarded during their most vulnerable period.
The addition of the Hepatitis B vaccine to the childhood immunization schedule was a response to the growing recognition of the disease's impact on public health. Hepatitis B can lead to chronic liver problems, including cirrhosis and liver cancer, and young children are particularly susceptible to these long-term complications. By vaccinating infants, health authorities aimed to provide long-lasting immunity and reduce the risk of infection during childhood and beyond. This approach was especially important given the often asymptomatic nature of Hepatitis B in children, making early prevention through vaccination a critical strategy.
The 1990s' vaccination protocol for Hepatitis B typically involved a series of three shots. After the initial dose at birth or 2 months, the second dose was administered one to two months later, followed by a third dose at 6 months of age. This schedule ensured the development of a robust immune response, offering protection against Hepatitis B for years to come. The timing of these doses was carefully planned to coincide with other routine childhood vaccinations, making it convenient for parents and healthcare providers to ensure children received all necessary immunizations.
This new vaccination practice had a profound impact on public health. It not only reduced the incidence of Hepatitis B in children but also contributed to a decline in the overall prevalence of the disease. The success of this strategy led to its widespread adoption, and today, the Hepatitis B vaccine is a standard component of infant immunization programs worldwide. The 1990s' initiative to vaccinate newborns against Hepatitis B is a testament to the power of preventive medicine and its ability to shape healthier futures for generations to come.
Furthermore, the introduction of the Hepatitis B vaccine at birth or 2 months of age highlighted the evolving nature of vaccination schedules. It demonstrated how medical advancements and a deeper understanding of diseases can lead to timely interventions, ensuring children are protected from an early age. This period in the history of vaccinations underscores the importance of staying abreast of medical research and adapting immunization practices to provide the best possible care for children.
Delta Variant Origins: Vaccine Connection or Natural Evolution?
You may want to see also
Frequently asked questions
In the early 20th century, children often received their first vaccinations, such as smallpox and diphtheria, between 1 and 2 years of age, though this varied by region and availability of vaccines.
In the 1950s, children were typically vaccinated against polio between the ages of 2 and 5, with the introduction of the inactivated polio vaccine (IPV) in 1955 and the oral polio vaccine (OPV) shortly after.
Routine childhood vaccination schedules began to standardize in the 1960s and 1970s, with most children receiving vaccines like DTP (diphtheria, tetanus, pertussis) and MMR (measles, mumps, rubella) starting at 2 months of age, following a series of doses through early childhood.