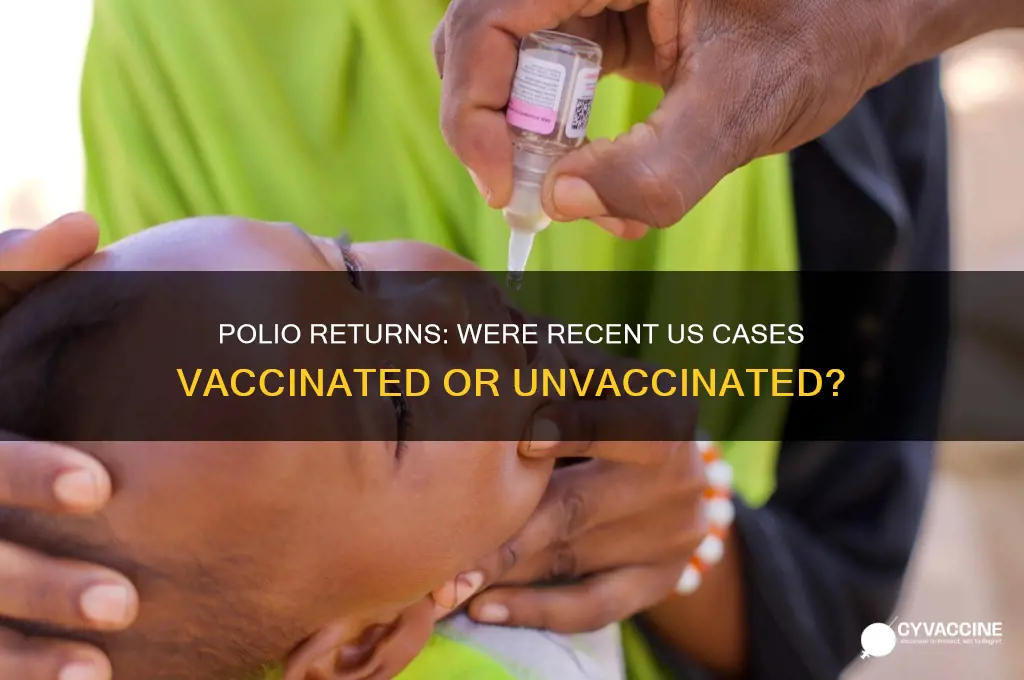
The recent cases of polio in the USA have sparked significant concern and raised questions about vaccination status. In 2022, an unvaccinated individual in New York was confirmed to have paralytic polio, marking the first such case in the U.S. in nearly a decade. Subsequent investigations revealed that the virus had been circulating in the community, with wastewater samples testing positive in multiple counties. While the majority of the population is vaccinated against polio due to widespread immunization efforts, these cases highlight the importance of maintaining high vaccination rates to prevent outbreaks, especially in areas with lower vaccine coverage. Public health officials emphasize that vaccination remains the most effective way to protect against polio, as the disease can cause severe paralysis and even death in rare cases.
Explore related products


$15.86 $19.99




What You'll Learn
![]()
Vaccination status of affected individuals
The recent cases of polio in the United States have raised important questions about the vaccination status of the affected individuals. Polio, a highly contagious disease caused by the poliovirus, has been largely eradicated in many parts of the world due to widespread vaccination efforts. However, the emergence of new cases in the U.S. highlights the importance of understanding whether these individuals were vaccinated and, if not, the reasons behind their unvaccinated status.
In the case of the 2022 polio outbreak in New York, health officials confirmed that the individual who tested positive for paralytic polio was unvaccinated. This case marked the first instance of polio-related paralysis in the U.S. in nearly a decade. The individual had not received the polio vaccine, which is typically administered as part of the childhood immunization schedule. This highlights a critical issue: unvaccinated individuals remain at significant risk of contracting polio, especially in areas where the virus may still circulate, even if rarely.
Further investigation into the outbreak revealed that the virus had been circulating in the community for some time, as evidenced by the detection of poliovirus in wastewater samples. This suggests that other unvaccinated individuals in the area may have been exposed and asymptomatically shed the virus. While most people infected with poliovirus do not develop symptoms, those who are unvaccinated are at higher risk of severe complications, including paralysis. This underscores the importance of maintaining high vaccination rates to protect both individuals and communities.
Another aspect to consider is the vaccination status of close contacts of the affected individual. Health officials in New York worked to identify and vaccinate unvaccinated individuals in the community to prevent further spread. This response included targeted vaccination campaigns and public health messaging to emphasize the importance of polio immunization. The fact that the virus was detected in wastewater but only one case of paralysis was reported suggests that many individuals in the community were likely protected by vaccination, preventing widespread disease.
The recent polio cases also bring attention to vaccine hesitancy and access issues. While the polio vaccine has been widely available in the U.S. for decades, some individuals or communities may remain unvaccinated due to misinformation, lack of access to healthcare, or personal beliefs. Addressing these barriers is crucial to ensuring that polio does not re-establish itself in the U.S. Public health efforts must focus on education, improving vaccine accessibility, and rebuilding trust in immunization programs to protect vulnerable populations.
In summary, the vaccination status of individuals affected by recent polio cases in the U.S. reveals a clear pattern: those who were unvaccinated were at higher risk of severe disease. The New York outbreak serves as a reminder of the critical role vaccination plays in preventing polio and the need for continued vigilance in maintaining high immunization rates. By understanding and addressing the reasons behind unvaccinated status, public health officials can work to eliminate polio once and for all.
Should You Mix Vaccines for Your Booster Shot? Expert Insights
You may want to see also
Explore related products






![]()
Polio vaccine effectiveness in recent cases
The recent cases of polio in the USA have sparked important discussions about vaccine effectiveness and the importance of maintaining high vaccination rates. In 2022, an unvaccinated individual in New York was diagnosed with paralytic polio, marking the first such case in the U.S. in nearly a decade. This incident raised questions about whether the individual had been vaccinated and highlighted the critical role of vaccines in preventing the spread of this highly contagious disease. Investigations revealed that the virus was genetically linked to the oral polio vaccine (OPV), which is no longer used in the U.S. but is still administered in some countries. This suggests the virus likely originated from outside the U.S., emphasizing the global nature of polio prevention efforts.
The polio vaccine has proven to be one of the most effective tools in public health, with two types currently in use: the inactivated polio vaccine (IPV) and the oral polio vaccine (OPV). In the U.S., only IPV is administered, which provides robust protection against paralytic polio but does not prevent asymptomatic infection or the shedding of the virus. This means that while vaccinated individuals are highly unlikely to develop severe disease, they can still carry and transmit the virus, particularly in under-vaccinated communities. The recent case in New York underscores the importance of high vaccination coverage to achieve herd immunity and protect those who cannot be vaccinated due to medical reasons.
Data from the recent U.S. case and global polio surveillance indicate that vaccinated individuals are overwhelmingly protected from severe outcomes. The New York patient, who was unvaccinated, suffered paralysis, while no vaccinated individuals in the surrounding community developed severe disease. This aligns with historical data showing that IPV is 90-100% effective in preventing paralytic polio after the full series of doses. However, the detection of vaccine-derived poliovirus in wastewater samples in New York and other states highlights the risk of outbreaks in areas with low vaccination rates. These findings reinforce the need for continued vaccination efforts to prevent the re-emergence of polio.
The effectiveness of the polio vaccine in recent cases also depends on community vaccination rates. In areas with high coverage, the vaccine not only protects individuals but also limits the virus's ability to circulate. Conversely, pockets of low vaccination leave populations vulnerable to outbreaks, as seen in the 2022 case. Public health officials have responded by urging vaccination and conducting targeted campaigns to increase IPV uptake, particularly in affected communities. This proactive approach is essential to prevent further cases and maintain the U.S.'s polio-free status.
In conclusion, the recent polio cases in the U.S. demonstrate the continued effectiveness of the vaccine in preventing severe disease, but they also highlight gaps in immunity that can allow the virus to spread. The polio vaccine remains a cornerstone of global eradication efforts, and maintaining high vaccination rates is crucial to protect both individuals and communities. These incidents serve as a reminder that vaccination is not just a personal health decision but a collective responsibility to safeguard public health.
IPV vs Polio Vaccine: Understanding the Differences and Similarities
You may want to see also
Explore related products






![]()
Source of polio virus in vaccinated areas
The recent detection of poliovirus in vaccinated areas, particularly in the United States, has raised questions about the source of these infections. While vaccination campaigns have significantly reduced polio cases globally, the virus can still circulate in communities with low vaccination rates or where vaccine efficacy is compromised. In the case of the United States, the poliovirus detected in wastewater and in a few individuals was genetically linked to the oral polio vaccine (OPV), which is no longer used in the country. This suggests that the virus likely originated from regions where OPV is still administered, highlighting the global interconnectedness of polio transmission.
One primary source of the poliovirus in vaccinated areas is vaccine-derived poliovirus (VDPV). VDPVs emerge when the weakened virus in OPV mutates over time in under-immunized populations. These mutated viruses can regain the ability to cause paralysis and spread in communities with low vaccination coverage. Since OPV is used in many low- and middle-income countries, international travel or migration can introduce VDPVs into regions that exclusively use the inactivated polio vaccine (IPV), such as the United States. This underscores the importance of maintaining high vaccination rates globally to prevent the spread of VDPVs.
Another potential source is importation through travel. Individuals from countries where polio is endemic or where OPV is used can unknowingly carry the virus to vaccinated regions. Even if the local population is vaccinated, the virus can still circulate in the environment, as evidenced by its detection in wastewater samples. This highlights the need for robust surveillance systems to monitor poliovirus activity, even in areas considered polio-free. Public health officials must remain vigilant and ensure that travelers from high-risk regions are up to date on their vaccinations.
Undervaccinated or unvaccinated pockets within vaccinated areas also pose a risk. Despite high overall vaccination rates in the United States, some communities have lower immunization coverage due to vaccine hesitancy, access barriers, or misinformation. These pockets can serve as reservoirs for the poliovirus, allowing it to persist and potentially spread. Strengthening local vaccination efforts and addressing vaccine hesitancy are critical to eliminating these vulnerabilities. Public health campaigns must emphasize the importance of herd immunity and the role of individual vaccination in protecting communities.
Finally, environmental factors play a role in the persistence and transmission of the poliovirus. The virus can survive in wastewater and other environmental reservoirs, particularly in areas with poor sanitation. Even in vaccinated regions, the presence of the virus in the environment can pose a risk if it comes into contact with undervaccinated individuals. Regular environmental monitoring and improvements in sanitation infrastructure are essential to mitigate this risk. Collaborative global efforts, such as the Global Polio Eradication Initiative, are vital to ensuring that the poliovirus is eliminated worldwide, thereby protecting vaccinated regions from imported cases.
In conclusion, the source of poliovirus in vaccinated areas, such as the United States, is multifaceted and often linked to global polio dynamics. Vaccine-derived polioviruses, importation through travel, undervaccinated communities, and environmental reservoirs all contribute to the persistence of the virus. Addressing these challenges requires a combination of global vaccination efforts, robust surveillance, and local public health interventions to ensure that polio remains eradicated in regions where it no longer circulates.
Unvaccinated Children in Schools: Legal Rights and Health Concerns Explained
You may want to see also
Explore related products





![]()
Role of vaccine hesitancy in outbreaks
The recent cases of polio in the USA have sparked important discussions about the role of vaccine hesitancy in disease outbreaks. According to various sources, including the Centers for Disease Control and Prevention (CDC), the individual who contracted polio in New York in 2022 was unvaccinated. This case highlights a critical issue: vaccine hesitancy can create pockets of vulnerability within communities, allowing diseases that were once nearly eradicated to re-emerge. Polio, a highly infectious disease that can cause paralysis and even death, was on the brink of global eradication due to widespread vaccination efforts. However, declining vaccination rates in certain areas have provided an opportunity for the virus to circulate, posing a risk not only to unvaccinated individuals but also to those who cannot be vaccinated due to medical reasons.
Vaccine hesitancy, defined as the delay in acceptance or refusal of vaccines despite availability, plays a significant role in the resurgence of preventable diseases like polio. In the case of the New York polio outbreak, the virus was genetically linked to the oral polio vaccine (OPV) used in other countries, suggesting it originated from an individual who had received the vaccine and traveled to the area. While OPV is highly effective, it can, in rare cases, revert to a form that can cause infection in under-vaccinated communities. This underscores the importance of maintaining high vaccination coverage to prevent such outbreaks. When vaccination rates drop, even a single case can quickly spread, particularly in areas with low herd immunity. The role of vaccine hesitancy here is clear: it weakens the collective protection that vaccines provide, leaving communities susceptible to outbreaks.
The impact of vaccine hesitancy extends beyond individual health, affecting public health systems and global eradication efforts. Polio eradication has been a priority for decades, with significant resources invested in vaccination campaigns worldwide. However, localized outbreaks in areas with low vaccination rates can derail progress. For instance, the detection of poliovirus in wastewater samples in New York and other states indicates community spread, likely fueled by low vaccination coverage in certain populations. This not only poses a risk to local communities but also threatens global health security, as the virus can spread across borders. Addressing vaccine hesitancy is therefore crucial to sustaining the gains made in disease control and prevention.
Misinformation and distrust in vaccines are key drivers of hesitancy, particularly in the context of polio. False claims about vaccine safety and efficacy have circulated widely, contributing to declining vaccination rates in some communities. In the case of polio, the shift from OPV to the inactivated polio vaccine (IPV) in many countries, including the USA, was driven by safety concerns. However, this transition has been misunderstood by some, leading to unfounded fears about vaccine safety. Public health officials must combat misinformation through transparent communication, community engagement, and education to rebuild trust in vaccines. Without addressing these root causes of hesitancy, outbreaks like the one in New York will continue to occur, undermining efforts to control and eradicate diseases.
Ultimately, the role of vaccine hesitancy in outbreaks like the recent polio cases in the USA cannot be overstated. It serves as a stark reminder of the importance of maintaining high vaccination coverage to protect both individuals and communities. Public health strategies must focus on understanding and addressing the underlying reasons for hesitancy, from misinformation to systemic barriers to access. Strengthening vaccine confidence through evidence-based communication and community-centered approaches is essential to prevent future outbreaks. The fight against polio and other vaccine-preventable diseases is far from over, and overcoming vaccine hesitancy is a critical step in ensuring a healthier, more resilient future.
Whooping Cough Vaccine: Is It Covered by Medicare?
You may want to see also
Explore related products






![]()
Comparison of vaccinated vs. unvaccinated cases
The recent cases of polio in the USA have sparked important discussions about vaccination status and its role in disease prevention. A comparison of vaccinated versus unvaccinated cases reveals significant insights into the effectiveness of polio vaccines and the risks associated with remaining unvaccinated. According to public health reports, the majority of recent polio cases in the USA have occurred in individuals who were either unvaccinated or under-vaccinated. This aligns with global data, which consistently shows that polio outbreaks predominantly affect communities with low vaccination rates. Vaccinated individuals, on the other hand, have demonstrated a high level of protection against the disease, with only rare instances of breakthrough infections reported.
One key aspect of the comparison is the severity of symptoms and outcomes between vaccinated and unvaccinated individuals. Unvaccinated cases tend to experience more severe symptoms, including paralysis, which is the most debilitating complication of polio. In contrast, vaccinated individuals who contract the virus typically exhibit milder symptoms or remain asymptomatic. This disparity underscores the vaccine's ability not only to prevent infection but also to reduce the severity of the disease if infection does occur. The oral polio vaccine (OPV) and the inactivated polio vaccine (IPV) have proven to be highly effective in preventing paralytic polio, further emphasizing the importance of full vaccination.
Another critical point in the comparison is the role of herd immunity and its impact on both vaccinated and unvaccinated populations. Herd immunity, achieved through high vaccination rates, protects those who cannot be vaccinated due to medical reasons or are too young to receive the vaccine. However, when vaccination rates drop, herd immunity weakens, leaving unvaccinated individuals at higher risk of contracting polio. Recent cases in the USA highlight the consequences of vaccine hesitancy and misinformation, as communities with lower vaccination rates have seen a resurgence of the disease. Vaccinated individuals, while protected, are also affected by this trend, as the risk of outbreaks increases in under-vaccinated areas.
Furthermore, the comparison extends to the long-term implications for public health. Unvaccinated cases contribute to the continued circulation of the poliovirus, posing a threat to global eradication efforts. The USA, having been declared polio-free since 1979, now faces the challenge of preventing further spread due to these recent cases. Vaccinated populations play a crucial role in maintaining the progress made toward eradication by reducing the virus's transmission potential. Public health officials stress that achieving and maintaining high vaccination coverage is essential to prevent future outbreaks and protect both vaccinated and unvaccinated individuals.
In conclusion, the comparison of vaccinated versus unvaccinated cases in the recent polio incidents in the USA clearly demonstrates the critical importance of vaccination. Vaccinated individuals benefit from robust protection against infection and severe disease, while unvaccinated individuals face significantly higher risks. The resurgence of polio in under-vaccinated communities serves as a stark reminder of the ongoing need for vaccination to safeguard public health. Strengthening vaccination efforts and addressing vaccine hesitancy are essential steps to prevent further cases and move closer to the global goal of polio eradication.
Update Passport Number in Vaccination Certificate: A Step-by-Step Guide
You may want to see also
Frequently asked questions
No, the recent cases of polio in the USA were in individuals who were unvaccinated or had not completed their full vaccination series.
While rare, vaccinated individuals can still contract polio, but the vaccine provides strong protection, significantly reducing the risk of paralysis and severe disease.
No, the recent cases were caused by circulating vaccine-derived poliovirus (cVDPV), which can emerge in under-vaccinated communities, not from the inactivated polio vaccine (IPV) used in the USA.
The polio vaccine did not fail; the cases occurred in unvaccinated individuals. The vaccine remains highly effective in preventing polio when administered as recommended.
No, vaccinated individuals are not contributing to the spread of polio. The spread is primarily occurring in under-vaccinated or unvaccinated populations where the virus can circulate and mutate.